5480909
Descrição
FlashCards por olimcconnell, atualizado more than 1 year ago
|
|
Criado por olimcconnell
mais de 8 anos atrás
|
|
| Questão | Responda |
| Definitions of abnormality Statistical infrequency | Abnormality is defined as those behaviours that are extremely rare, i.e. any behaviour that is found in very few people is regarded as abnormal "A person’s trait, thinking or behaviour would be considered to be an indication of abnormality if it was found to be numerically (statistically) rare/uncommon/anomalous " |
| Statistical infrequency (EVALUATION) | 1. Some abnormal behaviour is desirable, i.e. IQ, a high IQ would be desirable and is associated with intelligence 2. Depression is present in 27% of the elderly, this means it is common, but it is still clearly an issue (NIMH, 2001) 3. Statistics enable a cut-off point, however it is subjective since different attitudes like amount of sleep are ambiguous |
| Definitions of abnormality Deviation from social norms | Abnormal behaviour is seen as a deviation from unstated rules about how one is 'ought' to behave, any violation is abnormal "Behaviour is classified as abnormal if it violates the social norms and behaviour in a particular social group. Their behaviour may be incomprehensible to others or make others feel threatened or uncomfortable since it is a comprehension to the norm" |
| Deviation from social norms (EVALUATION) | 1. Historical validity, example of fascists states i.e. Russia, Germany in WW1, also homosexuality. Non-Conformists = excluded (Szasz) 2. Cultural variations, different context for example: Tribes, hallucinations and screaming. 3. Does distinguish between desirable and undesirable, also the effect on others. Definition clearly shows transgression |
| Definitions of abnormality Failure to function adequately | People are judged on their ability to go about daily life. If they can't do this and are also experiencing distress then it is considered a sign of abnormality " A person is considered abnormal if they are unable to cope with the demands of everyday life e.g. self-care, hold down a job, interact meaningfully with others, make themselves understood etc. This causes distress to the individual and others" Assessment use of WHODAS |
| Failure to function adequately (EVALUATION) | 1. Needs someone to assess the mental state, ambiguous due to state awareness, i.e. may not be an issue to the person 2. Some dysfunctions can be adaptive and functional, eating orders = attention which is rewarding 3. Subjective from patients point of view, because of WHODAS, however demand characteristics |
| Definitions of abnormality Deviation from ideal mental health | Abnormality is defined in terms of mental health, behaviours that are associated with competence and happiness, Ideal mental health would include a positive mental attitude towards self image, resistance to stress and an accurate perception of reality |
| Deviation from ideal mental health Jahoda | Proposed by Jahoda, the definition looks at positives over negatives - the idea of mental health rather than illness 6 major criteria Self attitudes (esteem) Personal growth (development) Integration (stress) Autonomy (independence) Perception of reality (accuracy) Mastery of environment (control) An absence of the criteria = mental disorder |
| Deviation from ideal mental health (EVALUATION) | 1. Unrealistic criteria, if the criteria of Jahoda were true, the majority of us would be considered abnormal, also quite difficult to measure 2. Suggests mental health is the same as physical health when physical are easy to diagnose and detect 3. Is a positive approach focusing on positives over negatives therefore correlate with 'positive psychology' with positive effects |
| Mental Disorders | Phobias Depression OCD |
| Phobias | A group of mental disorders characterised by high levels of anxiety in response to a particular stimulus or group of stimuli. The anxiety interferes with normal living Instances of irrational fear that produce conscious avoidance of the feared object or situation |
| Phobias Emotional Characteristics | Fear Anxiety Panic |
| Phobias Behavioural Characteristics | Avoidance Fainting Freezing |
| Phobias Cognitive Characteristics | Irrational thinking Unreasonableness which is recognised |
| Depression | A mood disorder where an individual feels sad and/or lacks interest in their usual activities. Further characteristics include irrational negative thoughts, raised or lowered activity levels and difficulties with eating, sleeping and concentration Persistent depressive = long term/recurring |
| Depression Emotional Characteristics | Negative emotions Sadness Loss of interest Sometimes anger |
| Depression Behavioural Characteristics | Reduced or increased energy Reduced or increased sleeping Reduced or increased eating |
| Depression Cognitive Characteristics | Irrational negative thoughts Self beliefs which are self-fufilling |
| OCD | An anxiety disorder where anxiety arises from both obsessions (persistent thoughts) and compulsions (repeated behaviours). Compulsions are the response of obsessions, and the sufferer believes the compulsions will reduce anxiety |
| OCD Emotional Characteristics | Anxiety Distress Awareness of dramatisation Shame |
| OCD Behavioural Characteristics | Compulsions to counter obsessions No connection in a realistic way |
| OCD Cognitive Characteristics | Recurrent, intrusive thoughts More than average worries |
| Behavioural approach to explaining Phobias | Two-Process model: A theory that explains the two processes that lead to the development of phobias, begin by classical conditioning then maintained by operant conditioning Mowrer |
| Two process model Classical conditioning: Initiation | A phobia is acquired through association Involves pairing of NS with UCS so that eventually NS becomes the CS, capable of eliciting a CR |
| Classical conditioning (KEY STUDY) | Little Albert, Rayner 1920 Creation of conditioned response to neutral objects and a steel bar to elicit fear, thus associating the loud bang with the neutral objects causing a fear of the controlled response |
| The two-process model Operant conditioning: Maintenance | The phobia is maintained through negative reinforcement which is the avoidance of fear, by avoiding the presence of fear, this reinforces the idea of the phobia |
| Explaining phobias (EVALUATION) | 1. The model ignores cognitive factors, i.e. irrational thoughts could lead to anxiety and may trigger a phobia 2. Social learning ignored, however Bandura finds it is present, Model and buzzer, stimulates pain 3. Importance of classical conditioning: people recall specific incidents, may only relate to some phobias (Sue et al) |
| The behavioural approach Treating Phobias Systematic desensitisation | Systematic De-Sensitisation Counter-conditioning: phobic stimulus associated with new response of relaxation Reciprocal inhibition: the relaxation inhibits the anxiety Relaxation: deep breathing, focus on peace, progressive muscle relaxing Desensitisation hierarchy: from least to most fearful, relaxation practised |
| Systematic De-Sensitisation | Stage 1: Relaxed state incompatible with anxiety Stage 2: Desensitisation hierarchy, gradual anxiety Stage 3: Evoke events & engage relaxation Stage 4: Move to next step Stage 5: Eventual mastery over feared situation |
| Systematic De-Sensitisation (EVALUATION) | 1. Not appropriate for all phobias, especially underlying evolutionary components 2. Effectiveness of SD, evidence from McGrath 75% respond to this treatment 3. Behaviour therapies are quick and require less effort on the patients part, which is effective for children or adults with learning difficulties |
| The behavioural approach Treating Phobias Flooding | Flooding An alternative to gradual progression, one long session with the most feared stimulus. Continues until anxiety subsides, can be in reality or virtual reality |
| Flooding | Step 1: Patient taught to relax Step 2: Patient masters feared situation, that caused phobia |
| Flooding (EVALUATION) | 1. Individual differences, does not work for everyone and quitting only reduces effectiveness 2. Effectiveness is relatively quick, Choy says it is more effective than SD 3. Unethical to cause a traumatic experience |
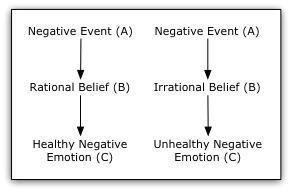
| The cognitive approach to explaining depression | Ellis' ABC model The key is that depression lay in irrational beliefs Model: (Two streams) A refers to activating event B refers to belief, rational or irrational C is the consequence, positive or negative Irrational beliefs, lie with mustabatory thinking, (i.e. i must be liked) which causes depressions and disappointment |
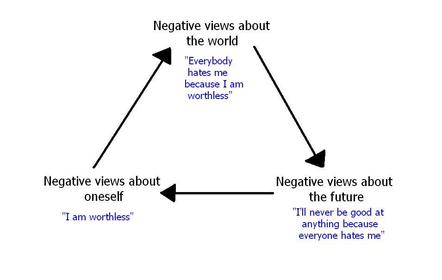
| The cognitive approach to explaining depression | Beck's negative triad Depression is rooted with negative interpretations Negative schema: Develops in childhood, leads to cognitive biases Negative triad: Three key elements, Negative: view on self, view of the world and view of the future |
| ABC Model | |
| Negative triad | |
| The cognitive approach to explaining depression (EVALUATION) | 1. Support for role of irrational thinking, depressed people make more errors, (Hammen) which can lead to depression 2. Blames client, ignores situational factors 3. Many practical application to CBT |
| The cognitive approach to treating depression | Cognitive-Behaviour Therapy (CBT) Ellis develops CBT in the 50's Puts emphasise on irrational thinking as the cause Solves emotional and behavioural problems hence REBT Extension to ABC model: DEF D = disputing thoughts and beliefs E = effects of disputing and attitude F = new feelings produced Homework: trying out new behaviours to test irrational beliefs Behavioural activation: encouraging re-engagement with pleasurable activities Unconditional positive regard: reduces sense of worthlessness |
| The cognitive approach to treating depression (EVALUATION) | 1. Supporting research, Ellis estimated 90% success over 27 sessions 2. Investigator effects, Kuyken and Tsivrikos suggests it may depend on competence of therapist 3. Drug therapy is far easier in time and effort, doesn't require effort from the participant which if failed could increase issue |
| The biological approach in explaining OCD | Genetic explanations COMPT gene: one allele common in OCD which elicits high levels of dopamine SERT gene: one allele common in OCD which elicits low levels of serotonin Diathesis-stress: same genes linked to other disorders, creating vulnerability |
| The biological approach to explaining OCD | Neural explanations Abnormal levels of neurotransmitters, (Dopamine and Serotonin), therefore drug treatments can form round this. Serotonin increase Abnormal brain circuits Damaged caudate nucleus doesn't suppress worry signals from OFC to thalamus |
| The biological approach to explaining OCD (EVALUATION) | 1. Real world application, especially in IVF, parents can see if gene is present 2. Studies show it being present if first relative and twins (5x and meta analysis) 3. Concordance rates are never 100% and do not consider environmental factors |
| The biological approach to treating OCD | Antidepressants SSRIs Tricyclics Anti-Anxiety drugs D-Cycloserine |
| The biological approach to treating OCD | SSRIs prevent re-uptake of serotonin by pre-synaptic nerve Released into a synapse from one nerve Targets receptor cells Re-absorbed by initial neuron Increase levels of serotonin at synapse Increase stimulation |
| The biological approach to treating OCD | Tricyclics Block re-uptake of noradrenaline and serotonin but have more severe side effects Block transporter mechanism More transmitters are left in the synapse Easing transmission of the next impulse |
| The biological approach to treating OCD | BZs Enhancement of GABA, slowing down the nervous system Reacts with special sites Increases flow of chloride ions Harder to stimulate by other ions Causing slowing down and relaxation |
| The biological approach to treating OCD (EVALUATION) | 1. Drug therapies are preferred to other treatments, cheap compared to psychological treatments, also little effort 2. Not a lasting cure, the APA suggest CBT should be trailed first as a lasting cure 3. Side effects of drugs often have negative impacts, SSRIs: headache and insomnia |
{kind=link}
{kind=link}
Quer criar seus próprios Flashcards gratuitos com GoConqr? Saiba mais.