15823591
Descrição
Mapa Mental por Sehar Khan, atualizado more than 1 year ago
|
|
Criado por Sehar Khan
aproximadamente 6 anos atrás
|
|
Esophageal Cancer
- Manifestations
- Onset of signs & symptoms is usually late in relation to
the extent of the tumour (Lewis, 2014; Canadian Cancer Society, 2018)
- Symptoms
- Painful swallowing
(odynophagia), pain the
throat, chest or back
- Fatigue
- Malaise
- Nausea/ Vomiting
- Painful swallowing
(odynophagia), pain the
throat, chest or back
- Signs
- Progressive
Dysphagia
- Weight loss
- Cough
- Reurgitation
- When esophageal stenosis is
severe, regurgitation of
blood-flecked esophageal
contents is common (Lewis, 2014)
- When esophageal stenosis is
severe, regurgitation of
blood-flecked esophageal
contents is common (Lewis, 2014)
- Hiccups
- Hoarseness
- Indigestion
- Heartburn
- Loss of apetite
- Progressive
Dysphagia
- Symptoms
- Onset of signs & symptoms is usually late in relation to
the extent of the tumour (Lewis, 2014; Canadian Cancer Society, 2018)
- Main Causes/Risk
Factors
- Epidemiology (Mao, Zheng & Ling, 2011; Napier, Scheerer & Misra, 2014)
- Sex, Age and Race
- Men are more likely to be diagnosed
with esophageal cancer than women
- Increases with age, with incidence
rates peaking at 70 years of age.
- Incidence and mortality rates in
African-American descent are higher
than that in Caucasians
- Men are more likely to be diagnosed
with esophageal cancer than women
- Geographic Location
- Squamous Cell Carcinoma is most prevalent in parts of China, Iran, South America, France and
Africa and low socioeconomic status is linked with it (Napier, Scheerer & Misra, 2014)
- Adenocarcinoma is most common in developed nations including Australia, Finland, France,
United States and United Kingdom (Napier, Scheerer & Misra, 2014)
- The highest current incidence
of EADC is in Great Britain
- The highest current incidence
of EADC is in Great Britain
- More than 50% of the EC
incidence in the world occur
in China
- Referred to as "Asian esophageal cancer
belt". The region extends from northeast
China to the Middle East (Napier, Scheerer
& Misra, 2014)
- Adenocarcinoma is most common in developed nations including Australia, Finland, France,
United States and United Kingdom (Napier, Scheerer & Misra, 2014)
- Squamous Cell Carcinoma is most prevalent in parts of China, Iran, South America, France and
Africa and low socioeconomic status is linked with it (Napier, Scheerer & Misra, 2014)
- Sex, Age and Race
- Cause of esophageal cancer is unknown but there are important risk factors (Lewis, 2018; Canadian Cancer Society, 2018)
- Long-term irritation of lining of the esophagus
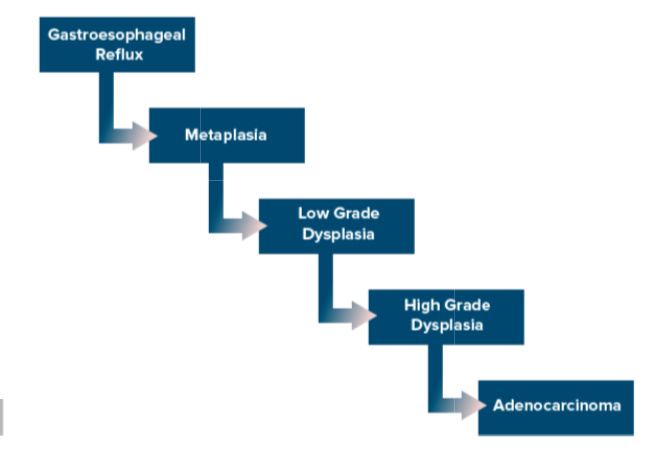
- GERD (Gastroesophageal reflux disease)
- Contents of the stomach back
up, or reflux into the
esophagus and causes
heartburn and discomfort
- GERD increases the risk of
Barret's esophagus, which
increases the risk of
developing ADC.
- GERD increases the risk of
Barret's esophagus, which
increases the risk of
developing ADC.
- Contents of the stomach back
up, or reflux into the
esophagus and causes
heartburn and discomfort
- Barrett's esophagus
- A complication of GERD where stratified
squamous epithelium is replaced by
columnar epithelium (Johns Hopkins
Medicine, n.d; Masab, 2018)
- It is estimated that 1 in 200 cases of Barrett's esophagus
will progress to esophageal cancer (Lewis, 2014)
- It is estimated that 1 in 200 cases of Barrett's esophagus
will progress to esophageal cancer (Lewis, 2014)
- A complication of GERD where stratified
squamous epithelium is replaced by
columnar epithelium (Johns Hopkins
Medicine, n.d; Masab, 2018)
- Achalasia
- The nerves that control the normal
rhythmic contractions in the
esophagus and the lower esophagus
sphincter doesn't work properly.
- The part of the esophagus above sphincter
becomes enlarged, and results in difficulty
swallowing food and liquid.
- The part of the esophagus above sphincter
becomes enlarged, and results in difficulty
swallowing food and liquid.
- The nerves that control the normal
rhythmic contractions in the
esophagus and the lower esophagus
sphincter doesn't work properly.
- Tylosis
- Rare inherited disease with scaly patches
(hyperkeratosis) on hand and feet and also
growths with finger-like projections, called
paillomas in the esophagus (Canadian
Cancer Society, 2018)
- Researchers have identified the
tylosis esophageal cancer (TOC)
gene.
- Researchers have identified the
tylosis esophageal cancer (TOC)
gene.
- Rare inherited disease with scaly patches
(hyperkeratosis) on hand and feet and also
growths with finger-like projections, called
paillomas in the esophagus (Canadian
Cancer Society, 2018)
- Plummer-vinson syndrome
- The mucous membranes of the mouth, throat and
esophagus waste away and a thin member of
tissue (known as esophageal web) can also grow
anywhere along the esophagus, which causes
problems swallowing (Canadian Cancer Society,
2018)
- A patient with a history of achalasia
is at greater risk for squamous cell
cancer (Lewis, 2014)
- A patient with a history of achalasia
is at greater risk for squamous cell
cancer (Lewis, 2014)
- The mucous membranes of the mouth, throat and
esophagus waste away and a thin member of
tissue (known as esophageal web) can also grow
anywhere along the esophagus, which causes
problems swallowing (Canadian Cancer Society,
2018)
- Scarring from swallowing lye
- Lye that is found in strong cleaners like drain
cleaners can burn and destroy esophageal
cells (Lewis, 2014)
- Lye that is found in strong cleaners like drain
cleaners can burn and destroy esophageal
cells (Lewis, 2014)
- HPV infection
- Studies have shown increased incidence of HPV infection in ESCC from Asian countries, South Africa,
Alaska, and Australia (Mao, Zheng & Ling, 2011)
- Studies have shown increased incidence of HPV infection in ESCC from Asian countries, South Africa,
Alaska, and Australia (Mao, Zheng & Ling, 2011)
- GERD (Gastroesophageal reflux disease)
- Lifestyle risk factors
- Smoking
- Smoking and drinking are the primary risk factors and have
synergistic effects. Alcohol is the major factor, but smoking may
increase the carcinogenicity caused by alcohol (Napier, Scheerer
& Misra, 2014; Zhang, 2013)
- Smoking and drinking are the primary risk factors and have
synergistic effects. Alcohol is the major factor, but smoking may
increase the carcinogenicity caused by alcohol (Napier, Scheerer
& Misra, 2014; Zhang, 2013)
- Excessive alcohol intake
- Nutritional imbalance
- Over-nutrition
- Excessive carbohydrate intake
and obesity (developed nations)
- Excessive carbohydrate intake
and obesity (developed nations)
- Under-nutrition
- Low intake of micronutrients such as vitamin A,
C, E, riboflavin, zinc, selenium and low intake of
fresh fruits and vegetables (developing nations)
- Low intake of micronutrients such as vitamin A,
C, E, riboflavin, zinc, selenium and low intake of
fresh fruits and vegetables (developing nations)
- Over-nutrition
- Drinking very hot beverages
- Drinking green tea at high temperatures
resulted in a six or seven times greater
increase in the risk of ESCC in patients who
were also smokers (Torres-Aguilera &
Remes, 2018)
- Drinking green tea at high temperatures
resulted in a six or seven times greater
increase in the risk of ESCC in patients who
were also smokers (Torres-Aguilera &
Remes, 2018)
- Chewing of betel quid (paan)
- Common in India and China. Contains cancer-causing
substances that increase the risk of developing SCC of
the esophagus (Canadian Cancer Society, 2018)
- Common in India and China. Contains cancer-causing
substances that increase the risk of developing SCC of
the esophagus (Canadian Cancer Society, 2018)
- Obesity
- Three times more risk of EADC
in overweight people (Zhang, 2013)
- Also a risk factor for GERD
- Also a risk factor for GERD
- Three times more risk of EADC
in overweight people (Zhang, 2013)
- Smoking
- Long-term irritation of lining of the esophagus
- Epidemiology (Mao, Zheng & Ling, 2011; Napier, Scheerer & Misra, 2014)
- Classifications
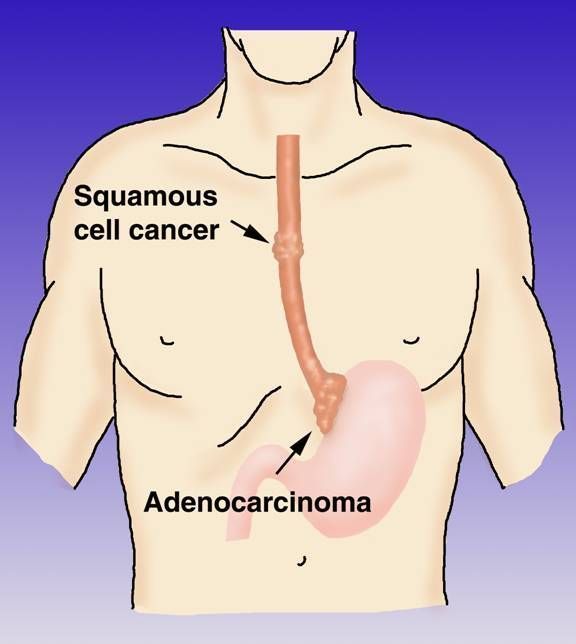
- Adenocarcinoma
(Canadian Cancer
Society, 2018)
- develops in the lower
third of the esophagus,
often in an area
containing Barrett’s
esophagus
- Barett's Esophagus: a complication of
GERD where stratified squamous
epithelium is replaced by columnar
epithelium (Johns Hopkins Medicine,
n.d; Masab, 2018)
- Occurs due to chronic reflux
of gastric acid and bile at
gastroesophageal junction
- Progresses to adenocarcinoma
- Progresses to adenocarcinoma
- Occurs due to chronic reflux
of gastric acid and bile at
gastroesophageal junction
- Barett's Esophagus: a complication of
GERD where stratified squamous
epithelium is replaced by columnar
epithelium (Johns Hopkins Medicine,
n.d; Masab, 2018)
- Advanced adenocarcinoma
of the esophagus often grows
into the GE junction and can
even grow into the upper
part of the stomach
- Pathophysiology (Masab,
2018)
- Changes in gene structure,
expression and protein structure
leading to tumor growth
- Risk factor of obesity lead to
hypertrophied adipocytes and
inflammatory cells within fat deposits,
creating an environment of low-grade
inflammation and promote tumor
development through the release of
adipokines and cytokines
- Adipocytes supply energy
production and support tumor
growth and progression
- Adipocytes supply energy
production and support tumor
growth and progression
- Changes in gene structure,
expression and protein structure
leading to tumor growth
- develops in the lower
third of the esophagus,
often in an area
containing Barrett’s
esophagus
- Squamous Cell
Carcinoma
- It can occur anywhere along the
esophagus, but it is most common in
the middle and upper part; occurs as
one or more tumors (Canadian Cancer
Society, 2018)
- Pathophysiology (Masab,
2018)
- Risk factors such as alcohol
and carcinogens found in
tobacco cause damage to
cellular DNA
- Decrease metabolic activity within
the cell to inhibit detoxification
and increase oxidation
- Inflammation of squamous
epithelium leads to dysplasia
and in situ malignant
transformation
- Dysplasia: appears as an
accumulation of atypical cells
(Mao, Zheng & Ling, 2011)
- Tumors usually present as fungating,
ulcerating, or infiltrating lesions in
the esophageal epithelium (Moa,
Zheng & Ling, 2011)
- Dysplasia: appears as an
accumulation of atypical cells
(Mao, Zheng & Ling, 2011)
- Decrease metabolic activity within
the cell to inhibit detoxification
and increase oxidation
- Risk factors such as alcohol
and carcinogens found in
tobacco cause damage to
cellular DNA
- Most common type of
esophageal cancer worldwide
(Napier, Scheerer & Misra, 2014)
- It can occur anywhere along the
esophagus, but it is most common in
the middle and upper part; occurs as
one or more tumors (Canadian Cancer
Society, 2018)
- Adenocarcinoma
(Canadian Cancer
Society, 2018)
- Treatment &
Management
- Surgical Interventions
(Lewis, 2014)
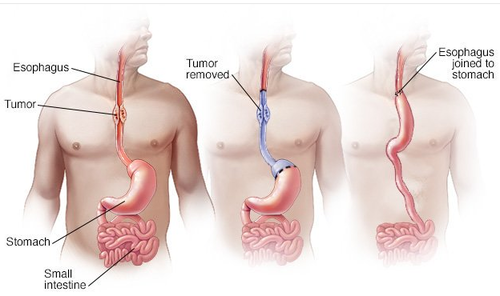
- Esophagectomy
- Removal of part or all
of the esophagus
- Removal of part or all
of the esophagus
- Esophagogastrostomy
- resection of a part of the
esophagus and anastomosis
of the remaining portion to
the stomach
- resection of a part of the
esophagus and anastomosis
of the remaining portion to
the stomach
- esophagogastrostomy
- resection of a portion of the
esophagus and anastomosis of a
segment of colon to the
remaining portion
- resection of a portion of the
esophagus and anastomosis of a
segment of colon to the
remaining portion
- May be thoracic or both
abdominal and thoracic
- Minimally invasive
esophagectomy
(laparoscopic vagal
nerve–sparing) uses smaller
incisions decreasing
hospital stays, and fewer
pulmonary complications
- Esophagectomy
- Radiation Therapy
(Canadian Cancer
Society, 2018)
- uses high-energy
rays or particles to
destroy cancer cells
- Commonly used to:
- shrink a tumour
before other
treatments such as
surgery
- destroy cancer
cells in the body
(as a primary
treatment)
- destroy
adenocarcinoma
cells left behind
after surgery and
reduce the risk of
the cancer
recurring
- shrink a tumour
before other
treatments such as
surgery
- may be used alone to
relieve pain or control
the symptoms of
advanced esophageal
cancer (palliative
radiation therapy)
- Two Types
- External Beam
- a machine directs
radiation through the skin
to the tumour and some
of the tissue around it
- Done 5x/week for
several weeks
- Done 5x/week for
several weeks
- a machine directs
radiation through the skin
to the tumour and some
of the tissue around it
- Brachytherapy
- an internal radiation therapy
that uses a radioactive material
called a radioactive isotope. It is
placed right into, or very close
to, the tumour and the radiation
kills the cancer cells over time.
- an internal radiation therapy
that uses a radioactive material
called a radioactive isotope. It is
placed right into, or very close
to, the tumour and the radiation
kills the cancer cells over time.
- External Beam
- uses high-energy
rays or particles to
destroy cancer cells
- Chemotherapy (Canadian
Cancer Society, 2018)
- may be given before surgery
(neoadjuvant chemotherapy) and after
surgery (called adjuvant chemotherapy),
or as the main treatment given (primary
chemotherapy)
- Neoadjuvent
chemotherapy: given
to shrink an
adenocarcinoma
before surgery
- Adjuvent chemotherapy:
to destroy cancer cells
left behind and lower the
risk that cancer will
come back, or recur
- Primary chemotherapy:
chemotherapy given as the main
treatment; it may be used for stage
4 esophageal cancer or if person is
not healthy enough to have
surgery or chemoradiation
- Sometimes used to relieve pain
or control the symptoms of
advanced esophageal cancer;
palliative chemotherapy
- Sometimes used to relieve pain
or control the symptoms of
advanced esophageal cancer;
palliative chemotherapy
- Neoadjuvent
chemotherapy: given
to shrink an
adenocarcinoma
before surgery
- may be given before surgery
(neoadjuvant chemotherapy) and after
surgery (called adjuvant chemotherapy),
or as the main treatment given (primary
chemotherapy)
- Chemoradiation
- Chemotherapy and
radiation therapy are
used at the same
time for treatment
- Chemotherapy and
radiation therapy are
used at the same
time for treatment
- Molecular Targeted Therapy (Canadian
Cancer Society, 2018)
- Uses drugs to target molecules
that tell the cells to to grow or
divide, thus stopping the growth
and spread of cancer cells while
limiting harm to normal cells
- Most commonly administered
targeted drug is trastuzumab
(Herceptin)
- Most commonly administered
targeted drug is trastuzumab
(Herceptin)
- Uses drugs to target molecules
that tell the cells to to grow or
divide, thus stopping the growth
and spread of cancer cells while
limiting harm to normal cells
- Endoscopic Mucosal Resection
Canadian Cancer Society, 2018)
- used to remove small, early stage tumours
that are only in the inner layer, or mucosa,
of the esophagus and have not spread to
the other layers of the esophagus
- After EMR, the healthy tissue removed along with the
tumour is examined under a microscope. If cancer
cells found in the tissue, more EMR or treatment with
chemotherapy, radiation therapy or photodynamic
therapy (PDT) may be needed to completely remove
or destroy the cancer.
- PDT: treatment with drugs that
make cells sensitive to light
(called photosensitizers). Drug
is taken up by cancer cells,
then, endoscope is used to
expose cancer cells to light
- PDT: treatment with drugs that
make cells sensitive to light
(called photosensitizers). Drug
is taken up by cancer cells,
then, endoscope is used to
expose cancer cells to light
- After EMR, the healthy tissue removed along with the
tumour is examined under a microscope. If cancer
cells found in the tissue, more EMR or treatment with
chemotherapy, radiation therapy or photodynamic
therapy (PDT) may be needed to completely remove
or destroy the cancer.
- used to remove small, early stage tumours
that are only in the inner layer, or mucosa,
of the esophagus and have not spread to
the other layers of the esophagus
- Palliative Therapy (Lewis,
2014)
- consists of
restoration of
swallowing and
maintenance of
nutrition and
hydration
- Relieve obstruction
- Dilation: relieves
dysphagia, allows for
improved nutrition
- Stent Placement: may help when
dilation is no longer effective.
Stent is placed in esophagus so
that food and fluids can pass
through stenotic segment of
esophagus
- Tube placement
for nutritional
support and pain
management
- consists of
restoration of
swallowing and
maintenance of
nutrition and
hydration
- Surgical Interventions
(Lewis, 2014)
- Diagnostic Testing (Lewis, 2014; Canadian
Cancer Society, 2018)
- Upper GI endoscopy
- A flexible tube with a light
and lens on the end
passes through the mouth
and down the throat into
the esophagus.
- To check for bleeding,
ulcers, tumours,
inflammation or narrowing.
- Also done to take samples
of tissue to be tested in the
lab (biopsy).
- Endoscopy with biopsy is necessary to
make a definitive diagnosis of carcinoma
by identification of malignant cells (Lewis,
2014)
- Endoscopy with biopsy is necessary to
make a definitive diagnosis of carcinoma
by identification of malignant cells (Lewis,
2014)
- Also done to take samples
of tissue to be tested in the
lab (biopsy).
- To check for bleeding,
ulcers, tumours,
inflammation or narrowing.
- A flexible tube with a light
and lens on the end
passes through the mouth
and down the throat into
the esophagus.
- Endoscopic ultrasonography
- High-frequency
sound waves to
make images of
structures in body.
- Uses an endoscope with an ultrasound
probe. It provides detailed information
about the location, size, depth of the
tumour and if the cancer has spread to
surrounding lymph nodes or tissues
(Canadian Cancer Society, 2018).
- Important tool used to stage
esophageal cancer (Lewis, 2014)
- Important tool used to stage
esophageal cancer (Lewis, 2014)
- Uses an endoscope with an ultrasound
probe. It provides detailed information
about the location, size, depth of the
tumour and if the cancer has spread to
surrounding lymph nodes or tissues
(Canadian Cancer Society, 2018).
- High-frequency
sound waves to
make images of
structures in body.
- Biopsy
- Removal of tissue/ cell from
the body to confirm
malignancy
- Removal of tissue/ cell from
the body to confirm
malignancy
- Other tests (Canadian Cancer Society, 2018; Lewis, 2014)
- CT scan
- CT and MRI makes
3-D pictures of the
organs, tissues,
bones and blood
vessels. They are
used to assess the
extent of the disease
(Lewis, 2018)
- CT and MRI makes
3-D pictures of the
organs, tissues,
bones and blood
vessels. They are
used to assess the
extent of the disease
(Lewis, 2018)
- PET scan
- Radioactive 3-d colour images to look
for changes in the metabolic activity of
body tissues
- Radioactive 3-d colour images to look
for changes in the metabolic activity of
body tissues
- MRI
- Pulmonary function tests
- Group of tests that
measure how well the
lungs are functioning
- Group of tests that
measure how well the
lungs are functioning
- Heart function tests
- ECG measures the
electrical activity in the
heart. Echocardiogram
uses ultrasound to
look at the structure
and motion of the
heart
- ECG measures the
electrical activity in the
heart. Echocardiogram
uses ultrasound to
look at the structure
and motion of the
heart
- Thorascopy
- Procedure involving
tube-like instrument with
light to assess for cancer
in lymph nodes and other
organs near the
esophagus (Canadian
Cancer Society, 2018)
- Procedure involving
tube-like instrument with
light to assess for cancer
in lymph nodes and other
organs near the
esophagus (Canadian
Cancer Society, 2018)
- Laparoscopy
- Procedures that uses endoscope to
examine and remove internal organs
and to accurately stage esophageal
cancer
- Procedures that uses endoscope to
examine and remove internal organs
and to accurately stage esophageal
cancer
- Bronchoscopy
- Performed to detect
malignant involvement of
the lung (Lewis, 2018)
- Performed to detect
malignant involvement of
the lung (Lewis, 2018)
- CT scan
- History and physical examination
- Barium swallow
- Barium is a liquid that
coats the inside of
organs and shows
their outline clearly
on an x-ray.
- Often the first
diagnostic test used to
check for esophageal
cancer.
- It can show ulceration, narrowing/ stricture of the
esophagus, the location and general size of the
tumour, abnormal opening from the esophagus
into the trachea (tracheoesophageal fistula) and
spread of cancer to the stomach (Canadian Cancer
Society, 2018; Lewis, 2018).
- It can show ulceration, narrowing/ stricture of the
esophagus, the location and general size of the
tumour, abnormal opening from the esophagus
into the trachea (tracheoesophageal fistula) and
spread of cancer to the stomach (Canadian Cancer
Society, 2018; Lewis, 2018).
- Often the first
diagnostic test used to
check for esophageal
cancer.
- Barium is a liquid that
coats the inside of
organs and shows
their outline clearly
on an x-ray.
- Staging (Canadian Cancer
Society, 2018; Napier,
Scheerer & Misra, 2014)
- Squamous Cell Carcinoma
- Stage 0
- Tumour only within the
epithelium of the inner lining
of the esophagus.
Precancerous condition.
- Tumour only within the
epithelium of the inner lining
of the esophagus.
Precancerous condition.
- Stage 1A
- Tumour grown into the
connective tissue or
muscle layer of the
mucosa
- Tumour grown into the
connective tissue or
muscle layer of the
mucosa
- Stage 1B
- Tumour grown into the
connective tissue or muscle
layer of: the mucosa/
surrounding the mucusa, thick
outer muscle layer
- Tumour grown into the
connective tissue or muscle
layer of: the mucosa/
surrounding the mucusa, thick
outer muscle layer
- Stage 2A
- Tumour grown into the muscularis propria or
connective tissue that supports and covers the
outside of the esophagus or grown into the
adventitia.
- Tumour grown into the muscularis propria or
connective tissue that supports and covers the
outside of the esophagus or grown into the
adventitia.
- Stage 2B
- Tumour grown into the adventitia.into the
adventitia or connective tissue or muscle
layer of the mucosa or into the submucosa.
The cancer has also spread to 1 or 2 nearby
lymph nodes.
- Tumour grown into the adventitia.into the
adventitia or connective tissue or muscle
layer of the mucosa or into the submucosa.
The cancer has also spread to 1 or 2 nearby
lymph nodes.
- Stage 3A
- Tumour grown into the connective
tissue or muscle layer of the mucosa or
into the submucosa or the muscularis
propria. Spread to 3-6 nearby lymph
nodes
- Tumour grown into the connective
tissue or muscle layer of the mucosa or
into the submucosa or the muscularis
propria. Spread to 3-6 nearby lymph
nodes
- Stage 3B
- Tumour grown into the
muscularis propria or
adventitia, or nearby areas
such as pleura, pericardium,
diaphragm, peritoneum or
azygos vein.
- Tumour grown into the
muscularis propria or
adventitia, or nearby areas
such as pleura, pericardium,
diaphragm, peritoneum or
azygos vein.
- Stage 4A
- Tumour grown into nearby areas
such as the pleura, pericardium,
diaphragm, peritoneum, or
azygos vein or main artery
carring blood of the heart,
vertebrae or trachea.
- Tumour grown into nearby areas
such as the pleura, pericardium,
diaphragm, peritoneum, or
azygos vein or main artery
carring blood of the heart,
vertebrae or trachea.
- Stage 4B
- The cancer has spread to
other parts of the body
(distant metastasis), such
as to the lungs, liver, &
stomach.
- The cancer has spread to
other parts of the body
(distant metastasis), such
as to the lungs, liver, &
stomach.
- Stage 0
- Adenocarcinoma
- Stage 1A
- Tumour grown into the
connective tissue or muscle
layer of the mucosa
- Tumour grown into the
connective tissue or muscle
layer of the mucosa
- Stage 1B
- Tumour grown into
connective tissue or muscle
layer of the mucosa or into
the submucosa or the thick
outer muscle layer
(muscularis propria)
- Tumour grown into
connective tissue or muscle
layer of the mucosa or into
the submucosa or the thick
outer muscle layer
(muscularis propria)
- Stage 1C
- Tumour has grown into the connective tissue or muscle
layer of the mucosa or into the submucosa or the thick outer
muscle layer (muscularis propria).
- Tumour has grown into the connective tissue or muscle
layer of the mucosa or into the submucosa or the thick outer
muscle layer (muscularis propria).
- Stage2A
- Tumour grown into the muscularis propria
- Tumour grown into the muscularis propria
- Stage 2B
- Tumour has grown into the connective tissue or muscle
layer of the mucosa or into the submucosa or it has
grown into the layer of connective tissue that supports
and covers the outside of the esophagus (adventitia).
- Tumour has grown into the connective tissue or muscle
layer of the mucosa or into the submucosa or it has
grown into the layer of connective tissue that supports
and covers the outside of the esophagus (adventitia).
- Stage 3A
- Tumour grown into the
connective tissue or muscle
layer of the mucosa or into
the submucosa or it grows
into muscolaris propria.
- Tumour grown into the
connective tissue or muscle
layer of the mucosa or into
the submucosa or it grows
into muscolaris propria.
- Stage 3B
- Tumour grown into the muscularis propria or
the adventitia or into nearby areas such as the
pleura, pericardium, diaphragm, peritoneum or
vein that runs along the spinal column (azygos
vein).
- Tumour grown into the muscularis propria or
the adventitia or into nearby areas such as the
pleura, pericardium, diaphragm, peritoneum or
vein that runs along the spinal column (azygos
vein).
- Stage 4A
- Tumour grown into nearby
areas such as the pleura,
pericardium, diaphragm,
peritoneum, or azygos vein
or main artery carring
blood of the heart,
vertebrae or trachea.
- Tumour grown into nearby
areas such as the pleura,
pericardium, diaphragm,
peritoneum, or azygos vein
or main artery carring
blood of the heart,
vertebrae or trachea.
- Stage 4B
- Cancer has spread to other parts of
the body (distant metastasis) such
as lungs, liver or stomach
- Cancer has spread to other parts of
the body (distant metastasis) such
as lungs, liver or stomach
- Stage 0
- Tumour only within the
epithelium of the
inner lining of the
esophagus.
Precancerous
condition.
- Tumour only within the
epithelium of the
inner lining of the
esophagus.
Precancerous
condition.
- Stage 1A
- Staging is essential to deciding
appropriate treatment and
interventions
- Squamous Cell Carcinoma
- Complete blood count
- Several laboratory
tests to assess RBC,
WBC, and platelets.
- To check for anemia and
bleeding; set a baseline
to compare with blood
tests done during and
after treatment to check
the effects of therapies
- To check for anemia and
bleeding; set a baseline
to compare with blood
tests done during and
after treatment to check
the effects of therapies
- Several laboratory
tests to assess RBC,
WBC, and platelets.
- Upper GI endoscopy
- Nursing
Interventions/Care (Lewis,
2014)
- Preoperative
- Assess for poor nutrition due to inability
to ingest adequate amounts of food/
fluids
- High calorie, high
protein diet
- High calorie, high
protein diet
- Teach client/family how to
keep intake/output records
and assess for signs of fluid &
electrolyte imbalance
- Meticulous oral
care
- Assess for poor nutrition due to inability
to ingest adequate amounts of food/
fluids
- Postoperatively
- Assess NG tube
drainage
- May be bloody for first
8-12 hours, gradually
becoming greeish-yelloe
- May be bloody for first
8-12 hours, gradually
becoming greeish-yelloe
- Monitor for
respiratory
complications
- Turning and deep breathing
done every 2 hours; use
Incentive spirometer
- Turning and deep breathing
done every 2 hours; use
Incentive spirometer
- Must place client in
semi-Fowler or Fowler position
to prevent reflux and
aspirations of gastric secretions
- Maintain upright position
for at least 2 hours after
eating
- Maintain upright position
for at least 2 hours after
eating
- Assess NG tube
drainage
- continuous follow-up, encouragement
and assisstence in maintaining
nutrition
- May require a
permanent
gastrostomy
- May require a
permanent
gastrostomy
- Help decrease client's
fear/anxieties through
therapeutic communication
- Other patient outcomes
- Relief of pain
- maintain patent
airway
- able to swallow
comfortably
- understand
prognosis of
disease
- Relief of pain
- Preoperative
- Complications (Lewis,
2014)
- Hemorrhage may occur if the cancer erodes through
the esophagus and into the aorta.
- Esophageal perforation with fistula formation into
the lung or the trachea can sometimes develop
- Could spread via lymph system. Liver and the lung
are common sites of metastasis.
- The tumour may enlarge enough to
cause esophageal obstruction.
- Hemorrhage may occur if the cancer erodes through
the esophagus and into the aorta.
Anexos de mídia
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quer criar seus próprios Mapas Mentais gratuitos com a GoConqr? Saiba mais.