3873073
Question 1
Question
The progressive loss of dopamine neurons between the substantia nigra and striatum is associated with which type of dementia?
Answer
-
Parkinson's
-
Alzhiemer's
-
Vascular Dementia
-
Mild Cognitive Impairment
Question 2
Question
The loss of dopamine neurons in the Basal Ganglia disease affects which subcortical circuit?
Answer
-
Direct motor pathway
-
Indirect motor pathway
-
Both Indirect and Direct motor pathways are affected
Question 3
Question
Which of the following are symptoms of Parkinson's Disease?
Answer
-
Difficulty distinguishing between smells, or loss of sense of smell.
-
Mood changes such as Apathy, Depression and Anxiety.
-
Autonomic dysfunction causing constipation
-
Sleep disturbances
-
Rigidity, Resting Tremor and Bradykinesia
-
Dyskinesia
-
Seizures
-
Smooth movement
-
Feeling unstable, postural difficulities
Question 4
Question
Depression occurs in approximately [blank_start]50%[blank_end] of Parkinson's patients.
Answer
-
50%
-
10%
-
80%
Question 5
Question
Which statement best describes the genetic component of Parkinson's
Answer
-
Parkinson's is a highly heritable disease, the presence of certain genes is predominant predictor.
-
Parkinson's is a highly heritable disease, in which several dominant type genes predict the development of parkinson's
-
Parkinson's is a highly heritable disease, in which several ressesive type genes predict the development of parkinson's
-
Genetics explain about 15% of the incidence of Parkinson's. There are 2 rare dominant gene mutations and several recessive mutations.
Question 6
Question
Definite diagnosis of Parkinson's is possible post mortem, if depigmentation is observed in the substantia nigra.
Answer
- True
- False
Question 7
Question
Autonomic dysfunction, depression, memory complaints, and Bradykinesia that develops gradually over time, rather than within a year is suggestive of:
Answer
-
Parkinson's Disease
-
Lewy Body Dementia
-
Alzhiemer's
Question 8
Question
The one year rule regarding Lewy Bodies Dementia and Parkinson's:
Answer
-
If motor and cognitive disturbances that develop in less than one year is likely to be Lewy Body Dementia rather than Parkinson's.
-
If motor and cognitive disturbances that develop gradually over more than one year is more likely to be Lewy Body Dementia rather than Parkinson's.
Question 9
Question
Frontal subcortical circuits are effector mechanisms that allow the organism to act on the environment. Impaired executive functions, apathy, and impulsivity are hallmarks of frontal subcortical circuit dysfunction. The [blank_start]dorsolateral prefrontal[blank_end] circuit allows the organization of information to facilitate a response; the [blank_start]anterior cingulate[blank_end] circuit is required for motivated behavior; and the [blank_start]orbitofrontal[blank_end] circuit allows the integration of limbic and emotional information into behavioral responses.
Answer
-
dorsolateral prefrontal
-
anterior cingulate
-
orbitofrontal
-
anterior cingulate
-
dorsolateral prefrontal
-
orbitofrontal
-
orbitofrontal
-
anterior cingulate
-
dorsolateral prefrontal
Question 10
Question
[blank_start]Parkinson's[blank_end] is the world's 2nd most common neurodegenerative disease
Answer
-
Parkinson's
-
Alzheimer's
-
Huntington's
Question 11
Question
Bradykinesia refers to:
Answer
-
Slowed movement
-
Rigitity
-
Tremor
-
Stooped posture
Question 12
Question
The gait associated with [blank_start]Parkinson's[blank_end] is characterized by a forward stooped posture, diminished or absent arm swing and slow shuffling steps, with difficulty starting to walk and once walking, difficulty stopping.
Answer
-
Parkinson's
Question 13
Question
Which of the following describes the speech and writing characteristic of Parkinson's disease
Answer
-
Writing acquires a cramped, micrographic and jerky appearance. Speech is commonly dysarthric; monotonal, low volume and variable speech speeds such that words may rush out one moment, then be halting and slow the next.
-
Writing acquires a cramped, micrographic and jerky appearance. Speech is commonly aphasic; nonsense babbling with fluent production and normal prosody
-
Writing is usually unaffected. Speech is commonly dysarthric; monotonal, low volume and variable speech speeds such that words may rush out one moment, then be halting and slow the next.
Question 14
Question
Parkinsonism refers to a
Answer
-
Disease
-
Syndrome
-
Early onset phase of Parkinson's Disease
Question 15
Question
Which of the following best describes the Risk factors associated with Parkinson's disease?
Answer
-
Repeated TBI Men > Women People regularly exposed to pesticides (Farmers and Agricultural Worker) Regular Inhalation of Heavy Metals Smokers < Non-Smokers Coffee Drinkers < Non-Coffee drinkers
-
Repeated TBI Men < Women People regularly exposed to pesticides (Farmers and Agricultural Worker) Regular Inhalation of Heavy Metals Smokers > Non-Smokers Coffee Drinkers < Non-Coffee drinkers
-
Single TBI Men > Women People regularly exposed to pesticides (Farmers and Agricultural Worker) Fans of Heavy Metal music Smokers > Non-Smokers Coffee Drinkers > Non-Coffee drinkers
-
Repeated TBI Men > Women People regularly exposed to pesticides (Farmers and Agricultural Worker) Regular Inhalation of Heavy Metals Smokers > Non-Smokers Coffee Drinkers > Non-Coffee drinkers
Question 16
Question
Parkinson's involves which of the following?
Answer
-
Dopminergic system
-
Noradrenergic system
-
Serotonergic system
-
Cholinergic system
Question 17
Question
Parkinson's Disease may begin two or more decades before the first symptoms develop.
Answer
- True
- False
Question 18
Question
Progression of [blank_start]Parkinson's disease[blank_end] tends to be slow with most patients surviving ten to 15 years after first symptoms are noticed.
Answer
-
Parkinson's disease
-
Delirium
-
Lewy Bodies Dementia
-
Creutzfeld Jacob’s disease
Question 19
Question
The majority of Parkinson's patients survive beyond 75 years
Answer
- True
- False
Question 20
Question
Earlier disease onset, tremor dominant, non-tremor dominant and rapid disease progression with dementia ar sub groups of
Answer
-
Alzheimer's
-
Vascular Dementia
-
Creutzfeld Jacob’s Disease
-
Parkinson's
Question 21
Question
Select the appropriate incidence of each of the following Parkinson's subtypes:
Earlier disease onset [blank_start]25%[blank_end]
Tremor dominant [blank_start]31%[blank_end]
Non-tremor dominant [blank_start]35%[blank_end]
Rapid disease progression with dementia [blank_start]8%[blank_end]
Answer
-
25%
-
31%
-
35%
-
8%
-
31%
-
25%
-
8%
-
70%
-
35%
-
25%
-
8%
-
70%
-
8%
-
60%
-
25%
-
31%
Question 22
Question
Which subtype of Parkinson's disease has the slowest progression in terms of cognitive decline?
Answer
-
Earlier disease onset
-
Tremor dominant
-
Non-tremor dominant
-
Rapid disease progression with dementia
Question 23
Question
When using the Unified Parkinson's Disease Rating Scale (UPDRS) a higher scores represents
Answer
-
a higher level of functional disability
-
a higher level of functional independence
Question 24
Question
Diagnosis of Parkinson's disease is confirmed as INCORRECT in one fourth of autopsied cases.
Answer
- True
- False
Question 25
Question
Which of the following disorders closely resemble Parkinson's Disease?
Answer
-
Progressive supranuclear palsy
-
Corticobasal degeneration
-
Vascular Parkinsonism
Question 26
Question
Which of the following represent the early signs of Parkinson's Disease
Answer
-
Tremor, Rigidity, Bradykinesia, Posture
-
Complete loss, or less sensitive sense of smell. Numbness and Coldness.
-
Cognitive Decline, Posture, Loss of Balance
-
Loss of Balance alone
Question 27
Question
The cognitive deficits typical of the early stages of Parkinson's are most similar to
Answer
-
those that occur with frontal lobe damage: difficulties switching or maintaining a set in the presence of feedback, initiating responses, goal directed behaviour.
-
those that occur with temporal lobe damage: difficulties with recognition, orientation and digit span, but spared implicit learning
-
those that occur with occipital lobe damage: difficulties switching or maintaining a set in the presence of feedback, initiating responses, goal directed behaviour.
-
those that occur with frontal lobe damage: difficulties with recognition but spared implicit learning
Question 28
Question
Vocabulary, grammar, and syntax tend to remain intact in PD
Answer
- True
- False
Question 29
Question
Diagnosis of depression in Parkinson's patients can be complicated by the presence of bradykinesia. Bradykinetic patients can lack facial expressiveness giving off the impression of depression, in addition to reduced motor activity and slowed responding. This is further compounded by the unreliability of self-reports in patients who are cognitively impaired.
Answer
- True
- False
Question 30
Question
Depression in Parkinson's Disease tends to respond well to conventional medication used to treat idiopathic depression.
Answer
- True
- False
Question 31
Question
Diagnosis of [blank_start]dementia with Lewy bodies[blank_end] is typically made when the diagnosis of dementia precedes or coincides within one year of the onset of motor symptoms. Whereas [blank_start]Parkinson's disease with dementia[blank_end] is usually made when dementia develops within the context of established [blank_start]PD[blank_end].
Answer
-
Parkinson's disease with dementia
-
dementia with Lewy bodies
-
PD
-
DLB
-
dementia with Lewy bodies
-
Parkinson's disease with dementia
Question 32
Question
Which of the following deficits tend to distinguish between Parkinson's with cognitive impairment and Parkinson's with dementia?
Answer
-
Executive dysfunction, particularly set shifting and concept formation.
-
Recognition Memeory
-
Impaired Verbal Fluency
-
Initiation
Question 33
Question
The positive effects of L - Dopa on movement
Answer
-
Tend to be stable, and can last many years.
-
Tend to begin to wear off after 2 - 4 years.
Question 34
Question
Parkinson's - Tango dance classes twice a week has been shown to improve balance, functional mobility and walking compared to a no dance group.
Answer
- True
- False
Question 35
Question
What am I?
Neurodegenerative disorder
Hereditary, Autosomal dominant
Typical Age at onset: 35-45 years
Duration: 15-20 years
Symptoms include: Bradykinesia and/or Chorea, Apathy, Executive Dysfunction, Working Memory Deficit, Psychiatric disorder, and elevated suicide rate
Answer
-
Huntington's Disease
-
Alzheimer's
-
Mild Cognitive Impairement
-
Parkinson's
-
Vascular Dementia
-
Major Depressive Disorder
-
Schizophrenia
Question 36
Question
All Huntington's patients develop dementia, unless they die before the disease has run it's course.
Answer
- True
- False
Question 37
Question
What number of trinucleotide CAG repeats (Cytosine, Adenine, Guanine) is considered pathological and linked to the development of Huntington's disease?
Answer
-
> 38
-
> 48
-
17 - 29
-
< 35
Question 38
Question
[blank_start]Huntington's disease[blank_end] results from an excessive number of trinucleotide [blank_start]CAG[blank_end] repeats ([blank_start]cytosine, adenine, guanine[blank_end]) in the [blank_start]HD gene[blank_end] that encodes a protein known as [blank_start]huntingtin[blank_end] located on chromosome [blank_start]4[blank_end]. People without the disease will have [blank_start]fewer than 35[blank_end] repeats. [blank_start]Huntington's Disease[blank_end] is considered autosomal [blank_start]dominant[blank_end], so that [blank_start]half[blank_end] of all offspring of a single carrier parent will develop the disease.
Answer
-
Huntington's disease
-
Alzheimer's disease
-
Parkinson's disease
-
Lewy bodies dementia
-
Major Depressive Disorder
-
Huntington's Disease
-
Alzheimer's Disease
-
Parkinson's Disease
-
Major depressive disorder
-
Lewy bodies dementia
-
CAG
-
GAG
-
TAG
-
cytosine, adenine, guanine
-
tycoon, adenine, guanine
-
guanine, adenine, guanine
-
HD gene
-
PD gene
-
AD gene
-
MD gene
-
huntingtin
-
tryptone
-
parkintin
-
globin
-
4
-
5
-
6
-
7
-
fewer than 35
-
more than 35
-
fewer than 15
-
more than 15
-
dominant
-
recessive
-
50%
-
35%
-
10%
Question 39
Question
Huntington's disease is more prominent in [blank_start]Caucasian[blank_end] populations than either [blank_start]Asian or African[blank_end] populations.
Answer
-
Caucasian
-
Asian
-
African
-
Asian or African
-
Caucasian or African
-
Asian or Caucasian
Question 40
Question
Huntington's disease - The most consistent change in neurotransmitters occurs as reduced levels of [blank_start]GABA[blank_end], with a consistent concomitant increase in [blank_start]excitatory[blank_end] neurotransmitters.
Answer
-
GABA
-
GATA
-
Glutamate
-
Norepinephrine
-
excitatory
-
inhibitory
Question 41
Question
There is a [blank_start]negative[blank_end] correlation between the number of CAG repeat length and age at onset for huntington's disease. Additionally, disease severity is [blank_start]positively[blank_end] correlated with CAG repeat lengths.
Answer
-
negative
-
positive
-
positively
-
negatively
Question 42
Question
In [blank_start]huntington's[blank_end] disease early onset is associated with more severe symptoms and faster degeneration. Conversely, early onset [blank_start]Parkinson's[blank_end] disease is associated with a slower progression.
Answer
-
Huntington's
-
Parkinson's
-
Parkinson's
-
Huntington's
Question 43
Question
Cognitive Impairment is often the first expression of the disease and may predate motor symptoms by as much as two year.
This statement is consistent with
Answer
-
Parkinson's disease
-
Huntington's disease
Question 44
Question
Huntington's Disease, Neuropsychological Profile:
Attention Span: [blank_start]Drops as disease progresses[blank_end]Set Shifting: [blank_start]Impaired[blank_end]
Working Memory: [blank_start]Impaired[blank_end]
Memory Deficit: [blank_start]Mild initially, worsen with time[blank_end]
Memory deficits tend to be due to [blank_start]retention strategy[blank_end]
Vocabulary and Grammar - [blank_start]Preserved early, develops last[blank_end]
Executive Function: [blank_start]Impaired[blank_end]
Answer
-
Drops as disease progresses
-
Preserved
-
Impaired
-
Preserved
-
Impaired
-
Preserved
-
retention strategy
-
primary retention deficit
-
Mild initially, worsen with time
-
Early development
-
Preserved early, develops last
-
Early sign
-
Impaired
-
Preserved
Question 45
Question
Emotional disturbances of personality change develop in [blank_start]almost all[blank_end] patients with Huntington's Disease.
Answer
-
almost all
-
10% of
-
30% of
-
50% of
Question 46
Question
Select ALL correct responses regarding depression in Huntington's Disease:
Answer
-
Depression often precedes motor and cognitive impairment
-
Depression is more common in Huntington's disease than Alzhiemers
-
Suicide rated for Huntington's patients are much higher than the general population. However, genetic testing that confirms HD does not appear to increase suicide risk.
-
Depression in Huntington's Disease is most likely a reaction to symptoms
Question 47
Question
Deep Brain Stimulation is more effective as a treatment of Huntington's Disease than Parkinson's
Answer
- True
- False
Question 48
Question
Which of the following is NOT classed as a subcortical dementia?
Answer
-
Parkinson's Disease
-
Huntington's Disease
-
Vascular Dementia
-
Alzheimer's Dementia
Question 49
Question
Multi Infarct Dementia (DIM), CADASIL (Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoaraiosis) and HCHWA-D (Hereditary cerebral hemorrhage with amyloidosis-Dutch type) are subtypes of which of the following?
Answer
-
Huntington's
-
Vascular Dementia
-
Hypertenion
-
Alzhiemer's
-
Fronto-Temporal Dementia
Question 50
Question
The umbrella term used in the DSM 5 to refer to what is commonly called dementia
Answer
-
Dementia
-
Major Dementia
-
Major Neurocognitive disorder
-
Major Neurodemented disorder
Question 51
Question
A lacunes or microinfarct is a damaged region of the brain < [blank_start]2mm[blank_end] in area, and typically involve central white matter tracts and [blank_start]subcortical[blank_end] regions.
Answer
-
2mm
-
10mm
-
0.5mm
-
subcortical
-
cortical
Question 52
Question
Strategic infarct dementia is
Answer
-
dementia resulting from a single lesion in a critical brain region
-
dementia brought on by surgical lesions to the subthalamic nucleus
-
A type of alzheimer's disease
-
Not a true dementia
Question 53
Question
A slowly progressive form of Vascular dementia that involves subcortical white matter lesions produced by chronic ischemia.
Answer
-
Alzheimer's Disease
-
CADASIL
-
Binswanger's disease
-
Lacunar/Multi infarct dementia
Question 54
Question
Huntington's Disease, Parkinson's Disease and Vascular Dementia all involve which of the following symptoms? Choose characteristic symptoms!
Answer
-
Executive Dysfunction
-
Depression
-
Psychomotor difficulties
-
Intial Primary Memory Loss
-
Arteriosclerosis
-
Lacunes
Question 55
Question
Intact disease insight tends to be present in Vascular Dementia
Answer
- True
- False
Question 56
Question
Name this disease.
Non-familial (i.e non-genetic)
Prevalence of 1.4 per 100,000
No known disease specific biomarker
Patients often display a inability to look downwards
Primary lesion sites begin in the upper brainstem and extend to the basal ganglia. In particular, this process appears to disconnect ascending pathways from these subcortical structures to the prefrontal cortex.
Dopamine levels drop drastically in the striatum
Alzheimer's often co-occurs (69% of cases)
Answer
-
Parkinson's
-
Lewy Bodies Dementia
-
Progressive supranuclear palsy
-
Huntington's disease
Question 57
Question
Which disease displays the following symptoms:
Onset after the age of 40
Early Symptoms:
Postural Instability
Dysarthria
Bradykinesia
Within the first year:
Cognitive or behavioural changes begin to develop. Rarely develop first
Can include: deficits typical of frontal lesions: apathy, initiation difficulties, flexibility.
Memory ability may be normal but significantly slowed. Memory impairment can occur, though not to the same extent as AD
Forward digit span may be within normal limits
Language will often remain intact, but primary progressive aphasia can occur. Also note Dysarthria.
Later:
Vertical gaze palsy, when patients try to bend their head to compensate their eyes roll up reflexively.
Others:
Oculomotor defects
Death often results from respiratory arrest, either secondary to pneumonia or due to degenerative processes involving brainstem respiratory centres.
Answer
-
Parkinson's
-
Lewy Bodies dementia
-
Progressive supranuclear palsy
-
Creutzfeldt Jacobs disease
Question 58
Question
Name this disease:
Primary symptomatic features include:
Progressive gait disturbance
Urinary Incontinence
Confusion, disorientation and memory problems.
Memory problems usually develop after Urinary incontinence and gait disturbance. Though Executive dysfunction can present relatively early in the disease. Perseveration,
Typical imaging shows enlargement of the ventricle due to excess CSF and white matter damage.
Answer
-
Normal Pressure Hydrocephalus
-
Alzheimer's Disease
-
Parkinson's Disease
-
Creutzfeldt Jacob's disease
Question 59
Question
Which of the following diseases/disorders can often be successfully treated with a "shunt"
Answer
-
Normal Pressure Hydrocephalus
-
Alzheimer's disease
-
Parkinson's
-
Lewy Bodies dementia
Question 60
Question
Normal Pressure Hydrocephalus has an incidence of approximately [blank_start]5.5[blank_end] in 100,000. Progressive supranuclear palsy has an incidence of approximately [blank_start]1.4[blank_end] in 100,000.
Answer
-
5.5
-
10.5
-
20.5
-
205
-
1.4
-
5.5
-
150
-
500
Question 61
Question
Name this disease:
Progressive dementia with rapid onset
Death usually occurs after 4-5 months
Atypical EEG
Myoclonus, gait disturbance, possible seizures
Psychiatric disturbance
Hallucinations
Answer
-
Creutzfeld Jakob’s Disease
-
Normal Pressure Hydrocephalus
-
Progressive supranuclear palsy
-
Early Onset Parkinson's
Question 62
Question
To receive a diagnosis of MCI the memory problems have to interfere with daily functioning
Answer
- True
- False
Question 63
Question
Histopathological hallmark of Alzheimer’s disease
Answer
-
Pick Bodies
-
Lewy bodies
-
Amyloid plaques
-
Ubiquitin inclusions
Question 64
Question
Sudden onset, fluctuating cognition and attention
Answer
-
Vascular dementia
-
Lewy body dementia
-
Delirium
-
Dementia
Question 65
Question
Visual hallucinations, most often
Answer
-
Fronto temporal dementia
-
Lewy body dementia
-
Alzheimer’s dementia
-
Semantic dementia
Question 66
Question
When does normal biological decay begin?
Answer
-
25 - 30 years
-
40 - 45 years
-
50 - 55 years
-
> 65 years
Question 67
Question
What proportion of the following populations have dementia?
Of 80+ population: [blank_start]20%[blank_end] dementia
Of 85+ population: [blank_start]40%[blank_end] dementia
Answer
-
20%
-
40%
-
60%
-
40%
-
20%
-
60%
Question 68
Question
A patient who presents with dysfunction on memory tasks (or any other domain), despite some difficulties day to day they are still able to function independently at home. What would be the most appropriate diagnosis?
Answer
-
MCI
-
CADASIL
-
Alzheimer's
-
Normal Pressure Hydrocephalus
Question 69
Question
Deficits in Mild Cognitive Impairment can only occurs within the cognitive domain of memory
Answer
- True
- False
Question 70
Question
All patients who develop true Mild Cognitive Impairment will progress to dementia
Answer
- True
- False
Question 71
Question
Non-amnestic MCI though to be predictive of:
Answer
-
Alzheimer's disease
-
Forms of dementia other than Alzheimer's (e.g Lewy Bodies Dementia, FTD)
Question 72
Question
Approximately [blank_start]5.6 - 15%[blank_end] of MCI patients convert to Dementia each year. However in many cases MCI will not develop any further, and in some cases it is even alleviated after time.
Answer
-
5.6 - 15%
-
30 - 35%
-
50%
Question 73
Question
Walking 72 blocks a week was associated with greater grey matter volume and a two fold reduced risk developing a cognitive impairment more than a decade later in a longitudinal study.
Answer
- True
- False
Question 74
Question
[blank_start]Amnestic MCI[blank_end] - Poor memory performance, below expected for the patient's age with no other cognitive deficits and not serious enough to warrant a diagnosis of dementia.
[blank_start]Nonamnestic MCI[blank_end] - Poor performance in any domain other than memory, below expected for the patient's age with no other cognitive deficits and not serious enough to warrant a diagnosis of dementia.
[blank_start]Multi domain MCI[blank_end] - Poor performance in at least two domains, below expected for the patient's age with no other cognitive deficits and not serious enough to warrant a diagnosis of dementia.
Answer
-
Amnestic MCI
-
Nonamnestic MCI
-
Multi domain MCI
Question 75
Question
Dementia applies to a condition in which both cognitive decline AND [blank_start]functional impairment[blank_end] are observed.
Answer
-
functional impairment
-
vascular impairment
-
atrophy of the hippocampus
-
dysexecutive syndrome
Question 76
Question
Alzheimer's Disease accounts for [blank_start]60 - 80%[blank_end] of dementia, with an estimated incidence of [blank_start]8.45 million[blank_end] affected in europe alone with an annual cost of [blank_start]141 billion[blank_end] Euro per year
Answer
-
60 - 80%
-
10 - 20%
-
45%
-
8.45 million
-
4.45 million
-
10.45 million
-
50 million
-
141 billion
-
20 billion
-
300 billion
Question 77
Question
A definite diagnosis of Alzheimer's is only possible after post-mortem exam in which amyloid plaques and neurofibrillary tangles are confirmed present.
Answer
- True
- False
Question 78
Question
Whether [blank_start]Alzheimer's[blank_end] disease evolves from neurofibrillary tangles and amyloid plaques or whether they are a by product of the disease [blank_start]in unknown.[blank_end]
Answer
-
Alzheimer's
-
Stroke
-
Normal Pressure Hydrocephalus
-
is unknown.
-
is certain.
-
depends of the type of dementia
Question 79
Question
[blank_start]Probable Alzheimer's disease:[blank_end] Dementia has been established by clinical and neuropsychological examination. Cognitive impairments also have to be progressive (ie decline from previous functioning) and be present in two or more areas of cognition. Deficit interferes with ability to work/daily functioning. Onset between the ages of 40 and 90 years and finally there must be an absence of other diseases capable of producing a dementia syndrome.
[blank_start]Definite Alzheimer's disease:[blank_end] The patient meets the criteria for probable Alzheimer's disease and has histopathologic evidence of AD via autopsy or biopsy.
[blank_start]Unlikely Alzheimer's disease:[blank_end] The patient presents a dementia syndrome with a sudden onset, focal neurologic signs, or seizures or gait disturbance early in the course of the illness
[blank_start]Possible Alzheimer's disease[blank_end]: There is a dementia syndrome with an atypical onset, presentation or progression; and without a known etiology; but no co-morbid diseases capable of producing dementia are believed to be in the origin of it. Or a lack of sufficient patient history or objective cognitive documentation.
Answer
-
Probable Alzheimer's disease
-
Definite Alzheimer's disease
-
Unlikely Alzheimer's disease
-
Possible Alzheimer's disease
-
Definite Alzheimer's disease:
-
Probable Alzheimer's disease
-
Possible Alzheimer's disease
-
Unlikely Alzheimer's disease
-
Unlikely Alzheimer's disease:
-
Definite Alzheimer's disease
-
Probable Alzheimer's disease
-
Possible Alzheimer's disease
-
Possible Alzheimer's disease
-
Probable Alzheimer's disease
-
Definite Alzheimer's disease
-
Unlikely Alzheimer's disease
Question 80
Question
According to the DSM-IV a diagnosis of probable Alzheimer's must include a decline in at least two cognitive domains. One of these deficits MUST involve an inability to learn new information or recall previously learned information. The decline must also be sufficient enough to impair social or occupational functioning.
Answer
- True
- False
Question 81
Question
[blank_start]30%[blank_end] of all dementia cases are due to Alzheimer's ALONE, [blank_start]38%[blank_end] are AD with infarcts
Answer
-
30%
-
60 - 80%
-
10 - 20%
-
38%
-
20%
-
50%
-
12%
Question 82
Question
A common explanation to account for the fact that people with higher levels of education have a lower risk of developing AD is that these people have a higher [blank_start]cognitive reserve[blank_end] to compensate for the negative effects of the disease.
Answer
-
cognitive reserve
Question 83
Question
Higher rates of educational attainment is associated with [blank_start]faster[blank_end] rates of cognitive decline after a diagnosis of dementia but [blank_start]a delayed[blank_end] onset.
Answer
-
faster
-
slower
-
the same
-
a delayed
-
an early
Question 84
Question
Alzheimer's likely does not have a genetic component.
Answer
- True
- False
Question 85
Question
Roughly [blank_start]25%[blank_end] of Alzheimer's disease is familial, this is especially the case for [blank_start]early[blank_end] onset AD in which [blank_start]60%[blank_end] of cases are familial.
Answer
-
early
-
late
-
25%
-
60%
-
80%
-
60%
-
25%
-
80%
Question 86
Question
What percentage of Alzheimer's Begins before the age of 60 - 65? I.e What proportion of AD is "early onset"
Answer
-
1 - 6%
-
20%
-
10%
-
10 - 20%
Question 87
Question
Mutations of the presenilin-1 gene on chromosome 14, presenilin-2 gene on chromosome 1 and Amyloid precursor protein gene on chromosome 21 are associated with which form of dementia?
Answer
-
Early Onset Alzhiemer's
-
Early Onset Parkinson's
-
Early Onset Huntington's
Question 88
Question
Vascular risk factors such as high fat consumption, arteriosclerosis, hypertension and diabetes are risk factors for:
A. Alzheimer's Disease
B. Vascular Dementia
Answer
-
A
-
B
-
Both A and B
-
Neither
Question 89
Question
TBI increases the risk factor of which of the following diseases?
A. Alzheimer's
B. Parkinson's
Answer
-
A
-
B
-
A and B
-
Neither A nor B.
Question 90
Question
Hormone Replacement Therapy (combined estrogen and progesterone) may as much as double the risk of developing Alzheimer's Dementia.
Answer
- True
- False
Question 91
Question
Daily light to moderate alcohol consumption (1-2 drinks per day) is associated with a lower risk of dementia.
Answer
- True
- False
Question 92
Question
[blank_start]Neurofibrillary tangles[blank_end] develop when the microtubules that transport substances from the nerve cell body to the end of the axon become twisted. The protein that helps to maintain these structures is known as [blank_start]tau[blank_end]. In [blank_start]Alzheimer's disease[blank_end], this protein is altered allowing the twisted tubules to aggregate into [blank_start]tangles[blank_end].
Answer
-
Neurofibrillary tangles
-
Amyloid Plaques
-
Lewy Bodies
-
tau
-
amyloid
-
Lewy protein
-
Alzheimer's disease
-
Lewy Bodies Dementia
-
Huntington's Disease
-
tangles
-
plaques
Question 93
Question
In AD which of the following cortical regions are comparatively spared, even in later stages?
Answer
-
primary motor and sensory areas
-
primary visual areas
-
temporal lobe, especially the medial temporal lobe including the hippocampus and the entorhinal cortex.
-
prefrontal areas
Question 94
Question
Second to memory decline, which of the following presents the most sensitive measure when diagnosing AD
Answer
-
Hippocampal volume on MRI
-
Language Disorder
-
Blood Test
-
Motor coordination/Gait
Question 95
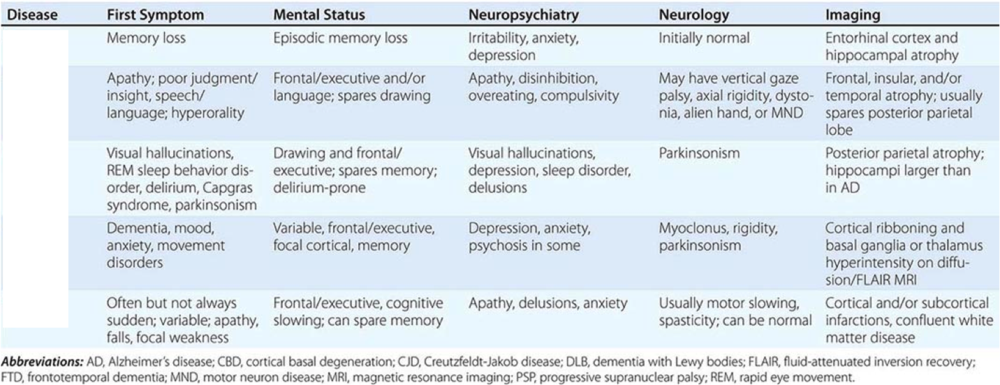{kind=link}
Answer
-
AD
-
FTD
-
DLB
-
CJD
-
Vascular
-
FTD
-
AD
-
CJD
-
DLB
-
Vascular
-
DLB
-
AD
-
FTD
-
CJD
-
Vascular
-
CJD
-
Vascular
-
AD
-
FTD
-
DLB
-
Vascular
-
DLB
-
AD
-
CJD
-
FTD
Question 96
Question
In alzheimer's, [blank_start]older[blank_end] memories tend to be better preserved than [blank_start]new[blank_end] memories.
Answer
-
older
-
newer
-
new
-
old
Question 97
Question
Central to language deterioration in Alzheimer's patients is a disintegration of [blank_start]semantic relationships and understanding[blank_end].
Answer
-
semantic content of words and sentences
-
syntax and linguistic organisation
-
word pronounciation
Question 98
Question
Although popular as a screening measure for AD clock drawing deficits are not specific to AD, in fact they tend to occur more frequently in Parkinson's Disease and Lewy Body Dementia.
Answer
- True
- False
Question 99
Question
The closing in phenomenon demonstrated by some dementia patients in visuoconstruction tasks is more closely associated with:
A: Alzheimer's Disease
B: Vascular Dementia
Answer
-
A
-
B
-
A and B
Question 100
Question
[blank_start]Perseveration[blank_end] is the uncontrolled repetition or continuation of a response (e.g., behavior, word, thought, activity, strategy, or emotion) in the absence of an ongoing occasion or rationale for that behavior or emotion (e.g., the topic or task requirements have changed). Whereas, an [blank_start]intrusion[blank_end] is defined as the inappropriate repetition of a prior response to a task after intervening stimuli, that is on a later task.
Answer
-
intrusion
-
Perseveration
Question 101
Question
Alzheimer's and EEG: slowing
[blank_start]Increased[blank_end] theta activity, combined with
[blank_start]Decreased[blank_end] alpha activity, and
[blank_start]Decreased[blank_end] beta activity
Late stages: [blank_start]Increased[blank_end] delta activity
Answer
-
Increased
-
Decreased
-
Decreased
-
Increased
-
Decreased
-
Increased
-
Increased
-
Decrease
Question 102
Question
[blank_start]Frontotemporal lobar[blank_end] dementia typically involved pathology of the frontal and temporal lobes with relative sparing of the posterior regions. Age of onset is relatively young (40 - 65) and there are three main subtypes a [blank_start]behavioural[blank_end] variant, a [blank_start]semantic[blank_end] type and [blank_start]primary progressive aphasia[blank_end].
Answer
-
Frontotemporal lobar
-
behavioural
-
semantic
-
primary progressive aphasia
Question 103
Question
Pick's Disease is the former name of which type of dementia/major neurocognitive disorder?
Answer
-
Lewy Bodies Dementia
-
Alzhiemer's
-
Frontotemporal lobar dementia FTLD
-
Progressive supranuclear palsy
Question 104
Question
Which of the following are considered risk factors for FTLD
Answer
-
Being Female
-
Old Age
-
Low Educational achievement
-
Several genetic factors, 40 - 50% of cases are transmitted by autosomal dominant inheritance
-
TBI may be a contributing factor
Question 105
Question
Pick's Bodies are found in about [blank_start]20%[blank_end] of patients with FTLD.
Answer
-
20%
-
90%
-
70%
-
0%
Question 106
Question
In pure/classic FTLD the parietal and occipital lobes remain intact.
Answer
- True
- False
Question 107
Question
Hippocampal atrophy in FTLD (Choose the BEST)
Answer
-
Is typically atrohpied
-
Is typically spared
-
Varies from case to case
Question 108
Question
Which of the following types of dementia best fits the following symptom set in its classic form:
extrapyramidal signs (shakiness, rigidity etc), apathy, relatively young onset (40 - 65), executive dysfunction, incontinence, and in particular profound social and behavioural change as an early stage symptom.
Answer
-
FTLD - Behavioural subtype
-
Normal Pressure Hydrocephalus
-
Parkinson's disease dementia
-
Alezhiemer's
Question 109
Question
In a classic distinction Alzheimer's patients will present with [blank_start]memory[blank_end] problems as the primary symptom, whereas patients with FTLD will more often present with [blank_start]social and executive[blank_end] primary symptoms. However these distinctions should be taken lightly as co-occurrence and symptomatic overlap are common.
Answer
-
memory
-
dysexecutive
-
incontinence
-
social and executive
-
memory related
-
sensory related
Question 110
Question
Dementia patients who have more temporal than frontal involvement, little to no posterior involvement, intact autobiographical memory but impaired knowledge of word meaning. This constellation of symptoms best matches
Answer
-
FTLD - Semantic dementia
-
FTLD - Behavioural variant
-
Alzheimer's
-
Normal Pressure Hydrocephalus
Question 111
Question
Semantic dementia (FTLD) - usually grammar and syntax remains intact. Prominent anterior temporal lobes atrophy is associated.
Answer
- True
- False
Question 112
Question
[blank_start]Primary progressive aphasia[blank_end] occurs without memory impairment or dementia in the early course. Many patients remain dementia free for at least 2 years and as many as 10. The disorder starts with anomia and proceeds to grammatical structure and language comprehension
Answer
-
Primary progressive aphasia
Question 113
Question
[blank_start]Primary progressive aphasia[blank_end] starts with anomia and proceeds to grammatical structure and language comprehension. [blank_start]FTLD - Semantic Dementia[blank_end] word meanings are usually lost with an intact sense of grammar.
Answer
-
FTLD - Semantic Dementia
-
Primary progressive aphasia
-
Primary progressive aphasia
-
FTLD - Semantic Dementia
Question 114
Question
Primary progressive aphasia - Usually associated with [blank_start]FTLD[blank_end] although [blank_start]AD[blank_end] accounts for 30% of all cases. [blank_start]Unlike[blank_end] other FTLD women are more often affected than men.
Answer
-
FTLD
-
AD
-
PDD
-
HD
-
AD
-
FTLD
-
PDD
-
HD
-
Unlike
-
Like
Question 115
Question
1st Step: Neurodegenerative disease: Shows [blank_start]progressive deterioration[blank_end] of behaviour and/or cognition by observation or history (as provided by a knowledgeable informant).
II. [blank_start]Possible[blank_end] bvFTLD
Three of the following behavioural/cognitive symptoms (A–F) must be present to meet criteria. Ascertainment requires that symptoms be persistent or recurrent, rather than single or rare events.
A. Early* behavioural disinhibition [one of the following symptoms (A.1–A.3) must be present]:
A.1. [blank_start]Socially inappropriate behaviour[blank_end]
A.2. [blank_start]Loss of manners or decorum[blank_end]
A.3. [blank_start]Impulsive, rash or careless actions[blank_end]
B. Early apathy or inertia [one of the following symptoms (B.1–B.2) must be present]:
B.1. Apathy
B.2. Inertia
C. Early loss of [blank_start]sympathy or empathy[blank_end] [one of the following symptoms (C.1–C.2) must be present]:
C.1. Diminished response to other people’s needs and feelings
C.2. Diminished social interest, interrelatedness or personal warmth
D. Early [blank_start]perseverative[blank_end], stereotyped or compulsive/ritualistic behaviour [one of the following symptoms (D.1–D.3) must be present]:
D.1. Simple repetitive movements
D.2. Complex, compulsive or ritualistic behaviours
D.3. Stereotypy of speech
E. [blank_start]Hyperorality[blank_end] and dietary changes [one of the following symptoms (E.1–E.3) must be present]:
E.1. Altered food preferences
E.2. Binge eating, increased consumption of alcohol or cigarettes
E.3. Oral exploration or consumption of inedible objects
F. Neuropsychological profile: executive/generation deficits with relative sparing of [blank_start]memory and visuospatial functions[blank_end] [all of the following
symptoms (F.1–F.3) must be present]:
F.1. Deficits in executive tasks
F.2. [blank_start]Relative sparing of episodic memory[blank_end]
F.3. Relative sparing of visuospatial skills
III. Probable bvFTLD
All of the following symptoms (A–C) must be present to meet criteria.
A. Meets criteria for possible bvFTD
B. Exhibits significant functional decline (by caregiver report or as evidenced by Clinical Dementia Rating Scale or Functional Activities Questionnaire scores)
C. Imaging results consistent with bvFTD [one of the following (C.1–C.2) must be present]:
C.1. [blank_start]Frontal and/or anterior temporal atrophy[blank_end] on MRI or CT
C.2. [blank_start]Frontal and/or anterior temporal[blank_end] hypoperfusion or hypometabolism on PET or SPECT
IV. Behavioural variant FTD with definite FTLD Pathology
Criterion A and either criterion B or C must be present to meet criteria.
A. Meets criteria for possible or probable bvFTD
B. Histopathological [blank_start]evidence of on biopsy or at post-mortem[blank_end]
C. Presence of a known pathogenic mutation
V. [blank_start]Exclusionary criteria[blank_end] for bvFTLD
Criteria A and B must be answered negatively for any bvFTLD diagnosis. Criterion C can be positive for possible bvFTLD but must be negative for probable bvFTLD
A. Pattern of deficits is better accounted for by other non-degenerative nervous system or medical disorders
B. Behavioural disturbance is better accounted for by a psychiatric diagnosis
C. Biomarkers strongly indicative of Alzheimer’s disease or other neurodegenerative process
Answer
-
Exclusionary criteria
-
evidence of on biopsy or at post-mortem
-
Frontal and/or anterior temporal atrophy
-
Frontal and/or anterior temporal
-
Socially inappropriate behaviour
-
Loss of manners or decorum
-
Impulsive, rash or careless actions
-
Hyperorality
-
progressive deterioration
-
memory and visuospatial functions
-
Relative sparing of episodic memory
-
perseverative
-
sympathy or empathy
-
Possible
Question 116
Question
Difficulty in language as most prominent clinical feature
Principal cause of impaired ADL
Aphasia most prominent deficit at onset and initial phase
Sounds like?
Answer
-
Primary Progressive Aphasia
-
Alzheimer's
-
Lewy Bodies
Question 117
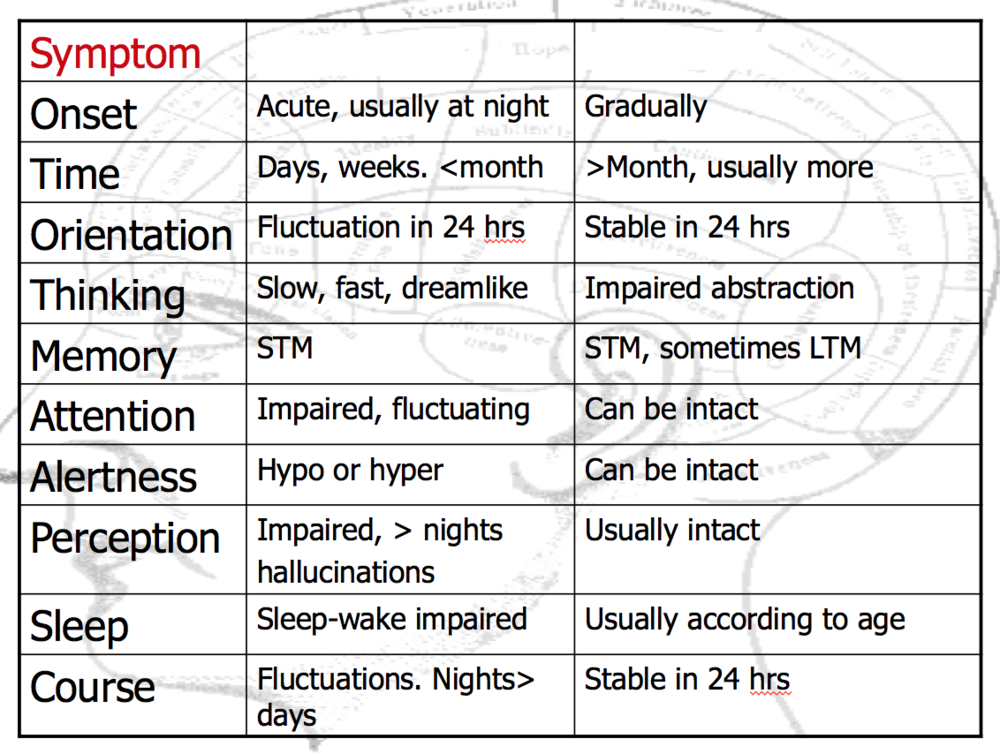
{kind=link}
Answer
-
Depression
-
Delirium
-
Dementia
-
Dementia
-
Delirium
-
Depression
Question 118
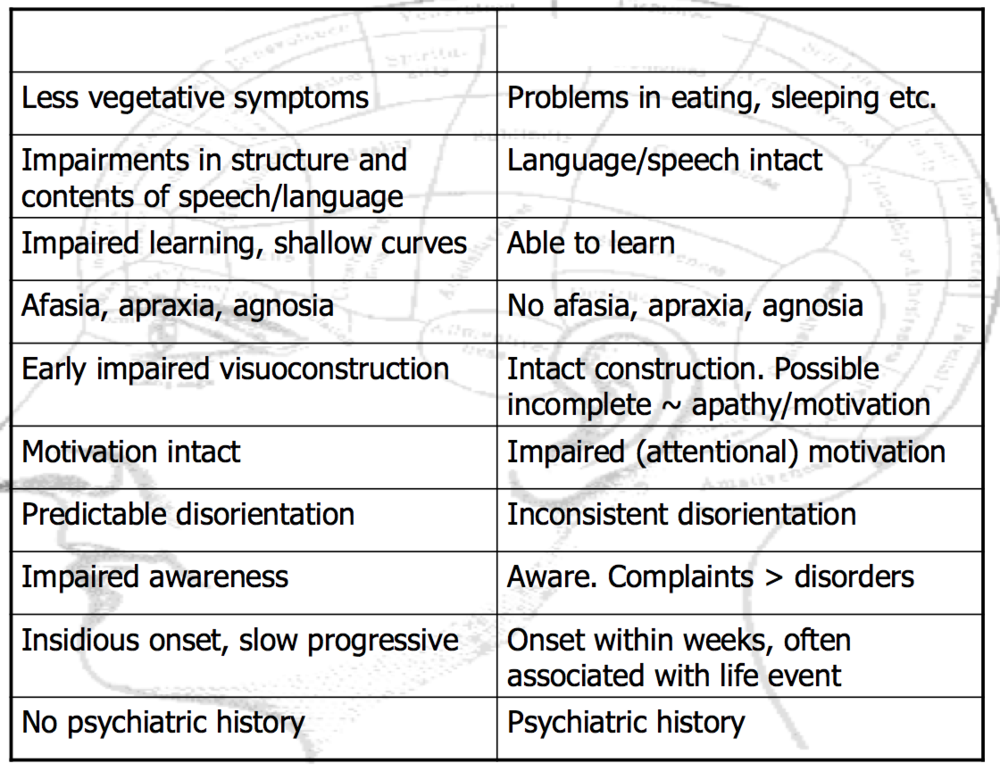
{kind=link}
Answer
-
Delirium
-
Depression
-
Dementia
-
Dementia
-
Depression
-
Delirium
Question 119
Question
What is the relationship between the following list and dementia?
Hypothyroidism, Neurology (tumor, hematoma's), Intoxications (medication, alcohol), Infections (Lues, HIV, Lyme), Deficiencies (vit. B12, B1), Psychiatric Health.
Answer
-
Possible confounding factors in diagnosis
-
Possible causal factors
Question 120
Question
Name the dementia:
Unrecognized until the 1970s
Major features include extrapyramidal signs (parkinsonisms), fluctuating cognition, visual hallucinations
Often deficits in attention, visuoperceptual and executive function.
Not neatly classified as primarily sub-cortical nor cortical
Answer
-
Alzheimer's
-
Dementia with Lewy Bodies
-
Parkinson's Disease
-
Progressive supranuclear palsy
Question 121
Question
Lewy bodies are found in:
Answer
-
Dementia with Lewy Bodies
-
Lewy Body variant of Alzheimer's (if neurofibrillary tangles are also present)
-
Parkinson's Disease
-
All of these are correct.
Question 122
Question
Amyloid Plaques are uncommon in Dementia with Lewy bodies, though neurofibrillary tangles are common.
Answer
- True
- False
Question 123
Question
Lewy bodies in largely concentrated in the substantia nigra alone are characteristic of:
Answer
-
Parkinson's Disease
-
Dementia with Lewy Bodies
-
Alzheimer's
Question 124
Question
Lewy bodies in the substantia nigra, limbic and cortical areas, without neruofibrillary tangles (tau) is suggestive of
Answer
-
Dementia with Lewy Bodies.
-
Alzheimer's
-
Parkinson's
Question 125
Question
Decline in [blank_start]DLB[blank_end] is usually more rapid than decline in [blank_start]AD[blank_end]
Answer
-
DLB
-
AD
-
AD
-
DLB
Question 126
Question
It is well known that some normally functioning elderly people at the time of death have abundant neuropathological signs of AD (etc) in post mortem exam
Answer
- True
- False
Question 127
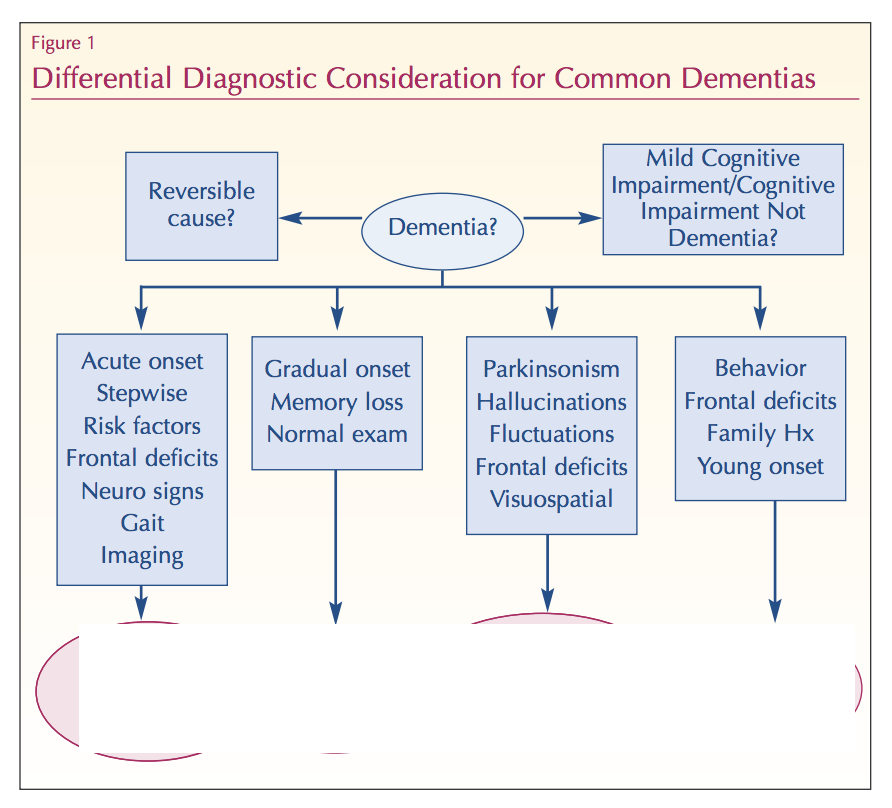{kind=link}
Answer
-
Vascular Dementia
-
AD
-
PD or DLB
-
FTLD
Question 128
Question
Label the functions associated with these frontal-subcortical circuits:
DLPFC - [blank_start]Executive Functioning[blank_end]
Anterior Cingulate - [blank_start]Motivation and Drive[blank_end]
Orbito Frontal/Lateral Orbital PFC - [blank_start]Inhibition, Social rules[blank_end]
Answer
-
Motivation and Drive
-
Executive Functioning
-
Inhibition, Social rules
-
Executive Functioning
-
Executive Functioning
-
Inhibition, Social rules
-
Inhibition, Social rules
-
Motivation and Drive
-
Motivation and Drive
Question 129
Question
Depression can result in biases in
A Attention
B Processing
C Memory
D All of the above
Answer
-
A
-
B
-
C
-
D
Want to create your own Quizzes for free with GoConqr? Learn more.