Página 1
Classifications of Pain
Nociceptivedestroyed tissue activates nociceptive nerve fibers physical, chemical, pressure, thermal destruction1. Somatic injury to skin, muscle, soft tissue, bone very incidental or movement related localized constant or intermittent gnawing, aching, sharp with movement 2. Visceral less localized constant referred aching, squeezing, cramping
Neuropathic injury to nerve tissue central, peripheral, autonomic radiates along nerves or nerve roots Feels like: burning dysesthesia (numb, tingling), hyperalgesia (exagerrated response to painful stimulus) lancinating/ piercing/stabbing allodynia (pain from stimulus that doesn't usu cause pain)
Mixeddue to combo of :- physical destruction of tissue- inflammation caused by/ in response to tumors that activate nerves
pain is subjective experience multiple domains
PHYSICALUse : Brief Pain InventoryAssess: location pattern of occurence quality aggravating or relieving factors raditation of pain severity and variation in severity affects on ADLs pain tx and analgesic hx - adverse effects, compliance breakthrough pain - incident & spontaneous Present & past medical hx. Look for: delirium, cognitive failure, dementia (affects expression of pain) chronic pain (ie OA or diabetic neuropathy) exposure to neurotoxic antineoplastic agents complicated cancer pain syndromes (malignant leptomeningeal spread, plexus involvement, pathological fractures) infection or abscess hepatic or renal impairment medication interactions
LOOK UP: malignant leptomeningeal spread plexus involvement pathological fractures concomitant infection abscess assessment in cognitively impaired
PSYCHOLOGICAL depression, anxiety limited understanding of illness fear of opiods anger towards HCP or health care system personality or psychiatric disorder loss of body image poor coping denial hx drug or alcohol abuse
SOCIALfinancial issuesculture, religionfamily issues: discord or dysfunction guilt lack of understanding illness denial or unrealistic expectations
COMPLICATION CANCER PAINAssessment & management can be complicated in: younger pts neuropathic pain incidental/ episodic pain presence of psych distress substance abuse disorder severe pain at start
PAIN IN THE COGNITIVELY IMPAIRED look at behaviours available assessment tools not validated or reliable
Education pt & Family origin of pain type of pain initial management - titration expected adverse effects - management of pain monitoring address fear of opiods
Prevent & Minimize Adverse Effectsuse combination of educations & drugs
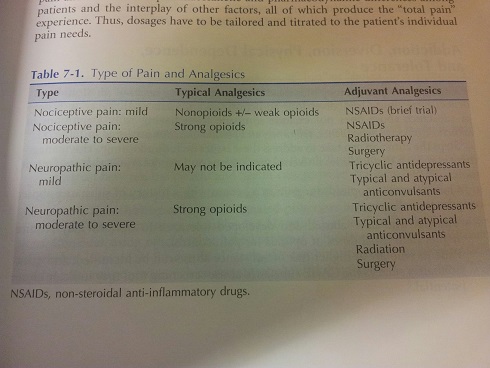
Matching Pain Severity to AnalgesicUSE: WHO 3-Step ladder
{kind=link}
LOOK UPtotal pain
LOOK UPtotal pain
Prescribe around-the-clock dose & breakthrough/rescue doses
Consider Adjuvants
Classifications of Pain
Pain Assessment
Management - Principles
Quer criar suas próprias Notas gratuitas com a GoConqr? Saiba mais.