23134012
Description
Quiz by Tobar MacPhail, updated more than 1 year ago
|
|
Created by Tobar MacPhail
over 4 years ago
|
|
Question 1
Question
What is multi-morbidity?
Answer
-
Dying but not knowing which condition caused it
-
Having three or more health conditions
-
Having one condition but with multiple symptoms
Question 2
Question
According to research by Ekelund (2015) a brisk walk of how long is enough to reduce an individual's risk of early death?
Answer
-
5 minutes
-
10 minutes
-
20 minutes
-
30 minutes
-
50 minutes
-
120 minutes
Question 3
Question
Which of the following are risk factors for CV disease and stroke in hypertension?
Answer
-
Stystolic BP over 120
-
Systolic BP Over 140
-
Diastolic BP Over 80
-
Diastolic BP over 90
Question 4
Question
[blank_start]Type 1 Diabetes[blank_end]: A condition from birth where the body produces insufficient insulin. Lifestyle can play a part in management, but is not causative.
[blank_start]Type 2 Diabetes[blank_end]: A condition that has lifestyle factors in it's development, as well as it's management when present. Over time insulin sensitivity becomes reduced and blood sugar becomes less able diffuse out of blood vessels.
Answer
-
Type 1 Diabetes
-
Type 2 Diabetes
Question 5
Question
For the majority of people, normal blood sugar ranges between [blank_start]4.0[blank_end] to [blank_start]6.0[blank_end] mmol/L ([blank_start]72[blank_end] to [blank_start]108[blank_end] mg/dl) when fasting, and up to [blank_start]7.8[blank_end] mmol/L ([blank_start]140[blank_end]mg/dl) 2 hours after eating.
Answer
-
4.0
-
6.0
-
72
-
108
-
7.8
-
140
Question 6
Question
An individual without Diabetes Mellitus will co-ordinate hormonal and metabolic events to ensure the maintenance of [blank_start]glucose homeostasis[blank_end].
In Diabetes, [blank_start]Insulin[blank_end] and other hormonal responses do not respond in the normal manner so the balance between [blank_start]peripheral[blank_end] glucose utilisation and [blank_start]hepatic[blank_end] glucose production may be disturbed.
There are many factors that will affect this response during a single bout of exercise.
Answer
-
glucose homeostasis
-
uninterrupted insulin production
-
Insulin
-
peripheral
-
central
-
aortic
-
hepatic
-
renal
-
thyroid
Question 7
Question
Which of the following are evidence based components/considerations of Type 2 diabetes management:
Answer
-
Sustained fasting
-
Shorter durations of exercise to manage glucose levels
-
Timing of exercise sessions around food intake/glucose levels
-
Extraneous insulin (when indicated)
-
Nutritional management/planning
-
Exercising for 2 or more hours to shunt glucose levels down quickly
-
Regular exercise
-
Vasodilatory drugs to allow for increased glucose clearance
-
Oral agents such as metformin
Question 8
Question
Beneficial effects of a single bout of exercise on type 2 diabetes include:
Answer
-
Increased insulin sensitivity
-
Greater glucose uptake by muscle cells
-
Lower blood sugar levels
-
Sustained reduced blood glucose for 24 hours
-
Decreased insulin sensitivity
Question 9
Question
Long term beneficial effects of exercise on Type 2 diabetes include
Answer
-
Improved sustained glycaemic control
-
Reduction of the blood lipids that can result in reduced glucose transport
-
Reduction in body fat % which is a risk factor in diabetic symptoms
-
Prevention of the development of type 2 diabetes for certain people
-
Increased sugar secretion in urine
-
Improved amylaze activity in glucose metabolism
Question 10
Question
Possible risks in exercising with type 2 diabetes include:
Systemic:
[blank_start]Retinal[blank_end] Haemorrhage
[blank_start]Increased[blank_end] proteinurea
Accelaration of [blank_start]microvascular lesions[blank_end]
Cardiovascular:
Cardiac [blank_start]arrythmias[blank_end]
Ischaemic [blank_start]heart disease[blank_end]
[blank_start]Raised[blank_end] blood pressure
Post exercise orthostatic [blank_start]hypertension[blank_end]
Metabolic:
[blank_start]Hyper[blank_end]glycaemia
Ketosis
Musculoskeletal:
[blank_start]Foot[blank_end] ulcers
Injury related to [blank_start]neuropathy[blank_end]
Degenerative [blank_start]joint[blank_end] disease
Answer
-
Retinal
-
Carotid
-
Cerebrovascular
-
Increased
-
Decreased
-
microvascular lesions
-
oxidative stress in the kidneys
-
breakdown of lipids
-
arrythmias
-
failure
-
heart disease
-
pain
-
Raised
-
Lowered
-
hypertension
-
hypotension
-
Hyper
-
hypo
-
Foot
-
Mouth
-
Abdominal
-
neuropathy
-
Osteopenia
-
joint
-
muscle
Question 11
Question
What are the signs/symptoms of a hypoglycaemic episode?
Answer
-
Frank haemoptysis
-
Palpitations/tachycardia
-
Palpitations/bradycardia
-
Blurred vision
-
Sweating
-
Vocal tics
-
Being hungry
-
Loss of appetite
-
Headache
-
Loss of concentration
Question 12
Question
Treating a hypoglycaemic episode should be done immediately. You can do this by eating or drinking [blank_start]15[blank_end] to [blank_start]20[blank_end] grams of a fast acting carbohydrate, this could include
[blank_start]3[blank_end] glucose or dextrose tablets
[blank_start]5[blank_end] jelly babies
a [blank_start]small[blank_end] glass of a sugary (non-diet) drink
a small carton of pure fruit juice
a tube of [blank_start]glucose[blank_end] gel
Answer
-
15
-
30
-
20
-
60
-
3
-
2
-
1
-
5
-
4
-
6
-
8
-
10
-
small
-
large
-
glucose
-
ketone
Question 13
Question
Which of the following are CONTRAINDICATIONS to exercise in type 2 diabetes?
Answer
-
Retinal haemorrhage
-
Illness or infection
-
Blood glucose >13.8 mmol/L and ketones present
-
Blood glucose < 3.9 mmol/L
-
Blood glucose < 4.5mmol/L
-
Blood glucose >12mmol/L with no ketones present
-
Foot pain
-
The usage of an insulin pump
Question 14
Question
What are PRECAUTIONS in exercise prescription for Type 2 diabetes?
Answer
-
Whether there is a readily available source of carbohydrate
-
Consumption of adequate fluids before, during, and after exercise
-
Good foot care
-
Carry medical identification
-
Retinal haemorrhage
-
Illness or infection
Question 15
Question
[blank_start]Chronic fatigue syndrome[blank_end] (CFS) is characterised by [blank_start]persistent[blank_end], medically unexplained fatigue, as well as symptoms such as musculoskeletal [blank_start]pain[blank_end], sleep disturbance, headaches and impaired [blank_start]concentration[blank_end] and [blank_start]short[blank_end] term memory. CFS presents as a common, debilitating and serious health problem
Answer
-
Chronic fatigue syndrome
-
Cystic fibrosis
-
Cerebral Failure Syndrome
-
persistent
-
intermittent
-
pain
-
weakness
-
dystrophy
-
concentration
-
vision
-
fluid intake
-
short
-
long
Question 16
Question
Graded exercise therapy is a staged approach to exercise for people with ME/CFS.
Exercise is based on the person's [blank_start]current[blank_end] level of activities (ADLs, relapses, goals) and should include [blank_start]sleep[blank_end] and relaxation strategies to manage recovery and acute exercise malaise.
Goals should be [blank_start]long term[blank_end], and the physiological context of exercise should be explained, including the potential to [blank_start]increase[blank_end] symptoms in the short term.
Start with [blank_start]low intensity[blank_end] exercise sustainable independent of fluctuations. Frequency should be progressed first, then duration.
There are [blank_start]no known[blank_end] pharmaceutical treatments to manage ME, and evidence for pacing strategies is [blank_start]insufficient[blank_end]: The ME association currently recommends pacing as the preferred approach to activity management.
Strategies that should be avoided include unsupervised [blank_start]vigorous[blank_end] exercise, encouraging of exercising substantially [blank_start]less[blank_end] than full capacity to reserve energy (envelope theory), encouraging [blank_start]complete rest[blank_end] during a relapse, or having exercise guided by inexperienced practitioners.
Answer
-
current
-
desired
-
sleep
-
long term
-
short term
-
increase
-
decrease
-
low intensity
-
high intensity
-
high volume
-
power
-
no known
-
several
-
insufficient
-
significant
-
vigorous
-
light
-
less
-
more
-
complete rest
-
manageable activity
Question 17
Question
Which of these is NOT an absolute contraindication to exercise?
Answer
-
Unstable Angina
-
Resting systolic >180mmhg
-
Resting diastolic >1000mmhg
-
uncontrolled tachycardia >100bpm
-
unstable or acute heart failure
-
febrile illness
-
uncontrolled conditions
-
blood glucose <4.5mmol/L
Question 18
Question
[blank_start]Deconditioning[blank_end] is associated with changes in muscle (sarcopenia) and bone, cardiovascular, respiratory, and metabolic changes.
Simply reducing normal activity levels results in elements of this problem: reductions in weekly weight bearing exercise result in a loss of bone mass in both men and women.
Answer
-
Deconditioning
Question 19
Question
What does FITT stand for?
F = [blank_start]Frequency[blank_end]
I = [blank_start]Intensity[blank_end]
T = [blank_start]Time[blank_end]
T = [blank_start]Type[blank_end]
Answer
-
Frequency
-
Intensity
-
Time
-
Type
Question 20
Question
When performing exercise with patients that are on multiple drugs, all exercise is contra-indicated due to the possibility of adverse reactions to combined drugs.
Answer
- True
- False
Question 21
Question
Which of the following are psychosocial factors that may influence exercise adherence?
Answer
-
Thoughts, beliefs, and attitudes
-
Knowledge and understanding
-
Locus of control
-
Previous exercise experience
-
Self efficacy
-
Fear avoidance
-
Compliance
-
Culture
-
Environment
Question 22
Question
The most frequently cited reason for dropping out of an exercise programme is lack of [blank_start]time[blank_end]
Answer
-
time
Question 23
Question
[blank_start]Motivational interviewing[blank_end] (MI) is a counselling technique that can be modified based on target group to change [blank_start]maladaptive[blank_end] behaviours, elicit ambivalences, and [blank_start]enhance[blank_end] self-efficacy for making changes.
MI is a collaborative, [blank_start]person[blank_end]-centred form of guiding to elicit and strengthen motivation for [blank_start]change[blank_end]. It is delivered over an [blank_start]extended[blank_end] period of time. It is particularly useful for helping those who are [blank_start]less[blank_end] ready to change, and has been found effective in promoting change (at least in the [blank_start]short[blank_end] term) with a wide range of health behaviours, including [blank_start]diet[blank_end] and physical activity. All health professionals can be trained in it's use.
The principles of MI are illustrated by the acronym RULE.
R: [blank_start]Resist the righting reflex[blank_end]. Practitioners should [blank_start]avoid trying[blank_end] to "put right" patient's behaviours.
U: [blank_start]Understand[blank_end] and explore the patient's own motivations
L: [blank_start]Listen with[blank_end] empathy
E: [blank_start]Empower[blank_end] the patient, encouraging hope and optimism.
Answer
-
Motivational interviewing
-
Myocardial Infarction
-
Multiple Interventions
-
maladaptive
-
enhance
-
inhibit
-
person
-
therapist
-
change
-
exercise
-
extended
-
extremely brief
-
less
-
more
-
diet
-
short
-
long
-
Resist the righting reflex
-
Retrain the wrong behaviours
-
avoid trying
-
attempt as early as possible
-
Understand
-
Unwrap
-
Listen with
-
Lack
-
Linger upon
-
Empower
-
Endure
Question 24
Question
Which of the following are examples of CHANGE TALK and not SUSTAIN TALK
Answer
-
Unable to commit to change
-
Expresses commitment to change
-
Expressing a desire for the status quo
-
Expressing the ability to make the change
-
Sees the need for change
-
Reduced confidence in being able to make the change
-
Expressing a wish to change
Question 25
Question
Preparing to change may contain the following components
D = [blank_start]Desire[blank_end] to change - I would like to
A= [blank_start]Ability[blank_end] - I would be able to
R = [blank_start]Reason[blank_end] = It would enable me
N = [blank_start]Need[blank_end] - I must/I cannot go on like this
Answer
-
Desire
-
Ability
-
Reason
-
Need
Question 26
Question
Mobilising change involves
C = [blank_start]Commitment[blank_end] to change - Likelihood of change "I will"
A = [blank_start]Activation[blank_end] ready for change - "I am ready to"
T = [blank_start]Taking[blank_end] steps - "I went to the exercise class"
Answer
-
Commitment
-
Activation
-
Taking
Question 27
Question
Which of the following are "Evocative questions/discussions" for change:
Answer
-
Asking for elaboration
-
Asking why they fail at exercise so frequently
-
Query extremes
-
Looking backward
-
Looking forward
-
Evoke shame
-
Use change rulers
-
Ask for examples
-
Come alongside
-
OARS
Question 28
Question
Weighing up benefits and costs of changing a behaviour is demotivating and should never be used in clinical practice
Answer
- True
- False
Question 29
Question
Evidence supports the notion that one specific behavioural model should be used to elicit behavioural change. It is ineffective to focus on generic competencies and skills.
Answer
- True
- False
Question 30
Question
Label each of the stages in the stages of change model
{kind=link}
Answer
-
Precontemplation
-
Contemplation
-
Preparation
-
Action
-
Maintenance
Question 31
{kind=link}
Answer
-
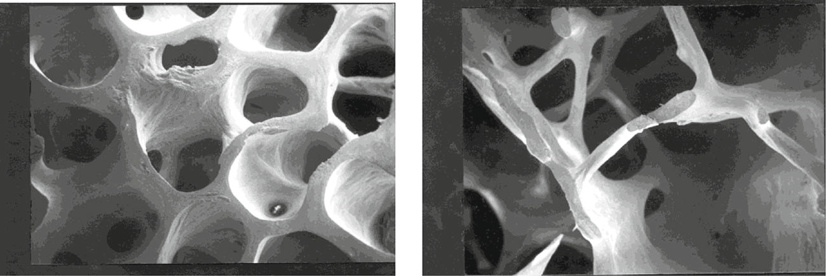
Osteoporosis
-
Bovine Spongiform Encephalopathy
-
Asthma
-
Osteochondritis Dessicans
Question 32
Question
[blank_start]Osteoporosis[blank_end] is a common bone disease characterised by reduced bone mass which is associated with an increased risk of low trauma fractures. Fractures are an important cause of morbidity and patients who suffer hip and vertebral fractures have a decreased life expectancy.
Answer
-
Osteoporosis
Question 33
Question
Bone mineral density as measured at the hip (femoral neck) by Dual energy xray absorptiometry (DEXA) is used to diagnose osteopenia and osteoporosis. Measurements are in bone mass density (BMD). Fill in the blank numbers used to diagnose each condition.
Osteopenia: BMD between [blank_start]1[blank_end]-[blank_start]2.5[blank_end] SD below that of a young normal adult
Osteoporosis: BMD [blank_start]2.5[blank_end] SD below that of a young normal adult.
Severe osteoporosis (established osteoporosis): osteoporosis in the presence of [blank_start]1[blank_end] or more fragility fractures.
Answer
-
1
-
2.5
-
2.5
-
1
Question 34
Question
Which of the following are lifestyle info/advice you can give to a person with osteoporosis to aid prevention of fragility fractures
Answer
-
Encourage walking, especially outdoors, to increase vitamin D production
-
Discourage outdoor walking due to risk of trips or falls
-
Engage in strength training, such as weight training, of different muscle groups
-
Discourage weigh training due to risk of spinal compression fractures
-
Combine many exercise types: balance, flexibility, stretching, endurance, and progressive strengthening
-
Keep exercise to aerobic endurance only to reduce risk of injury
-
Stop smoking and eat a balanced diet
-
Drink alcohol within recommended limits
-
Drink NO alcohol, even moderated intake is associated with fracture risk
-
Refer to the national osteoporosis society for more information
Question 35
Question
People with osteoporosis should be encouraged to minimise exercise, as even though there are some minor benefits to bone mineral density, the risk of deadly hip fractures is far too high. Nutritional interventions should take place for at least six months before regular exercise takes place.
Answer
- True
- False
Question 36
Question
Bisphosphonates such as alendronate acid and risedronate sodium are types of [blank_start]antiresorptive[blank_end] medication used in the treatment of [blank_start]osteoporosis[blank_end] that reduce the risk of vertebral fracture when given with calcium and [blank_start]vitamin D[blank_end] supplements.
Answer
-
antiresorptive
-
osteoporosis
-
vitamin D
Question 37
Question
Label the BMI classifications (BMI in kg/m2)
Classification
Healthy - [blank_start]18.5[blank_end]-[blank_start]24.9[blank_end]
Overweight - [blank_start]25[blank_end]-[blank_start]29.9[blank_end]
Obese 1 - [blank_start]30[blank_end]-[blank_start]34.9[blank_end]
Obese 2 -[blank_start]35[blank_end]-[blank_start]39.9[blank_end]
Obese 3 - [blank_start]≥ 40[blank_end]
Answer
-
18.5
-
24.9
-
25
-
29.9
-
30
-
34.9
-
35
-
39.9
-
≥ 40
-
≥ 50
-
25.5
-
32.5
-
33
-
42.5
-
43
-
52.5
-
53
-
62.5
-
≥ 70
Question 38
{kind=link}
Answer
-
74
-
84
-
94
-
104
-
114
-
74
-
84
-
94
-
104
-
114
-
82
-
92
-
102
-
112
-
122
-
82
-
92
-
102
-
112
-
122
-
80
-
90
-
100
-
110
-
80
-
90
-
100
-
110
-
88
-
94
-
100
-
102
-
115
-
130
-
88
-
94
-
100
-
102
-
115
-
130
-
No increased risk
-
Increased risk
-
High risk
-
Very high risk
-
No increased risk
-
Increased risk
-
High risk
-
Very high risk
-
No increased risk
-
Increased risk
-
High risk
-
Very high risk
-
No increased risk
-
Increased risk
-
High risk
-
Very high risk
-
No increased risk
-
Increased risk
-
High risk
-
Very high risk
-
No increased risk
-
Increased risk
-
High risk
-
Very high risk
-
No increased risk
-
Increased risk
-
High risk
-
Very high risk
-
No increased risk
-
Increased risk
-
High risk
-
Very high risk
-
No increased risk
-
Increased risk
-
High risk
-
Very high risk
Question 39
{kind=link}
Answer
-
37
-
94
-
31.5
-
80
-
40
-
102
-
35
-
88
-
0.90
-
0.85
Question 40
Question
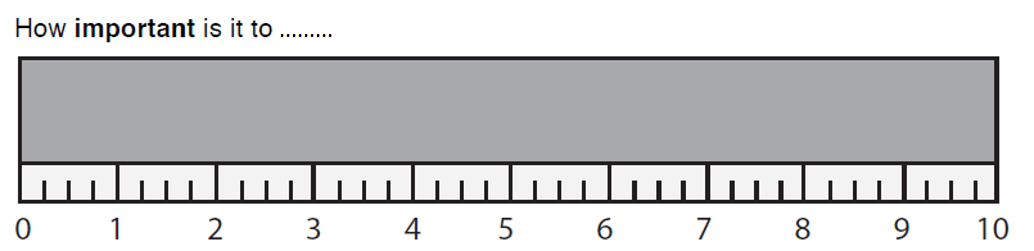
The full text in this image has been removed. Complete the sentences below.
The image displays a [blank_start]change ruler[blank_end] which is used to determine how ready a patient is for [blank_start]change[blank_end].
When using you can ask them how realistic or how confident they are about their response, or why 6 rather than 4, and what could help them/what support they need to score higher.
{kind=link}
Answer
-
change ruler
-
change
Question 41
Question
Link the description to the behaviour change theory/model:
[blank_start]Cognitive dissonance theory[blank_end] - A situation involving conflicting attitudes, beliefs or behaviors produces a feeling of mental discomfort leading to an alteration in one of the attitudes, beliefs or behaviors to reduce the discomfort and restore balance.
[blank_start]Diffusion of innovation theory[blank_end] - Explains how, over time, an idea or product gains momentum and spreads through a specific population or social system. The end result of this is that people, as part of a social system, adopt a new idea, behavior, or product. Adoption means that a person does something differently than what they had previously (i.e., purchase or use a new product, acquire and perform a new behavior, etc.). The key to adoption is that the person must perceive the idea, behavior, or product as new or innovative.
[blank_start]Health belief model[blank_end] - Based around the foundation that health related behaviours are predicated upon 1) the desire to avoid illness and/or recover from illness, and 2) the belief that a specific health action will avoid or help recover from said illness. An individual's course of action depends on the person's perceptions of the benefits and barriers of those health behaviours. There are six components of these beliefs and barriers. 1. Perceived susceptibility. 2. Perceived severity. 3. Perceived benefits. 4. Perceived barriers. 5. Cue to action, and 6. Self efficacy.
[blank_start]Motivational interviewing[blank_end] - A person centred counselling style for eliciting behavioural change by helping clients to explore and resolve ambivalence via focused and goal directed discussions. The core foundation is bringing about "change talk" and evoking patient motivation to make positive changes. The approach relies on non-judgement of the patient and accepting them how they are.
[blank_start]Self efficacy[blank_end] - In essence, a person's belief in their own competence and ability to achieve/perform a given goal/task. This can interact with all aspects of a person's life, but has particular relevance when it comes to making changes to health behaviours, where without this, a person will have minimal motivation to change as they will believe it outside the scope of their capabilities.
[blank_start]Social cognitive learning theory[blank_end] - A framework of learning and change based upon the observation of others within the context of social interactions, experiences, and outside media influences. "People do not learn new behaviours solely by trying them and either succeeding or failing, but rather the replication of the actions of others"
[blank_start]Theory of reasoned action[blank_end] - Aims to explain the relationship between attitudes and behaviours in human action. Mainly used to predict how individuals will behave based on their pre-existing attitudes and behavioural intentions. "An individual's decision to engage in a particular behaviour is based on the outcomes the individual expects will come as a result of performing it".
Transtheoretical model/[blank_start]stages of change theory[blank_end] - A framework based on the idea that individuals move through six stages of change: precontemplation, contemplation, preparation, action, maintenance and termination.
Answer
-
Cognitive dissonance theory
-
Diffusion of innovation theory
-
Health belief model
-
Motivational interviewing
-
Self efficacy
-
Social cognitive learning theory
-
Theory of reasoned action
-
stages of change theory
Want to create your own Quizzes for free with GoConqr? Learn more.