Descrição
|
|
Criado por Omolade Abidoye
aproximadamente 6 anos atrás
|
|
Página 1
UPPER LIMB FRACTURES CBL
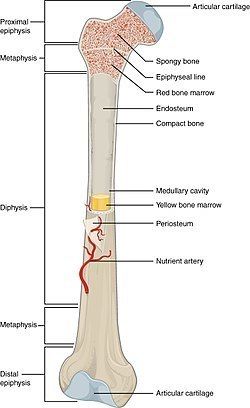
Osteoporotic fractures: occur with minimal trauma Pathological fractures: no trauma Stress fractures: due to prolonged unaccustomed activity but no trauma ANATOMY: outer envelope is cortical bone while inner core is cancellous bone
{kind=link}
:::::::::::::::::::::::::::: humerus ::::::::::::::::::::::::
ANATOMY muscle insertion for pec major, deltoid and corachobrachialis muscle origin for brachialis, biceps and brachioradialis median + ulnar nerve run along shaft while radial nerve is in spiral groove in between proximal and medial epicondyle
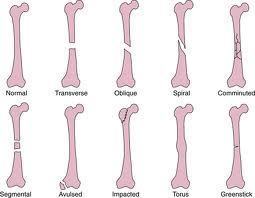
MODE OF INJURY direct trauma usually a transverse fracture indirect trauma usually spiral fracture fall on outstretched hand: high velocity comminuted fractures minimal trauma: pathological fractures in elderly fractures mostly in middle third (60%)
{kind=link}
Investigations: XR, MR/bone scan (pathological fractures), calcium levels Initial mgt: pain relief, splint, x-ray exam, temporary splintage definitve mgt: sugar tong humeral brace and regular XRs conservative mgt: fn-al brace for shaft fractures indications for surgery: open fracture, neurovascular injury, segmental fractures, polytrauma, floating elbow, floating shoulder, adequate alignment
INTRAMEDULLARY NAILING anterograde/retrograde** indicated in patho, segmental and osteoporotic fractures COMPRESSION PLATING method of choice for fixing fractures better union rate and lower complication rate compared with nailing COMPLICATIONS OF SURGERY (definite): infection, delayed/non union, nerve damage (radial nerve palsy) most humeral fractures treated conservatively radial nerve involvement should be checked 90% heal well
{kind=link}
{kind=link}
Página 2
hand and wrist fractures
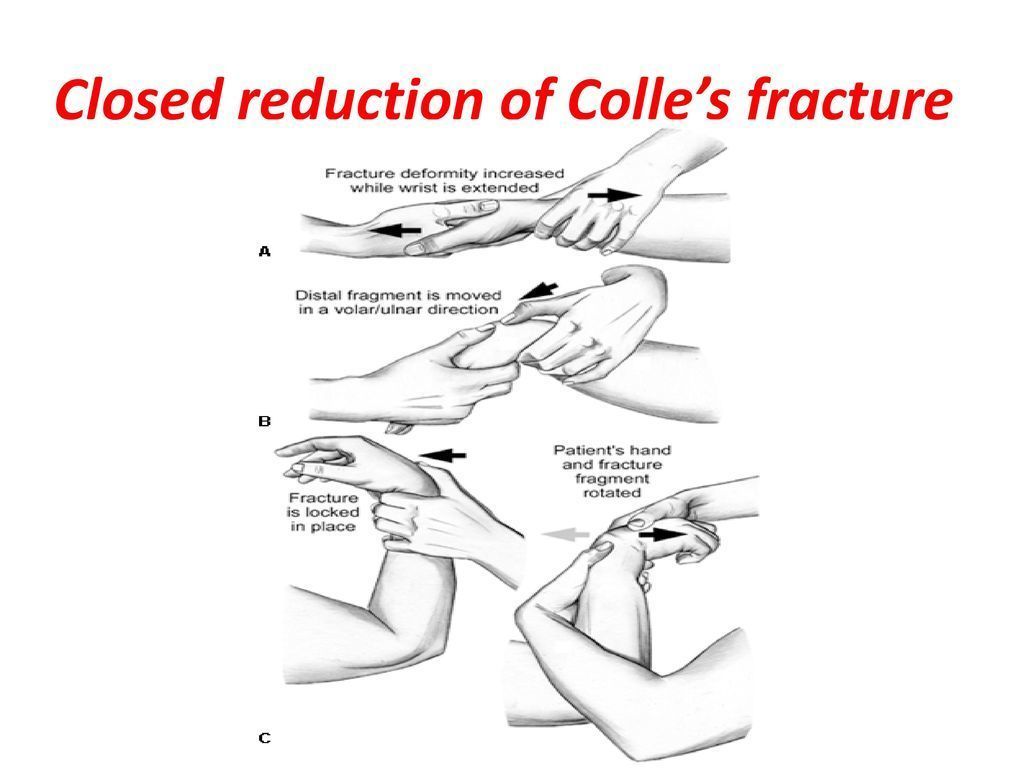
COLLES FRACTURE #1 distal radius fracture FOOSH #1 in older women due to osteoprosis on XR consider: angulation, impaction, displacement, joint involvement, other fractures (ulnar styloid, carpal bones) MGT conservative: with closed reduction (immediate in neurovascular damage) and plaster cast immobilisation, surgical: open plating, external fixation, closed manipulation COMPLICATIONS: malunion w/ dinner fork deformity, median nerve palsy, carpal tunnel
{kind=link}
SCAPHOID FRACTURES #1 carpal fracture 15-30y males caused by FOOSH or forced dorsiflexion (steering wheel) CFs: tenderness in anatomical snuffbox, scaphoid tubercle and longitudinal compression of scaphoid Investigations: scaphoid series (3/4 plain X-Rays), 2nd line is MRI Dx is difficult with XR MGT: Immobilise in plaster cast Follow-up internal fixation (screw/wire) to reduce risk of complication bone grafting potentially for non union Comps: non/mal union, OA, scapho-lunate dissociation, avascular necrosis
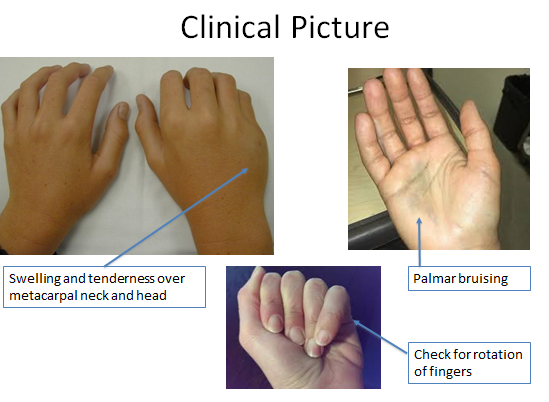
BOXER'S FRACTURE - #1 metacarpal fracture: 5th metacarpal neck with volar (palmar) displacement - usually after a punch - MGT: check for other injuries, abx for open wounds, most will heal with minimal immobilisation/splintage, may require operative fixation with percutaneous wires.
{kind=link}
Quer criar suas próprias Notas gratuitas com a GoConqr? Saiba mais.