4231342
| Questão | Responda |
| What are the two most common injectable General anaesthetics? | Propofol Thiopental |
| How is propofol introduced to the system? What are its benefits? | By IV non-irritant Rapid metabolism and distribution - very little time spent in excitement phase. |
| What are the 2 cons of propofol? | Expensive Cardiovascular depressant |
| What is propofol usually used for? | Used for induction into surgery |
| Through which receptors does propofol work? | GABAa and GlyR potentiation |
| What class of drugs is Thiopental? | Barbiturate |
| Where/how does thiopental act? | GABAa Receptors |
| What is the lipid solubility of thiopental and what does this mean in terms of plasma concentration? | High lipid solubility - plasma solubility rapidly declines as drug is stored in body fats |
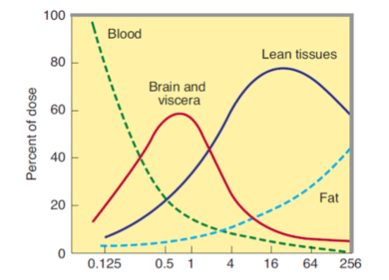
| What are the four main sites of action of barbiturates and in what order are the most rapidly distributed? | 1) Brain 2)Heart, lungs, liver & kidney 3)Muscle and fat (stored) 4)Liver metabolism |
| Explain these graphs | 1) Blood plasma levels rapidly decrease due to absorption of drug by tissues 2) Brain and viscera levels rapidly rise and decrease due to being well vascularised 3)Levels in lean tissue stay high 4) Drug stored in fat |
| Explain the 'hangover' effect of drugs such as thiopental | Anaesthetic is stored in fat and slowly released - not enough to cause general anaesthesia but enough to make patient feel groggy |
| How can thiopental cause death? | If the metabolism becomes saturated - if another dose is then given this can further activate GABAa receptors without the presence of GABA (thiopental is a barbiturate) |
| What are 'dissociative' anaesthetics? | Anaesthetics which cause a dissociation between mind and body |
| Give an example of dissociative anaesthetic | Ketamine |
| What are the advantages of dissociative anaesthetics? (4) | 1) High therapeutic index 2) No cardiovascular or respiratory depression 3)Non-cumulative effect 4)Analgesic |
| What are the disadvantages of dissociative anaesthetics? (2) | 1) Psychic disturbances 2) Involuntary movements |
| Which part of the population is ketamine most used in as an anaesthetic? | Children |
| What flows in through an NMDA receptor and what flows out? | Ca2+ and Na+ flow in K+ flows out |
| How does ketamine affect the NMDA receptor? What class of anatgonist is it? | Binds to the inside of the pore - non-competitive antagonist |
| Where does Etomidiate act and what is it's main side effect? | GABAa potentiator, high incidence of nausea |
| What type of drug is Midazolam? What is it used for? | Benzodiazepine - used as a pre operative sedative or if full anaesthetic not required |
| What type of drug is Alfaxalone? Where does it act and what is it used for? | Neurosteroid, GABAa potentiator, vet anaesthetic |
| What are the advantages of injectable anaesthetics? (2) | 1) Easy to administer 2) Rapid induction |
| What are the three disadvantages of injectable anaesthetics? | 1) Complex pharmacokinetics 2) Slow elimination 3) Side effect |
| What are the two subtypes of inhalation anaesthetics? | Gases Volatile liquid |
| Give an example of a gas and volatile liquid anaesthetic | N20 Desflurane |
| What is the route inhalation anaesthetics take to reach the brain? Why is induction slower than with injectable anaesthetics? | Air>lungs>blood>brain Injectable goes straight to blood. |
| What are the four things which determine the induction rate of an inhalation anaesthetic? | 1) Blood:gas partition coefficient 2) Oil:gas partition coefficient 3) Alveolar ventilation rate 4) Cardiac out out |
| What does the blood:gas partition coefficient determine? | How quickly/well a gas dissolves into the blood. |
| What is and what does the oil:gas partition coefficient determine? | 1) solubility of gas in fat 2) how long the anaesthetic takes to have an effect |
| What does the alveolar ventilation rate determine? | How quickly the gas gets into the blood and round the body |
| Why are the factor that govern the induction rate the same as those which govern the recovery rate for inhalation anaesthetics? | Gases are breathed out - not metabolised |
| Which 3 factors govern only the speed of induction? | 1) blood volume >> alveolar air space 2) Conc of anaesthetic in alveolae initially << inspired air 3)Brain in rapid equilibrium with blood |
| What is more desirable: A high blood:gas coefficient (rapid absorption) or a low blood:gas coefficient? Why? | Low - allows build up of anaesthetic in lungs, blood passing receives continual anaesthetic >>> steady state. Otherwise small volumes of blood receive all anaesthetic and remove it from lungs. |
| What are the blood:gas coefficients of: Ether Halothane Nitrous Oxide Desflurane | 1) 12 2) 2.4 3) 0.5 4) 0.4 |
| Do you want the oil:gas coefficient to be low or high? | High. Determines strength of anaesthetic. |
| Which anaesthetic has the best relationship between oil:gas partition coefficient and blood:gas coefficient? | Desflurane. (O:G = 23, B:G = 0.4) |
| What would you use for... rapid induction? (2) | Propofol, Thiopental |
| Maintenence of anaesthetia? (3) | Desflurane, isoflurane, nitrous oxide |
| Analgesic supplement? | Opioid |
| Muscle relaxant | NMJ blocking agent - eg atracurium |
| Muscarinic antagonist | Atropine |
| Antiemetic (anti-nausea) | Ondasetron |
{kind=link}
Quer criar seus próprios Flashcards gratuitos com GoConqr? Saiba mais.