144983
Anatomy Learning Tool

Description
Module Information
{kind=link}
Description
No tags specified
Show more
Show less
EYE
The eye, a part of the sensory nervous system, is the organ responsible for humans' conscious sense of light and visibility. It has the ability to phototransduce, which is the conversion of photon energy into an integrated neural signal that passes through the optic nerve as an action potential to the visual cortex of the brain. The processing of the brain information there results in the senses of colour, luminance, contrast, and dimension (Nguyen and Duong, 2020).
ANATOMY OF THE EYE
The eye is a three-layered sphere of fluid-filled tissue. The outer layer is called fibrous tunic and is made up of the sclera, a hard, white, fibrous substance. The cornea, a specialised transparent tissue that allows light to enter the eye, replaces this opaque outer layer at the front of the eye. The iris, ciliary body, and choroid are three separate but connected structures that make up the middle layer of tissue. The coloured area of the eye that is visible through the cornea is called the iris. It has 2 pairs of muscles with opposit functions to one another, allowing the pupil's size to be changed under neurological control (Purves et al., 2001).
The inner layer of the eyeball is the retina and it consists grossly of two functional parts with distinct locations: the optic and nonvisual parts. The optic part of the retina is sensitive to visual light rays and has two layers: a neural layer and pigmented layer. The neural layer is light receptive. The pigmented layer consists of a single layer of cells that reinforces the light-absorbing property of the choroid in reducing the scattering of light in the eyeball (Clinically oriented anatomy book).
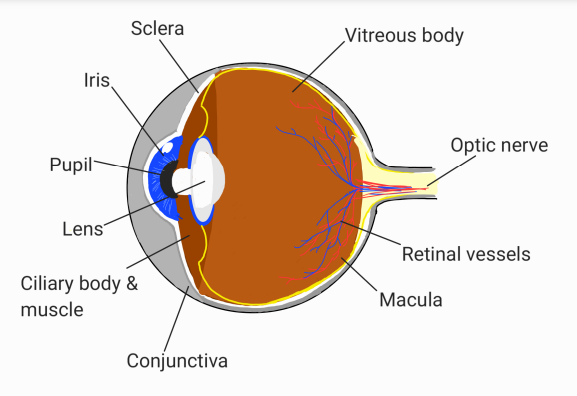
Structure of the eye
Six cranial nerves innervate the motor, sensory, and autonomic components in the eyes. The six cranial nerves are the facial nerve, abducens nerve, trigeminal nerve, trochlear nerve, optic nerve, and oculomotor nerve (CN II–CN VI and CN VII).
The optic nerve detects the incoming light and transfers the image seen on the retina to the cerebral brain (Smith and Czyz, 2022).
The superior, medial and inferior rectus, inferior oblique, levator palpebrae superioris, ciliary, and sphincter are among the extraocular muscles of the eyes that are innervated by the oculomotor nerve.
The superior oblique muscle causes the eye to torque inferiorly and inward, is motorily innervated by the trochlear nerve (Kim, Motlagh and Naqvi, 2022).
The ophthalmic branch (CN V1), maxillary branch (CN V2), and mandibular branch (CN V3) are the three divisions of the trigeminal nerve (CN V). However, the eye is innervated by the trigeminal nerve's ophthalmic branch (Huff and Daly, 2021).
The lateral rectus muscle, which permits abduction on the eye, is innervated by the abducens nerve (Nguyen, Reddy and Varacallo, 2020).
the facial nerve innervates the orbicularis oculi muscle, which is responsible for eye closure and blinking (Dulak and Naqvi, 2021).
• The lacrimal nerve, which arises in the lateral wall of the cavernous sinus and passes to the lacrimal gland, giving sensory branches to the conjunctiva and skin of the superior eyelid; its distal part also carries secretomotor fibers conveyed to it from the zygomatic nerve (CN V2).
• The frontal nerve, which enters the orbit through the superior orbital fissure and divides into the supra-orbital and supratrochlear nerves, providing sensory innervation to the superior eyelid, scalp, and forehead
• The nasociliary nerve, the sensory nerve to the eyeball, which also supplies several branches to the orbit, face, paranasal sinuses, nasal cavity, and anterior cranial fossa.
The infratrochlear nerve, a terminal branch of the nasociliary nerve, supplies the eyelids, conjunctiva, etc.
The ciliary muscle is a smooth muscle ring that controls accommodation by altering the shape of the lens, as well as controlling the flow of aqueous humor into Schlemm's canal. The ciliary muscle is attached to the zonular fibers, which suspend the lens. Upon contraction of the ciliary muscle, the tension on the lens becomes lessened, which causes it to adopt a more spherical shape to focus on near objects. Relaxation of the ciliary muscle has the opposite effect, optimizing distant focus (Ludwig et al., 2022).
TYPES OF GLAUCOMA:
Open-angle glaucoma (OAG): is a multifactorial, prolonged, progressive optic neuropathy that affects multiple factors and is distinguished by an open angle of the anterior chamber, typical modifications to the optic nerve, and progressive loss of peripheral vision followed by loss of the central visual field. Intraocular pressure (IOP) is a significant risk factor for this condition (Mahabadi, Foris and Tripathy, 2022). Nonetheless, open-angle glaucoma comprises the majority of cases in the United States and Western Europe.
Primary open-angle glaucoma (POAG): IOP-related injury to the optic nerve and the subsequent loss of retinal ganglion cells (RGCs) are suggested to be the causes of optic neuropathy. Commonly, POAG is identified during a normal eye checkup that includes fundoscopic assessment and visual field testing (using perimetry). Tonometry-measured increases in IOP are not required for diagnosis. Surgery to lower IOP and topical medication therapy are used to treat POAG, but new treatments that focus on RGC neuroprotection and axonal regeneration are now being developed (Weinreb et al., 2016).
Primary Congenital glaucoma (PCG): is a potentially blinding ocular condition that develops as a result of an abnormal anterior chamber angle during development and raises IOP. Trabecular dysgenesis, with or without different degrees of concomitant iridodysgenesis, such as halted posterior migration of the peripheral iris tissue and malformed trabecular angle meshwork, with or without dysgenesis of the Schlemm's canal (SC), is the underlying mechanism in PCG (Chen et al., 2014). The main surgical procedures used to treat PCG at the moment are goniotomy and trabeculotomy ab externo, which both aim to reduce the aberrant trabecular angle. As it directly treats the underlying outflow anomaly and restores a physiologic outflow of the aqueous humour from the anterior chamber to the SC, angle surgery is typically the main operation in PCG (Chen et al., 2014). Goniotomy is a surgery, which involves cutting the trabecular meshwork under direct gonioscopic visualisation to let the aqueous humour to flow into the SC and collection channels, has been demonstrated to be beneficial (Barkan, 1938). A safer operation with a lower incidence of infections and hypotony is trabeculotomy ab externo (Mori et al., 2020). Before a metal probe is placed into the Schlemm's canal and rotated into the anterior chamber to perforate the inner wall of the canal, the Schlemm's canal is first detected during the surgery by either pealing off a scleral flap or by making an incision in the scleral wall over the canal. (Mori et al., 2020).
GLAUCOMA: is a disease caused by an increase in pressure in the posterior chamber, within the eye as a result of blockage of the flow of aqueous humor, a watery fluid produced by the ciliary body.
There are two types of blockage:
1) The blockage may occur in the porous tissue between the anterior chamber and the canal of Schlemm or in the aqueous veins. This blockage is continuous, and the effect is chronic glaucoma. In persons in whom the angle at the periphery of the anterior chamber, the pressure of aqueous humor upon the back of the iris may force the outer part of the iris against the wall, so as to cover the outlet into the canal of Schlemm. Glaucoma caused by this type of obstruction is called acute or narrow-angle glaucoma. Narrow angle glaucoma causes pain in the eye, headaches and sometimes vomiting and nausea. Eventually, the affected person may see halos around lights
Treatments:
Therapy involves decreasing intraocular pressure using medications that constrict the pupil, such as miotic medications that promote increased aqueous fluid outflow. Surgery is needed to permanently reduce the high pressure, and a hole is made in the iris' outer periphery to let the aqueous humour to flow.
Risk factors for primary open angle glaucoma include older age, black race, Hispanic origin, family history and diabetes mellitus. (high risk among asian and alaskan populations, why?)
What is intraocular pressure?
Is the fluid pressure inside the eye. Is a measurement involving the magnitude of the force exerted by the aqueous humor on the internal surface of the anterior eye.
Normal Intraocular Pressure (IOP) = 10-21 mmHg. If it drops to 0 mmHg it is considered as hypotony, however, it can exceed the 70 mmHg and it leads to glaucomas.
Tonometry is the procedure eye care professionals perform to determine the IOP, the fluid pressure inside the eye.
What is the aqueous humor?
It is a transparent watery fluid with low protein concentrations. It is secreted from the ciliary body and it fills both the anterior and the posterior chambers of the eye. The anterior chamber of the eye is the space between the cornea anteriorly and the iris/pupil posteriorly. The posterior chamber of the eye is between the iris/ pupil anteriorly and the lens and ciliary body posteriorly.
The aqueous humor exits the anterior chamber via:
1) A small amount transmits through the iris and back into the posterior chamber.
2) A small amount passes into the subarachnoidal space and enters venous circulation in ciliary body, sclera, choroid.
3) The majority drains through the trabecular meshwork at the angle of the anterior chamber and into the canal of Schlemm, where it enters episcleral veins.
Women VS Men with Glaucoma:
i) Rotterdam study demonstrated increased risk of primary open angle glaucoma in women with early menopause.
ii) Women are at higher risk due to anatomical predispositon.
iii) Female sex hormones may influence IOP as well as vascular resistance that might effect the optic nerve head circulation. (Higher IOP after menopause).
iv) Hormone Replacement Therapy (HRT) (menopausal therapy, used to treat symptoms of menopause) leads to reduction of IOP after increase in both women with and without glaucoma.
v) Opposed to testosterone, estrogen enhances ocular blood flow.
vi) Female sex hormone may be protective against glaucoma (how?)
Description
No tags specified
Show more
The human eyeball consists of three main layers of the eye are: (1) the outermost supporting layer, which is composed of the clear cornea, the opaque sclera, and their zone of interdigitation, known as the limbus; (2) the middle uveal layer, which is composed of the iris, ciliary body, and choroid and constitutes the central vascular layer of the globe; and (3) the interior layer, which is commonly referred to as the retina.
Show less
Media
{kind=link}
Context
Description
No tags specified
Show more
Glaucoma is an irreversible, progressive optic neuropathies caused by high intraocular pressure, which can result in significant vision field loss and blindness. Older age, black race, Hispanic origin, family history of glaucoma, and diabetes mellitus are all risk factors for primary open-angle glaucoma.
Show less
Media
{kind=link}
Context
Description
No tags specified
Show more
The Schlemm's canal is a ring-shaped, endothelium-lined vessel that surrounds the cornea. It is located against the trabecular meshwork's juxtacanalicular area. Following filtering via the trabecular meshwork, one of its primary functions is to transfer aqueous humour into the collecting channels.
Show less
Media
{kind=link}
Context
Description
No tags specified
Show more
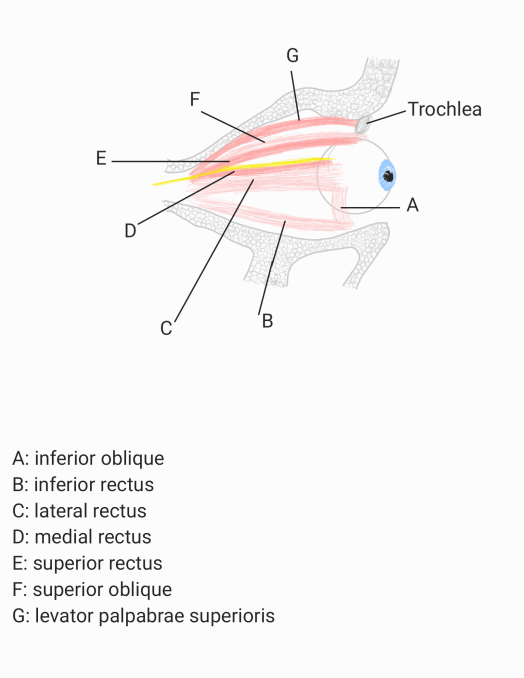
There are seven extraocular muscles. There are a total of four rectus muscles, two oblique muscles, and the standalone levator palpebrae superioris. The four rectus muscles are the medial rectus, lateral rectus, superior rectus, and inferior rectus. The oblique muscles are the superior and inferior obliques.
Levator palpabrae superioris acts to elevate the superior eyelid.
Superior oblique acts to abduct, depress and rotate the eyeball medially.
Inferior oblique acts to abduct, elevate and rotate the eyeball laterally.
Superior rectus acts elevate, adduct and rotate the eyeball medially.
Inferior rectus acts depress, adduct and rotate the eyeball laterally.
Medial rectus acts to adduct the eyeball.
Lateral rectus acts to abdoct the eyeball.
Show less
{kind=link}