23353807
Description
Quiz by Darryl Chung, updated more than 1 year ago
|
|
Created by Darryl Chung
over 4 years ago
|
|
Question 1
Question
MENOPAUSAL LOW MOOD
A 48 year-old woman presents to your GP surgery with low mood and loss of libido. This is causing a strain on her marriage and her husband complains that she has been "snappy" all the time in spite of sleeping quite well at night. Her periods have become more irregular, with the last one some 4 months ago. She is usually very upbeat and still goes to work as a receptionist in a business firm and enjoys her daily walks. What is your most appropriate management?
{kind=link}
Answer
-
Commence propranolol 40 mg twice daily.
-
Recommend using Replens vaginal lubricant.
-
Advise seeking a marriage counsellor.
-
Offer a trial of venlafaxine 37.5 mg twice daily.
-
Refer for cognitive behavioural therapy.
Question 2
Question
HOT FLUSHES
A 51 year-old female multi-regional drug representative attends your clinic complaining of poor sleep as she feels unbearably hot and sweaty in spite of leaving the window ajar. As she has not seen her period for 8 months and has not been in a relationship for 5 years, she feels that this is her menopause but states that she does not want HRT as her mother had developed breast cancer at the age of 44 years and her 53 year-old cousin was recently also diagnosed with breast cancer, having taken HRT. She denies smoking or alcohol and does regular weight training in the gym to keep toned. Which one recommendation is the most appropriate for her?
{kind=link}
Answer
-
Offer daily Vagifem as she will be at no greater risk with transdermal HRT of developing breast cancer than the general population.
-
She can safely have oestrogen-only HRT as there is little or no increased risk of breast cancer.
-
Prescribe clonidine as it is licensed for treatment of hot flushes.
-
Offer citalopram as an off-label two-week trial.
-
Refer for genetic specialist counselling.
Question 3
Question
NON-HRT THERAPY
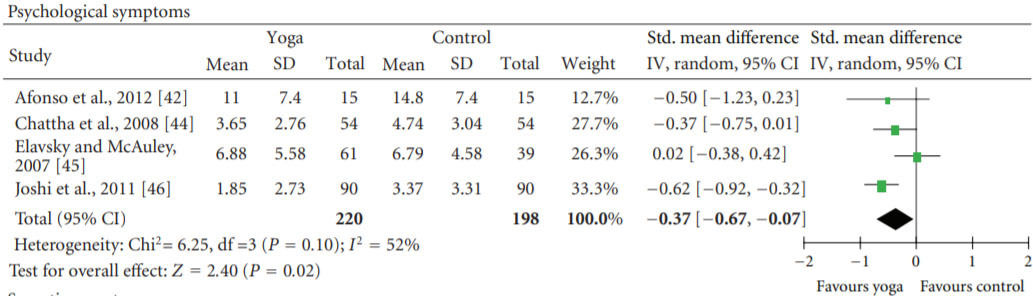
A 46 year-old woman who has been having hot flashes and irregular periods over the past 6 months comes to see you over concerns of recent low mood and anxiety. She is not keen to start medication and asks you if yoga would be helpful. You promise to look into it and get back to her. You come across a relevant meta-analysis of randomised controlled trials (Cramer, et al, 2012) and look at the forest plot comparing the short term effect on psychological menopausal symptoms of yoga to that of exercise or no intervention. From this study, what can you conclude?
{kind=link}
Answer
-
(A) Overall, there is significant benefit of yoga for treatment of menopausal psychological symptoms.
-
(B) Only the study of Elavsky and McAuley shows no significant difference between yoga and exercise/no intervention.
-
(C) Afonso et al. is the smallest of the trials in this meta-analysis.
-
(D) There is strong evidence for the beneficial effects of yoga on all symptoms of menopause.
-
(E) Joshi et al. conclusively demonstrate yoga is associated with long-term improvement of menopausal psychological symptoms.
Question 4
Question
PERIMENOPAUSAL CONTRACEPTION
A 48 year-old sexually active woman who has completed her family attends your clinic on her birthday and inquires whether her 4 year-old Mirena IUS should be removed since she thinks that she may be going through the "changes" as she has been experiencing troublesome hot flushes, mood swings, fatigue and dryness "down below". Apart from initial spotting, she has never had a period since she had the IUS inserted. Which of the following are viable options for her?
Image:
Mirena (binary/octet-stream)
{kind=link}
Answer
-
(A) Offer substitution with combined hormonal oral contraceptive.
-
(B) Switch IUS to Nexplanon and offer oestrogen-only HRT.
-
(C) The IUS can be safely removed once there are two FSH measurement of >30 U/l four weeks apart.
-
(D) Advise that she can keep the IUS for up to 7 years so long as she takes concomitant oestrogen-only HRT.
-
(E) Assure her that she is no longer at risk of pregnancy, remove the IUS and switch to continuous combined HRT.
-
(F) Insert a new Mirena IUS and commence sequential oestrogen-only HRT.
Question 5
Question
MENOPAUSAL MANAGEMENT
You undertake a telephone consultation with a 49 y.o. woman in your surgery who has been shielding from COVID-19 indoors in her apartment for the past 4 months. She is worried that her cervical screening appointment has been canceled. She also reports that she has been having vaginal dryness with itching, tiredness, hot flushes and night sweats which have now become unbearable in spite of having lighter sleep wear. Her last period was 7 months ago. Her past medical history is significant for polymyalgia rheumatica for which she takes 10 mg prednisolone for the past 6 months and depression for which she has been taking 40 mg fluoxetine for the past 2 years. Which of the following recommendations should you make?
{kind=link}
Answer
-
(A) Reassure her that she will receive an invitation as soon as normal screening programmes have recommenced and that she would also get the next appointment after the usual 3 years.
-
(B) Advise about cancer screening mammography in 1 year.
-
(C) Offer vaginal oestrogen in addition to vaginal lubricant.
-
(D) Request dual-energy X-ray absorptiometry (DXA) scan to measure bone mineral density (BMD) without calculating fragility fracture risk.
-
(E) Prescribe vitamin D supplementation if 25-hydroxyvitamin D serum levels are 25 to 50 nmol/l.
-
(F) Consider changing fluoxetine to venlafaxine.
Question 6
Question
RECURRENT MENOPAUSAL SYMPTOMS
A 55 year-old female office secretary, who is new to your surgery, stopped her sequential combined hormonal replacement therapy (HRT) 4 months ago which she had been having since the age of 48 years. She now requests recommencement of HRT for a recurrence of daily hot flushes and agitation affecting her work. She has become embarrassed with excessive sweating in spite of increased antiperspirant use. Apart from a couple spots of blood on her underwear last week, she has stopped having monthly bleeds since stopping HRT. Her cervical screening 2 months ago tested negative for HPV. She has an active history of smoking 20 cigarettes a day for the past 30 years but has found herself smoking even more because of her anxiety. Urinalysis was normal. What is the single most important management plan?
{kind=link}
Answer
-
Restart sequential combined HRT.
-
Offer transdermal HRT.
-
Commence a trial of Varenicline.
-
Seek urgent gynaecological specialist assessment.
-
Commence HRT as a continuous combined preparation.
Question 7
Question
VULVAL ITCHING
What is the treatment of choice for this 56 year-old post-menopausal woman who is complaining of increased vulval burning and itching and dyspaerunia? She denies any bleeding or vaginal discharge. Her last period was over 4 years ago.
Image:
Ls (binary/octet-stream)
{kind=link}
Answer
-
2% Clotrimazole cream topically three times daily for two weeks.
-
1% topical hydrocortisone ointment twice daily for four weeks.
-
Transdermal oestradiol patches for 6 months.
-
3-month regimen of topical 0.05% Clobetasol propionate.
-
A two week course of nightly topical Ovestin 0.1%.
Want to create your own Quizzes for free with GoConqr? Learn more.