9254677
Descrição
FlashCards por Marissa Alvarez, atualizado more than 1 year ago
|
|
Criado por Marissa Alvarez
aproximadamente 7 anos atrás
|
|
| Questão | Responda |
| Innate Immunity Mechanisms | 1) Mechanical Barriers 2) Soluble Mediators 3) Cellular Defense Mechanisms |
| Innate Immunity Mechanisms Mechanical Barriers/surface secretion: | skin, acidic pH in stomach, cilia |
| Innate Immunity Mechanisms Soluble Mediators | Lysozymes, basic proteins, complement, cytokines |
| Innate Immunity Mechanisms Cellular Defense Mechanisms | natural killer (NK) cells, neutrophils (PMNs), macrophages, mast cells, basophils, eosinophils |
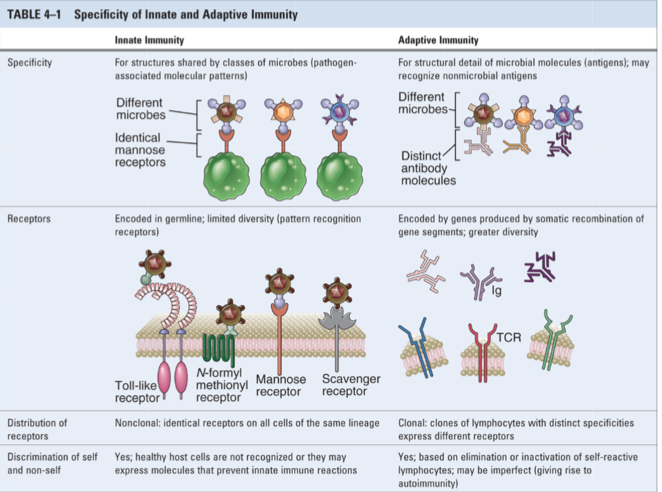
| Compare and contrast: Innate and Adaptive immunity | Innate immunity: not as specific, more broad -coded germ line (the genes code for what is made - no change) -nonclonal: identical receptors on ALL cells Adaptive immunity: more specific, more diversity (somatic gene rearrangements) -clonal: clones of lymphocytes w/distinct specificities express different receptors Both: distinguish between self and non-self peptides -have similar effector mechanisms for killing pathogens |
| Inflammation | an innate response that involves response that involves cellular & physiological elements Can be: 1) Localized: Infection or wounding can trigger: Capillary vasodilation – redness (erythrema) Capillary vasopermeation – swelling (edema) Cellular influx 2) ‘Vasoactive molecules’ (pro-inflammatory) released by white blood cells (WBC) 3) Systemic - Infection ONLY Fever Increase in WBC Changes in serum proteins (e.g., Acute phase proteins) Diagnostic for infection **Excessive inflammation causes immunopathogies -->Critical to the start of the immune response, but if you cannot turn it off then it becomes pathogenic |
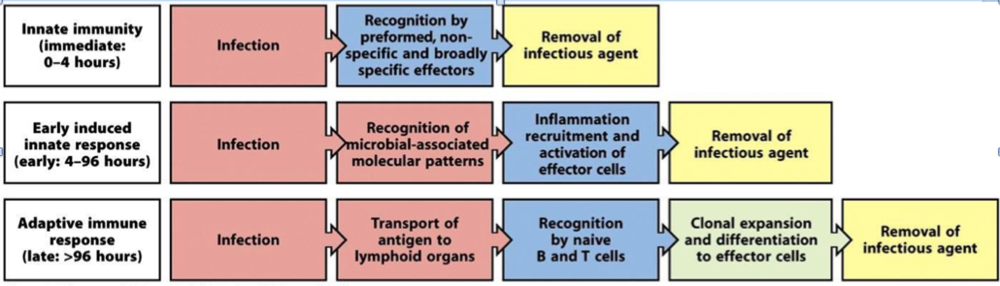
| Buildup of Immunity | |
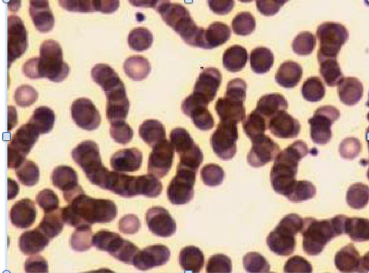
| The Acute Phase Response Black Bile & Medieval Bleeding | Systemic inflammatory response Fever, Changes in “Acute Phase Proteins” e.g., CRP, Complement proteins, plasminogen, fibrinogen, etc. Fibrinogen causes RBCs to stick together to form a Rouleaux (“Ru-Lo”) = “Black bile” Fast sedimentation rate (indicates some kind of septic response) Was bled to cure illness |
| "Danger Signals" activate innate cells | “Danger signals” = PAMPs “Pathogen-associated molecular patterns” -Molecules of pathogens or wounding -General structure/widespread occurrence -Conserved in evolution |
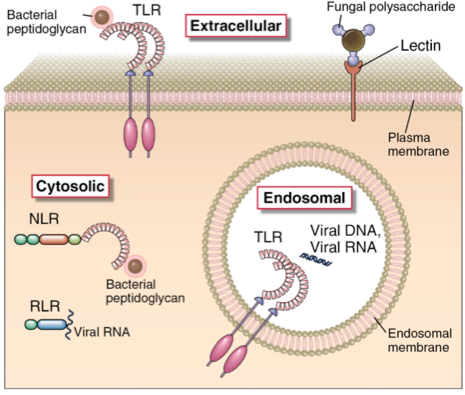
| PAMPS bind to Receptors called PRRs “Pattern Recognition Receptor” | “Pattern Recognition Receptor” (PRRs): Toll-like receptors (TLR) NOD-like receptors (NLR) RIG-like receptors (RLR) Caspase Recruitment Domain (CARD)-containing proteins **Very important to DC (dendritic cell) activation -Upregulates major histocompatibility complex (MHC) (HLA) expression -Allows T-cell activation |
| Some Danger Signals Include | Viral dsRNA Viral ssRNA Bacterial LPS, flagellin, pili Bacteral and fungal cell wall components Microbial polysaccharides Reactive oxygen molecules: H202, OH-, O2- Certain cellular molecules |
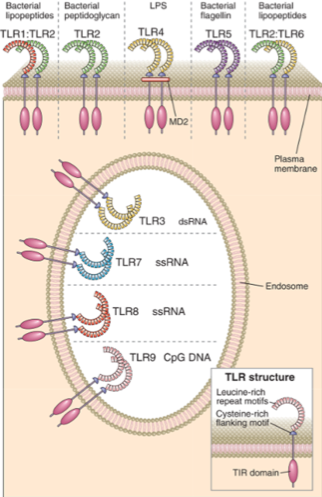
| TLR4 (Toll-like Receptor 4) recognizes: | EXTRACELLULAR things like LPS (can recognize conserved areas of pathogens) |
| Location of pathogen-associated molecular patterns (PAMPs) | NLR (nod-like) and RLR's (rig-like receptors) are intracellular TLR's (toll-like receptors) are extracellular |
| TLR (toll-like receptor) Ligands | -Contain leucine-rich repeats -Toll/IL-1 receptor (TIR) homology domain in their cytoplasmic tails |
| TL4 recognizes | LPS |
| TLR5 recognizes | bacterial flagellin |
| TLR3 recognizes | dsRNA |
| TLR7 & TLR8 recognize | ssRNA |
| TLR9 recognizes | CpG DNA short interspersed DNA sequences that deviate significantly from the average genomic pattern by being GC-rich, CpG-rich, and predominantly non-methylated |
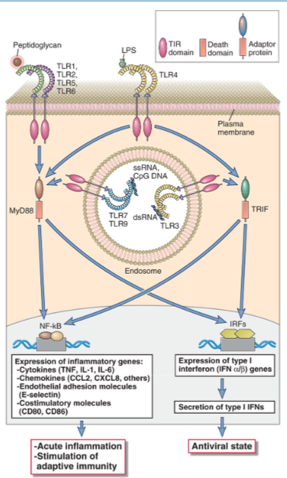
| TLR Signaling Two Core signaling proteins: | MyD88 and TRIF |
| MyD88 and TRIF (core TLR signaling proteins) | Lead to acute inflammation and stimulation of adaptive immune responses -downstream mediators of the TLR's -activate BOTH (not smart enough to to do one or the other in innate immunity) |
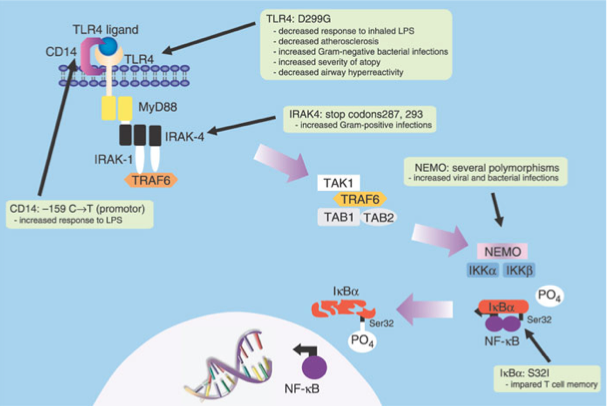
| TLRs in the pathogenesis of Human Disease | CDs: surface markers on cells (allow to distinguish) *Know the 5 Genetic mutations |
| TLR4: D299G Mutation Results in | decreased response to inhaled LPS |
| NEMO Mutation: (several polymorphisms) results in | increased bacterial and viral infections |
| IkBa: S321 Mutation results in | impaired T cell memory |
| IRAK4: stop codons 287, 293 Mutation results in | increased gram-positive infections |
| CARDs (Caspase Recruitment Domain- containing proteins) in human disease: CARD9 deficiency mutation | Reduced DC (dendritic cell) activation of specific T cell subsets -Leads to increased susceptibility of Candida albicans |
| Cytokines | **COMMUNICATION network for cells (recruited to different sites of infection) -Small soluble proteins -Important for development and immune system maturation/function *specific functions!! |
| The cytokines of innate immunity: | IL10 TNF TNF1alpha and TNF1beta |
| Cytokine IL10 | anti-inflammatory (targets macrophages and dendritic cells) |
| Cytokine TNF | pro-inflammatory (many targets-neutrophils, endothelia, etc.) |
| Cytokines TNF1alpha and TNF2beta | VIRAL response (targets every cell because anybody could be infected by a virus) |
| Chemokines and Chemokine Receptors | Low molecular weight proteins Highly conserved secondary structure Two types: CC or CXC REGULATE: 1) Inflammation 2) Leukocyte trafficking (indicates where the lymphocyte should go in the lymph node) 3) Immune cell differentiation |
| Chemokine Subfamily: HIV Co-receptors Main receptor? | CCR5 and CXCR4 (main receptor = CDR4) |
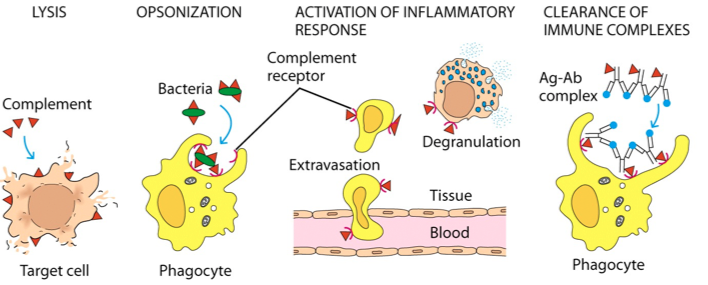
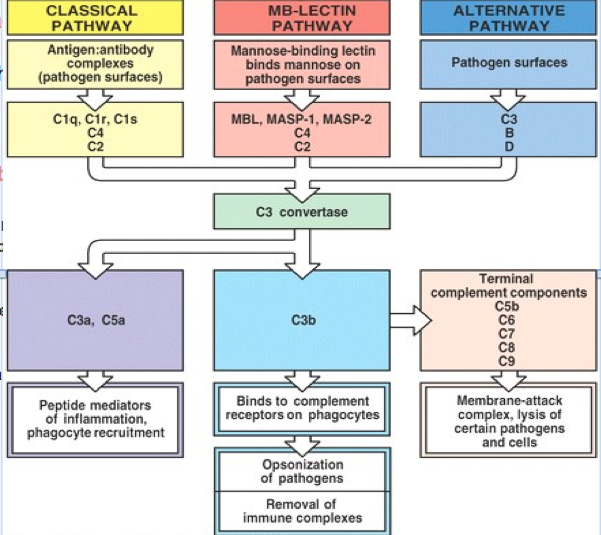
| What is complement? Four principles of complement activation | 1) Lysis of the target cell 2) Opsonization (deposit proteins that enhance uptake of the bacteria) 3) Activation of inflammatory response 4) Clearance of Immune Complexes |
| Complement involves a “proteolytic activation cascade” | |
| What are the 3 pathways of initiation? Classical (antibody required) Alternative (innate) Lectin (innate) | 1) Classical (antibody required) -- initiated by Ab bound to AG (antibody:antigen complexes) 2) Alternative (innate) -- does not involve Ab binding 3) Lectin (innate) -- activated by mannose-binding lectin |
| All three pathways of complement converge at? | C3 Convertase |
| C3 Convertase can split into: | C3a and 5a and C3b |
| C3a and C5a | anaphylatoxins INFLAMMATORY recruit phagocytes |
| C3b | OPSONIZATION (deposit proteins that enhance uptake of the bacteria) AND can split into C5b-C9 |
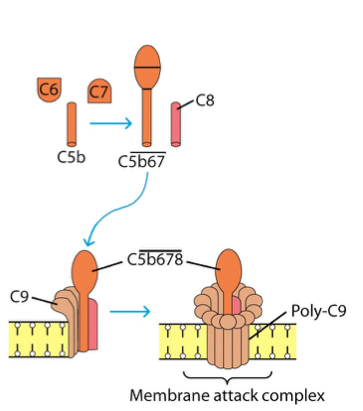
| C5b, C6, C7, C8, and C9 or C5b-C9 | forms the "MAC" (Membrane Attack Complex) complex -lysis of pathogens and cells by forming pores |
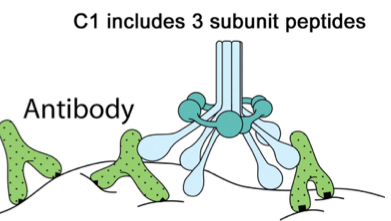
| The Classical Pathway involves 3 Stages Stage 1: | Initiation begins with C1 binding to Ab bound to Ag (antigen:antibody complex) Bind to Fc part of Ab (antigen binds to Fc part of Ab) |
| The Classical Pathway involves 3 Stages Stage 2: | Activated C1 triggers activation of C4 and then C2 -- to form C3 Convertase **Activation of C3 is an important AMPLIFICATION step -C3 convertase C3b (for opsonization) |
| The Classical Pathway involves 3 Stages Stage 3: | C3 Convertase also activates: anaphylatoxins – C3a & C5a C5a is the MOST potent and dominant anaphylatoxin |
| What do C5a and C3a do? | 1) increase vascular permeability -allowing increased fluid leakage and inflammatory runs -also increases migration of PMNs from blood to tissue and vice versa |
| C5b triggers formation of the Membrane Attack Complex | C5b triggers formation -C5b678 = center and C9 surrounds it to form the MAC (membrane attack complex) -pore lyses target cells |
| MAC (Membrane attack complex) is MOST effective against: | Gram-negative bateria Enveloped Viruses |
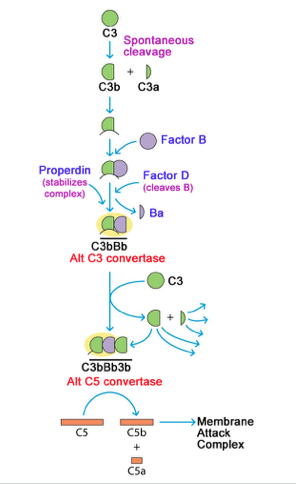
| The Alternative pathway | C3 spontaneously turns over C3a and C3b -Pathogens and Immune complexes --Binding to other protein "factors" creates alternative C3 and C5 Covertases leading to MAC formation *Factor D, Factor B, Properdin |
| Alternative Pathway *Factor D, Factor B, Properdin* | |
| The Lectin Pathway (MB Lectin) | *Mannose Binding Lectin* -binds to bacterial glycoproteins -Creates C1-like activator (activating C4, C2 --> C3 convertase) |
| Complement Regualtion | Negative regulatory step of complement: prevents you from getting affected by complement "attack" |
| Complement Regulation (1) liability of? (2) Sialic acid inactivates? (3) Regulatory proteins? | 1) Lability of protein fragments -rapid, spontaneous inactivation 2) Sialic acid in glycoproteins inactivates C3b on body cells 3) Regulatory proteins e.g., C1 inhibitor Consequence of problems w/regulation of complement: Hereditary Angiodema |
| Complement receptors mediate other functions: -- immune complex clearing -- chemotaxis -- opsonization | |
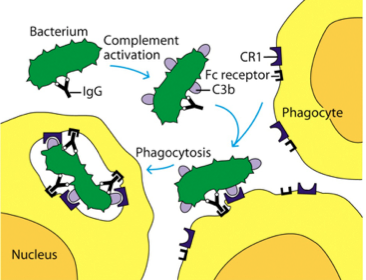
| How does C3b cause opsonization by phagocytic cells? | Roles for both Fc (binds IgG) and Complement receptors C3b is primary opsonin binds to CR1 receptor Coating of viruses blocks receptors and enhances opsonization |
| RBCs and CR1 play major role in immune complex clearance | Immune complexes generate C3b -- via classical or alternative pathways Transport to spleen & liver for Phagocytosis Deficiencies in complement-mediated immune-complex clearing are major cause of Systemic Lupus Erythromatosus (SLE) (C2 deficiency) |
| Complement and Medicine | Targeted biologics Eculizumab (1) Humanize monoclonal binds to complement component C5, inhibiting its cleavage and preventing activation of the lytic pathway --Approved to treat paroxysmal nocturnal hemoglobinuria (PNH) ---Acquired complement deficiency – lack regulatory proteins BLACK BOX WARNING: Increased risk of N. meningitidis infection |
| BUILDUP OF IMMUNITY | |
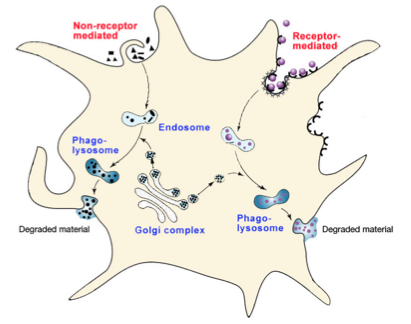
| Macrophage Killing Mechanisms | (1) External: Mediator secretion (2) Internal: requires phagocytosis Receptor mediated, or not Antibody Fc receptors, PRR, etc. (3) O2 dependent: “respiratory burst” O2 Independent: Enzymes (TNF) |
| Neutrophil (PMNs) Mechanisms | (1) Rapid responders FIRST responders! (2) Degranulation & phagocytosis (3) Extracellular Traps: Chromatin & antimicrobial enzymes (non-inflammatory, explodes and forms web to inhibit growth of bacteria) |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quer criar seus próprios Flashcards gratuitos com GoConqr? Saiba mais.