12973931
Description
Quiz by Melanie Grynsztejn, updated more than 1 year ago
|
|
Created by Melanie Grynsztejn
almost 7 years ago
|
|
Question 1
Question
The following are early onset EPS symptoms
Answer
-
Dystonia
-
Akathisia
-
Parkinsonism
-
Tardive dyskensia
Question 2
Question
Which EPS symtom can appear within days
Answer
-
Dystonia
-
Akatsia
-
Parkinsonism
-
Tardive dyskinesia
Question 3
Question
Which EPS symptom can appear within weeks?
Answer
-
Dystonia
-
Akathisia
-
Parkinsonsism
-
Tardive dyskenia
Question 4
Question
Which EPS symptom can appear within months?
Answer
-
Dystonia
-
Akathisia
-
Parkinsonism
-
Tardive dyskinesia
Question 5
Question
Which EPS symtoms can take years to appear?
Answer
-
Dystonia
-
Akathisia
-
Parkinsonism
-
Tardive dyskensia
Question 6
Question
Types of drug-induced movement disorders:
[blank_start]Acute:[blank_end] Occur within a short duration of treatment onset or dose increase
[blank_start]Chronic:[blank_end] Symptoms persist throughout treatment
[blank_start]Tardive[blank_end]: Delayed onset of symptoms
[blank_start]Withdrawal:[blank_end] Occur in the absence of treatment. May resolve
Answer
-
Acute:
-
Withdrawal:
-
Chronic:
-
Tardive
-
Tardive
-
Withdrawal
-
Withdrawal:
-
Tardive
Question 7
Question
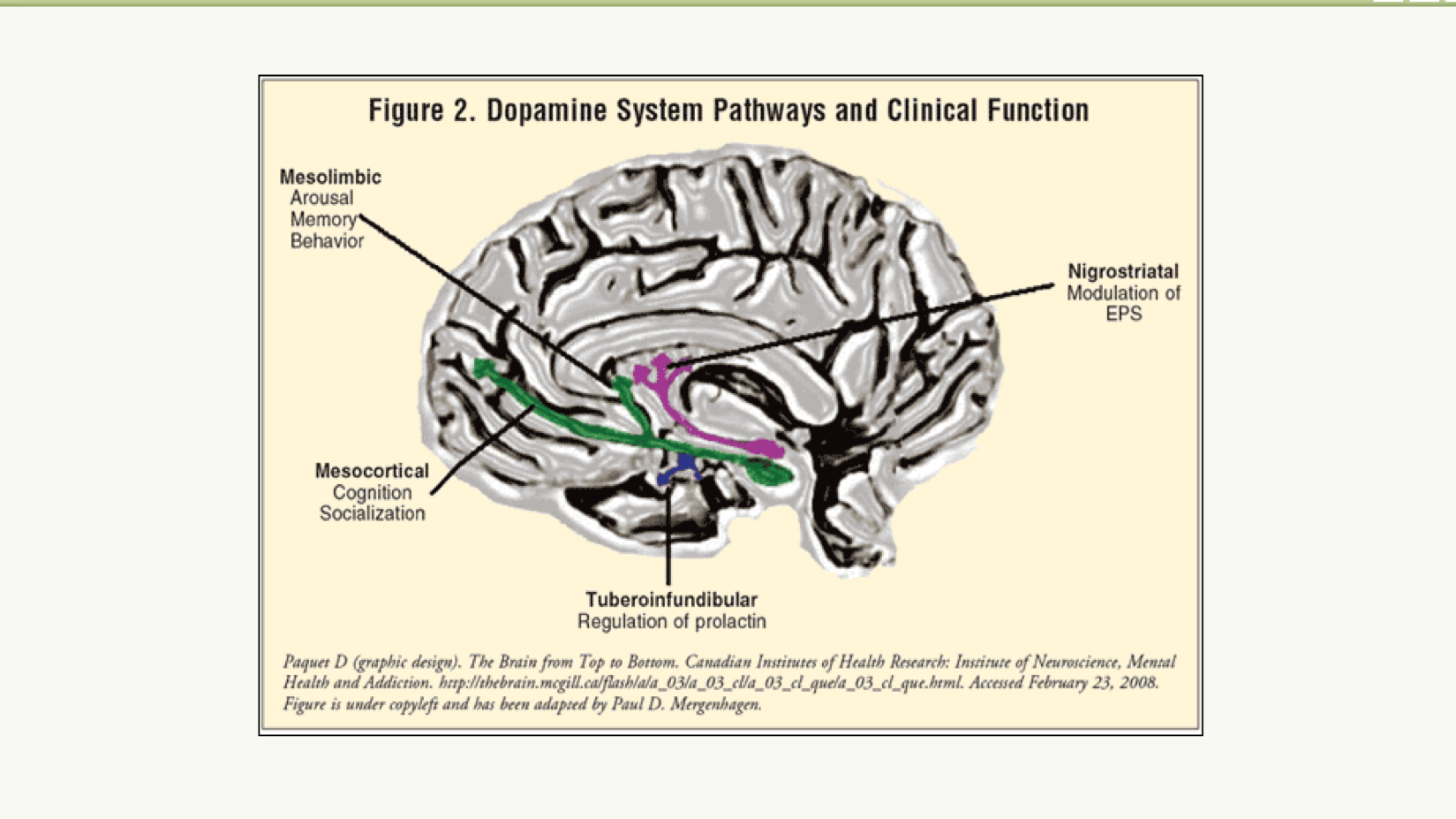
Dopamine system pathways include:
Mesolimbic: arousal, memory, behavior
Mesocortical: cognition, socializaiont
Tuberoinfundibular: regulation of prolactin
Nigrostriatal: modulation of EPS
{kind=link}
Answer
- True
- False
Question 8
{kind=link}
Answer
-
Dopamine deficiency in the basal ganglia and striatum
-
Overactive cholinergic system
-
Dopaminergic/serotonergic or dopaminergic/cholinergic imbalance in the nucleus accumbens
-
Blockade of the striatal dopamine receptors
Question 9
Question
What are risk factors for dystonia
Answer
-
Young age
-
H/O ECT
-
Male gender
-
High potency neuroleptics - Haldol, Prolixin
-
Comorbid medical conditions
Question 10
{kind=link}
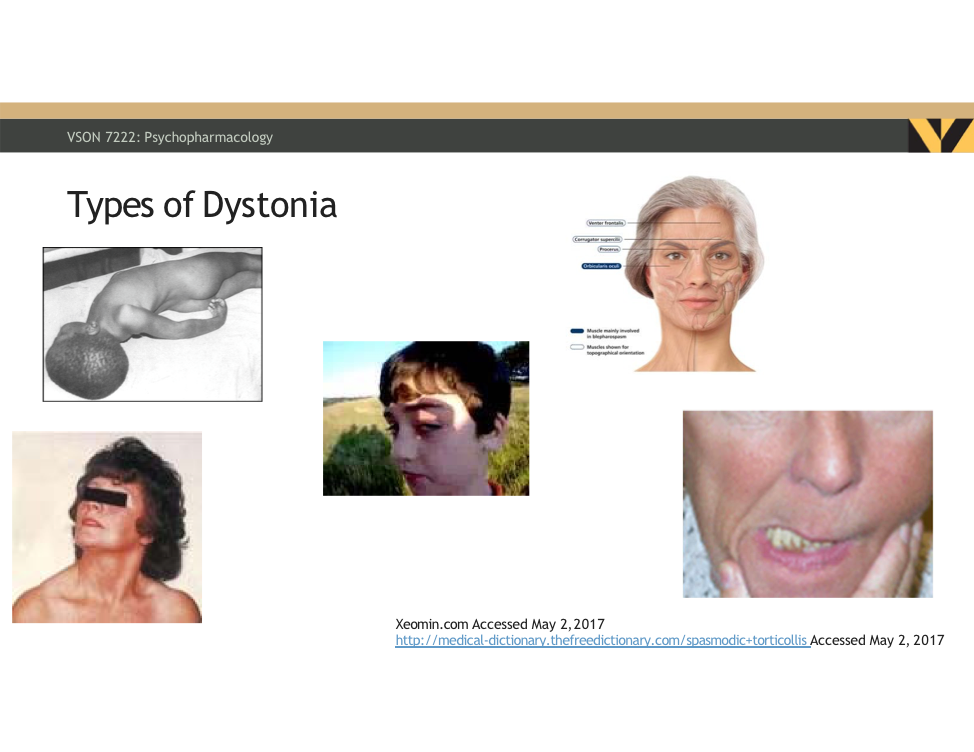
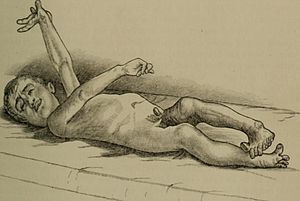
Answer
-
Opisthotonos
-
Blepharospasm
-
Torticollis
-
Oculogyric crisis
-
Oro-mandibular
Question 11
Question
The MOA for akathisia, from the Greek meaning "inability to sit", is:
Answer
-
Dopamine deficiency in the basal ganglia and striatum
-
Dopaminergic/serotonergic or dopaminergic/cholinergic imbalance in the nucleus accumbens, Overstimulation of locus coeruleus.
-
Blockade of the striatal dopamine receptors
-
Striatal dopaminergic hypersensitivity
Question 12
Question
Which of the following agents cause akathisia
Answer
-
SSRI
-
Second generation antipsychotics
-
Antiemetics
-
CCB
-
Anti-anxiolytics
Question 13
Question
What are some differentials for akathisia
Answer
-
GAD
-
ADHD
-
Agitation
-
MDD
Question 14
Question
What are clinical presentation of akathisia
Answer
-
Restlessness
-
Breaking out into song & dance for no reason
-
Fidgety movements/leg swinging
-
Marching in place
-
Rocking from one foot to another
-
Picking
Question 15
Question
The risk factors for akathisia include
Answer
-
Advanced age
-
Affective disorder
-
Cognitive impairment
-
Female impersonator performer
-
Female
-
H/O akathisia
-
Iron deficiency
-
High dose/potency/neuroleptics
Question 16
Question
Pathophysiology of pseudoparkinsonism is:
Answer
-
Dopamine deficiency in the basal ganglia and striatum
-
Dopaminergic/serotonergic or dopaminergic/cholinergic imbalance in the nucleus accumbens
-
Blockade of the striatal dopamine receptors and depletion of pre-synaptic celft
-
Striatal dopaminergic hypersensitivity and cholinergic deficiency in the basal ganglia
Question 17
Question
Parkinsonism = [blank_start]bradykesia[blank_end]
Pseudoparkinsonism = [blank_start]apraxic slowness[blank_end]
Answer
-
bradykesia
-
apraxic slowness
-
bradykinesia
-
apraxic slowness
Question 18
Question
Parkinsonism = [blank_start]resting tremor[blank_end]
Pseudoparkinsonism = [blank_start]essential tremor, myoclonus[blank_end]
Answer
-
resting tremor
-
essential tremor, myoclonus
-
resting tremor
-
essential tremor, myoclonus
Question 19
Question
Parkinsonism = [blank_start]lead pipe rigidity[blank_end]
Pseudoparkinsonism = [blank_start]paratonic rigidity[blank_end]
Answer
-
lead pipe rigidity
-
paratonic rigidity
-
lead pipe rigidity
-
paratonic rigidity
Question 20
Question
Parkinsonism = [blank_start]postural instability[blank_end]
Pseudoparkinsonism = [blank_start]frontal ataxia[blank_end]
Answer
-
postural instability
-
frontal ataxia
-
postural instability
-
frontal ataxia
Question 21
Question
Parkinsonism = [blank_start]Slow, shuffling gait with festination[blank_end]
Pseudoparkinsonism = [blank_start]Slow, shuffling apraxic gait[blank_end]
Answer
-
Slow, shuffling gait with festination
-
Slow, shuffling apraxic gait
-
Slow, shuffling gait with festination
-
Slow, shuffling apraxic gait
Question 22
Question
What are risk factors for pseudoparkinsonism?
Answer
-
Female
-
Male
-
Advanced age
-
Central DA receptor binding agents, Metclopramide, phenothiazines
-
AIDS
-
Cancer
Question 23
Question
Tardive dyskinesia
Answer
-
If identified early can be reversed
-
is not reversible
-
increased risk with increased use
-
increased use does not cause increases risk
-
early onset
-
late onset
Question 24
Question
MOA for tardive dyskinesia
Answer
-
Striatal dopaminergic hypersensitivity
-
Cholinergic deficiency within basal ganglia
-
Oxidative stress and cell injur
-
Genetic susceptibility
-
Glutamate-induced excitotoxicity
-
GABA mediated neuronal dysfunction
-
Blockade of the striatal dopamine receptors
Question 25
Question
Which medications most commonly cause tardive dyskinesia?
Answer
-
Meoclopramide
-
Alpha adrenergic agonists
-
SGA
-
FGA
Question 26
Question
Clinical presention of tardive dyskinesia
Answer
-
Choreiform - characterized by jerky, involuntary movements, chiefly of the face and extremitiesImage:Chorea (binary/octet-stream)
-
Athetoid - characterized by slow, involuntary, convoluted, writhing movements of the fingers, hands, toes, and feet and in some cases, arms, legs, neck and tongue
-
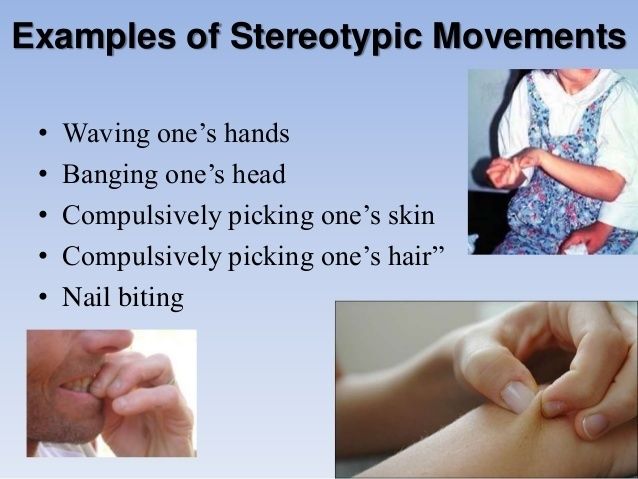
Stereotypic - petitive, nonfunctional motor behavior (e.g., hand waving or head banging), that markedly interferes with normal activities or results in bodily injury.
{kind=link}
{kind=link}
{kind=link}
Question 27
Question
EPS can be caused by antiemetics, antieliptics, psychotropics, cardiovascular agents and Levodopa
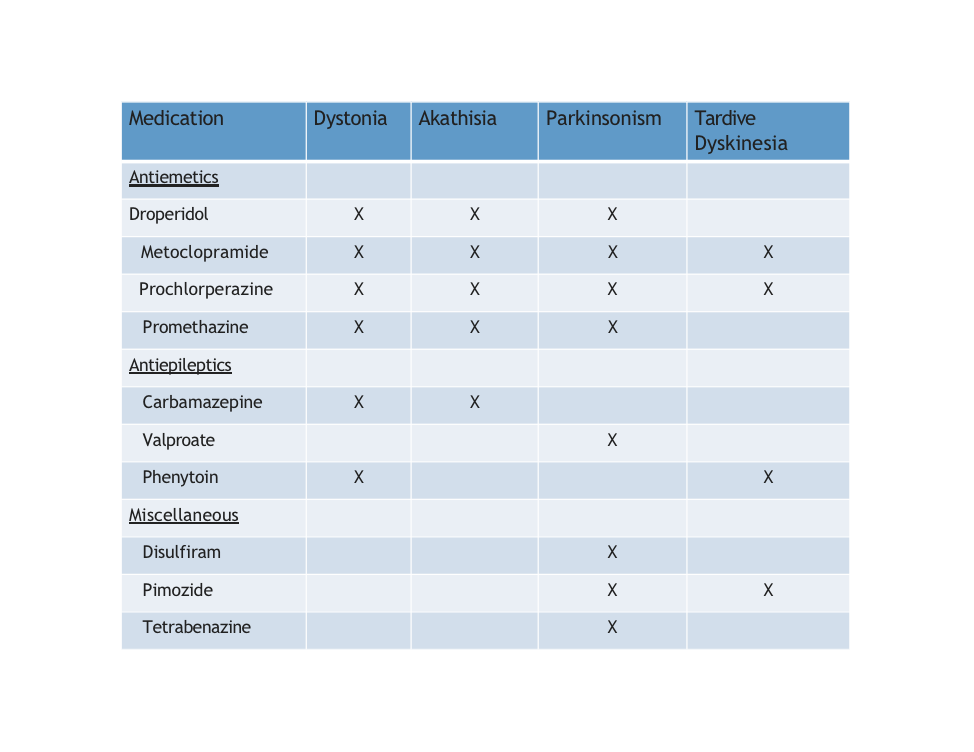{kind=link}
Answer
- True
- False
Question 28
Question
EPS can be caused by antiemetics, antieliptics, psychotropics, cardiovascular agents and Levodopa
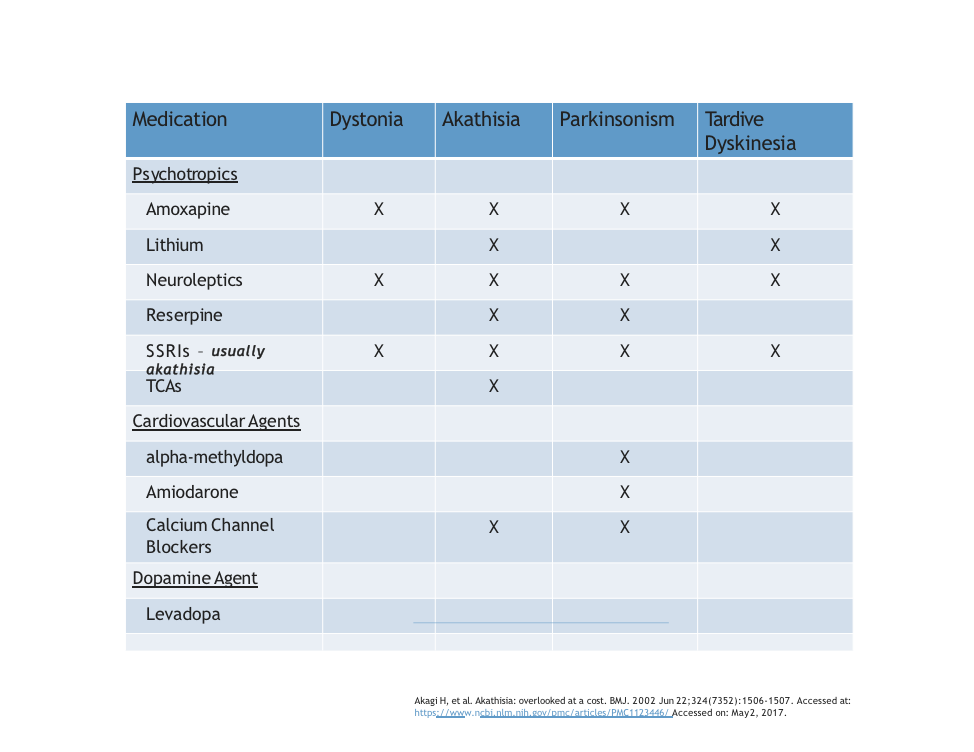{kind=link}
Answer
- True
- False
Question 29
Question
The following drugs cause all four movement disorders: dystonia, akathisia, Parkinsonism, tardive dyskinesia
Answer
-
Metoclopramide
-
Prochloraperazine
-
Amoxapine
-
Neuroleptics
-
SSRI
-
Levodopa
Question 30
Question
How often should the Abnormal Involuntary Movement Scale (AIMS) be administered?
Answer
-
Baseline then every week x4 then every 3 months
-
Baseline then every week x2 then every 12 months
-
Baseline then every week x2 then every 6 months
Question 31
Question
What are overall tips for treatment of EPS?
Answer
-
Stop offending agen (if possible)
-
Reduce the dose
-
Switch to a second generation antipsychotic
-
Treat prophylactically
-
A wing and prayer and refer to anyone else
Question 32
Question
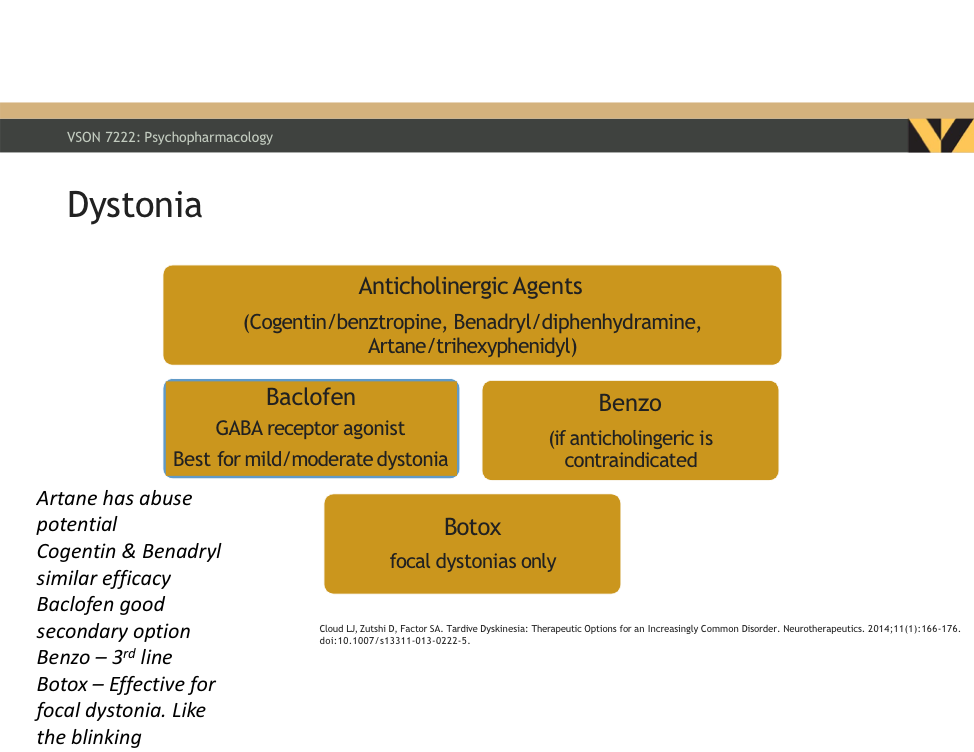
Dystonia put in order of line of treatment
First line = [blank_start]anticholinergic agents[blank_end]
Second line = [blank_start]Baclofen[blank_end]
Third line = [blank_start]Benzo[blank_end]
Fourth line - [blank_start]Botox[blank_end]
Answer
-
anticholinergic agents
-
Baclofen
-
Benzo
-
Botox
Question 33
{kind=link}
Answer
- True
- False
Question 34
Question
Drug of choice for dystonia is
Answer
-
Beta-blockers, anticholinergics, benzodiazepines, 5-HT2A receptor antagonist, mirtazapine
-
Anticholinergics (benztropine, diphenhydramine, trihexyphenidyl)
-
Clonzaepam, ginkgo biloba
Question 35
Question
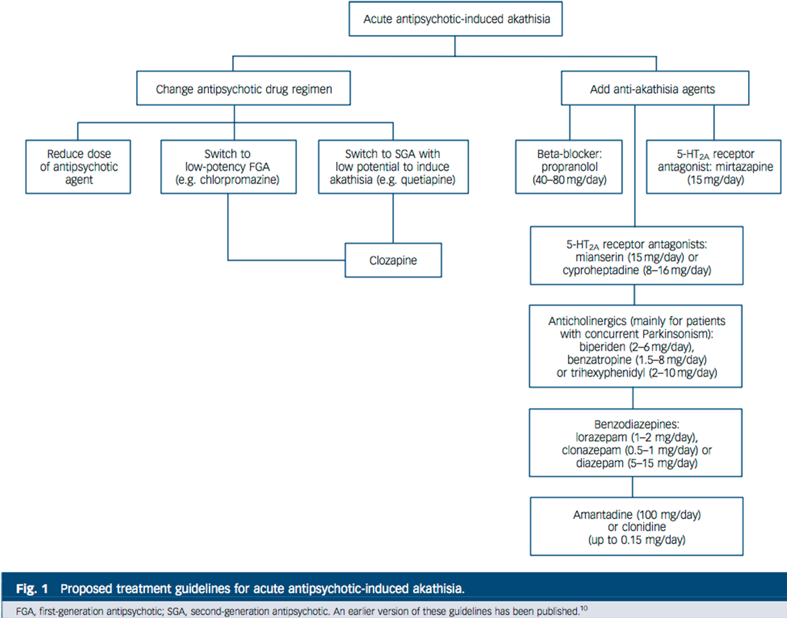
Drugs of choice for akathisia include
Answer
-
Anticholinergics (benztropine, diphenhydramine, trihexyphenidyl)
-
Beta-blockers, benzodiazepines, 5-HT2A receptor antagonist, mirtazapine
-
Clonazepam, ginkgo biloba
Question 36
Question
Mirtazapine (Remeron)
Answer
-
Used in low doses to treat akathisa
-
Used in low doses to treat dystonia
-
Alpha-adrenergic receptor antagonist
-
Alpha-adrenergic receptor agonist
-
Antagonizes 5-HT2 and 3 receptors
Question 37
{kind=link}
Answer
- True
- False
Question 38
Question
Which drugs are used to treat pseudoparkinsonism?
Answer
-
Cogentin (benztropine)
-
Symmetrel (amantadine)
-
Benzodiazepines
-
Mirtazapine (Remeron)
-
Diphenhydramine (Benadryl)
Question 39
Question
MOA for amantadine (Symmetrel) is
Answer
-
Dopamine agonist
-
Dopamine antagonist
-
5-HT2 agonist
-
5-HT2 antagonist
Question 40
Question
Side effects for benztropine (Cogentin) include
Answer
-
Dry mouth
-
Hypotension
-
Diarrhea
-
Constipation
-
Cognitive impairment
-
Sialorrhea
Question 41
Question
Side effects for amantadine (Symmetrel) include:
Answer
-
Hypotension
-
Hypertension
-
Agitation
-
Sedation
-
Worsening s/s of psychosis
Question 42
Question
Which drugs are used in the treatment of tardive dyskinesia
Answer
-
Diltiazem
-
Baclofen
-
Galantamine
-
Clonazepam
-
Ginkgo biloba
Question 43
Question
What is the first FDA approved medication for Tardive Dyskinesia
Answer
-
Velbeazine (Ingrezza)
-
Benztropine (Cogentin)
-
Trihexphenidyl (Artane)
-
Amantadine (Symmetrel)
Question 44
Question
What is the MOA for valbenazine (Ingrezza)?
Answer
-
Blocks alpha-adrenergic receptors and antagonizes 5-HT2 and 3 receptors
-
Reversible inhibition of vesicular monoamine transporter 2 (VMAT2), a transporter that regulates monoamine uptake from the cytoplasm to the synaptic vesicle for storage and release
-
Increase in synthesis and release of dopamine, and inhibition of dopamine uptake.
-
Selective M1 muscarinic acetylcholine receptor antagonist. It is able to discriminate between the M1 (cortical or neuronal) and the peripheral muscarinic subtypes (cardiac and glandular)
Question 45
Question
Acute [blank_start]laryngeal[blank_end] dystonia is considered a medical emergency.
Must seek treatment immediately. May require IV diphenhydramine
Answer
-
laryngeal
Question 46
Question
Velbenazine is extensively metabolized by hydrolysis to form active metabolite
and by oxidative metabolism to form mono-oxidized valbenazine and other minor metabolites
Answer
- True
- False
Question 47
Question
High fat meals may [blank_start]decrease[blank_end] absorption of valbenazine (Ingrezza)
Answer
-
decrease
-
increase
Question 48
Question
Common adverse side effects of valbenazine (Ingrezza) include:
Answer
-
Fatigue
-
HA
-
Constipation
-
Diarrhea
-
UTI
-
Somnolence
Question 49
Question
Warnings for valbenazine (Ingrezza) include:
Answer
-
Somnolence
-
QTc prolongation
-
Pregnancy/breastfeeding
-
Hypertension
Question 50
Question
Valbenazine should not be used in:
Answer
-
Severe renal impairment (< 30 mL/min)
-
CHF
-
Cirrhosis
-
Pancreatitis
Question 51
Question
Strong 3A4/2D6 inhibitors: [blank_start]Increase[blank_end] valbenazine concentration
Strong 3A4 inducer: [blank_start]Decrease[blank_end] valbenazine concentration
Answer
-
Increase
-
Decrease
-
Increase
-
Decrease
Question 52
Question
Valbenazine (Ingrezza) interacts with MAOIs by [blank_start]increasing[blank_end] the monamine NT in the synapse
Answer
-
increasing
-
decreasing
Question 53
Question
Valbenazine (Ingrezza) interacts with digoxin and [blank_start]increase[blank_end]s the digoxin concentration by p-glycoprotein [blank_start]inhibtion[blank_end]
Answer
-
increase
-
decreases
-
inhibtion
-
inducer
Question 54
Question
Deutetrabenazine (Austedo) is used for the treatment of chorea and schizophrenia/schizoaffective disorder. It is metabolized by CYP2D6
Answer
- True
- False
Want to create your own Quizzes for free with GoConqr? Learn more.