1063240
Beschreibung
Mindmap von LewisLewis, aktualisiert more than 1 year ago
|
|
Erstellt von LewisLewis
vor mehr als 10 Jahre
|
|
Neuro-opthalmology
- Visual loss
- Amsler grid
- In maculopathies the lines appear curved or broken (metamorphopsia)
- In maculopathies the lines appear curved or broken (metamorphopsia)
- Pinhole is used to test visual acuity
- Cataract and keratoconus improve with
the pinhole, while optic neuritis doesn't
- Cataract and keratoconus improve with
the pinhole, while optic neuritis doesn't
- Color vision test helps you identify lesions at the level
of the macula, of the optic nerve or at the chiasm
- Causes
- Optic neuropathy
- Eye disease
- Lesion in the intracranial visual pathway
- Optic neuropathy
- Monocular visual loss results from lesions anterior to the chiasm,
so to the optic nerve or to the eye itself; binocular visual loss results
from lesions at the level of the chiasm or posterior to the chiasm
- Visual field testing is helpful to localize and
identify diseases affecting the visual pathways
- You can test the visual field very simply with confrontation
in the office or with automated stated perimetry
- You can test the visual field very simply with confrontation
in the office or with automated stated perimetry
- The relationship between the retina and the visual field is opposite and reverse
- Span of the visual field
- 60° superiorly, 75° inferiorly
- 60° on the nasal side, 100° on the temporal side
- 60° superiorly, 75° inferiorly
- Automated static perimetry
- The most quantitative and sensible and
reproducible technique to detect visual field deficits
- The most quantitative and sensible and
reproducible technique to detect visual field deficits
- 4 rules to help us to understand
better the location of the defects
- The more congruous the defect, the more posterior the lesion
- In chiasmatic lesions you always have bitemporal
visual defects, also know as tunnel vision
- In posterior lesions you can pretend your back
head is against retina in order to locate the lesion
- Occipital lesions spare the macula
- Occipital part in fact presents 2 different vascular
supplies: posterior and medial cerebral artery
- Occipital part in fact presents 2 different vascular
supplies: posterior and medial cerebral artery
- The more congruous the defect, the more posterior the lesion
- Monocular lesions anterior to the chiasm
do not respect the vertical meridian
- Binocular lesions instead respect the vertical meridian
- Tools needed for a neuro-opthalmic examination at bedside
- Near card to check visual acuity
- A pair of reading glasses
- A pinhole
- A red object
- A striped ribbon or paper to test optokinetic nystagmus
- An Amsler grid
- Short-lasting dilating drops
- A direct opthalmoscope
- Near card to check visual acuity
- Amsler grid
- Diplopia
- Due to alterations in the movement of the eye
- Maddox rod test is used to recognize small differences in motility
- Maddox rod test is used to recognize small differences in motility
- Monocular diplopia is not related to neurological disorders, but to optical problems
- Binocular diplopia could result from
- Extraocular muscle disordes
- CN lesion (III, IV, VI)
- Thyroidal disease can involve these muscles
- Others
- Inflammatory disorders
- Tumors
- Infections
- Orbital venous congestion
- Trauma
- Giant cell arteritis (Horton's)
- Progressive myopathies
- Inflammatory disorders
- CN lesion (III, IV, VI)
- Neuromuscular junction disease
- Myasthenia gravis
- 50% of patients present with diplopia or ptosis
- You can test with the rest test or eye-pack test
- Pupils are never involved
- 50% of patients present with diplopia or ptosis
- Myasthenia gravis
- Inter/supra-nuclear pathways disease
- Extraocular muscle disordes
- Due to alterations in the movement of the eye
- CN III palsy
- Etiology
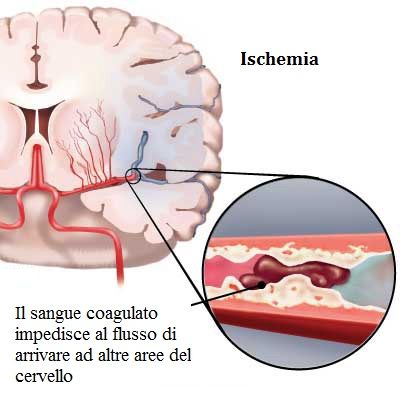
- Ischemia
- Check if patient is diabetic or has hypertension
- It occurs in the deeper part of the nerve,
sparing the superficial parasympathetic fibers
- If we find an enlarged pupil, ask for MRI or
angiography to identify compressive site
- If no pupil enlargement, check the BP or the glucose
- If we find an enlarged pupil, ask for MRI or
angiography to identify compressive site
- Check if patient is diabetic or has hypertension
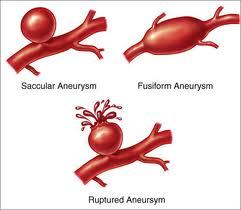
- Aneurysmatic compression
- Ischemia
- Etiology
- CN VI palsy
- Always check intracranial pressure
- The nerve is very susceptible when it enters
the cavernous sinus, where it tilts of 90°
- The nerve is very susceptible when it enters
the cavernous sinus, where it tilts of 90°
- Patients usually tilt the head in order to avoid double vision
- Always check intracranial pressure
- CN IV palsy
- Typically patients, to compensate for the
diplopia, tilt the head away from the lesion
- Hardest palsy to recognize
- Hardest palsy to recognize
- Causes
- 1/3 ischemical
- 1/3 congenital
- Especially in children
- Especially in children
- 1/3 due to injuries or tumor compression
- Especially in elderly
- Especially in elderly
- 1/3 ischemical
- Typically patients, to compensate for the
diplopia, tilt the head away from the lesion
- Multiple nerve palsy
- Typically in cavernous sinus and orbital apex
- Cavernous sinus syndrome
- Opthalmoplegia (multiple cranial nerve palsies)
- Horner Sd (sympathetic)
- Pain (trigeminal nerve)
- Proptosis and periorbital edema (if venous hypertension)
- Opthalmoplegia (multiple cranial nerve palsies)
- Orbital apex syndrome
- Ophthalmoplegia (multiple cranial nerve palsies)
- Horner Sd
- Pain (trigeminal nerve)
- Visual loss (optic neuropathy) – not present in cavernous sinus syndrome)
- Ophthalmoplegia (multiple cranial nerve palsies)
- Cavernous sinus syndrome
- Typically in cavernous sinus and orbital apex
- Anisocoria
- Unequal size of the pupils
- It can reveal a serious problem, like aneurysmatic compression in CN III palsy
- We should always check the pupils in the
light, in the dark, near and at a distance
- Pupils are controlled by a steady balance between
parasympathetic (CN III) constriction and sympathetic dilation
- 20% of people have physiologic anisocoria
- Always the same both in light and in the dark and it may switch side or go away
- Always the same both in light and in the dark and it may switch side or go away
- Unequal size of the pupils
- Myosis
- Sympathetic defect
- Horner syndrome
- Carotid dissection is the most important cause
- Traumatic causes (severe neck injury)
- Spontaneous (trivial events)
- Most frequent cause of myosis, if you can exclude
ocular problems or pharmacological problems
- Characterized by unilateral myosis with dilation lag in the dark, mild
ptosis due to Muller muscles paralysis and by pseudoenophthalmos
- Carotid dissection is the most important cause
- Pharmacological test can be done to localize
the lesion (not to make the diagnosis)
- Apraclonidine helps to differentiate
preganglionic from post-ganglionic lesions
- In post-ganglionic lesions it dilates the normal
pupil, while it doesn't affect the damaged pupil
- In pre-ganglionic lesions it creates an inverted anisocoria
where the affected pupil dilates more than the normal one
- In post-ganglionic lesions it dilates the normal
pupil, while it doesn't affect the damaged pupil
- Apraclonidine helps to differentiate
preganglionic from post-ganglionic lesions
- Sympathetic defect
- Mydriasis
- Most common causes
- Tonic pupil (Adie pupil)
- Most common parasympathetic palsy
- It features acute denervation (injury to short ciliary nerve, pupil and accommodation
fibers) and aberrant reinnervation (accommodative fibers innervate iris sphincter)
- Most common parasympathetic palsy
- CN III palsy
- Tonic pupil (Adie pupil)
- Associated situations
- Unilateral mydriasis
- Loss of accommodation
- Better constriction at near
- Sectorial palsy of iris sphincter
- Slow tonic redilation
- Supersensitivity to pilocarpine (parasympathomimetic) (0.1%)
- We can exploit this for diagnostic purposes
- If myosis at 0.1: Adie pupil
- If myosis at 1: 3rd nerve palsy
- If myosis at 2.5: pharmacological midriasis (e.g. cocaine)
- If myosis at 0.1: Adie pupil
- We can exploit this for diagnostic purposes
- Unilateral mydriasis
- Most common causes
- The blind spot is in the temporal zone
- Optic neuritis
- Inflammatory, infective or demyelinating
process affecting the optic nerve
- Classification
- Opthalmoscopic classification
- Retrobulbar neuritis
- Most frequent type in adults and frequently associated with MS
- Most frequent type in adults and frequently associated with MS
- Papillitis
- Most common type in children
- Most common type in children
- Neuroretinitis
- Painless unilateral visual impairment which starts
gradually and then becomes severe after about a week
- Painless unilateral visual impairment which starts
gradually and then becomes severe after about a week
- Retrobulbar neuritis
- Etiological classification
- Demyelinating
- Causes
- Isolated optic neuritis
- MS (most common)
- Devic disease (neuromyelitis optics)
- Schilder disease
- Isolated optic neuritis
- Treatment
- Intravenous methylprednisolone
- Intramuscular interferon beta-1a
- Intravenous methylprednisolone
- Most common
- Causes
- Parainfectious
- Optic neuritis may be associated with various viral infections
- Optic neuritis may be associated with various viral infections
- Infectious
- Sinus-related
- Cat-scratch fever
- Syphilis
- Lime disease
- Cryptococcal meningitis
- VZV
- Sinus-related
- Non-infectious
- Sarcoid
- Autoimmune
- Sarcoid
- Demyelinating
- Opthalmoscopic classification
- Non-arteritic anterior ischemic optic neuropathy
- Caused by occlusion of the short posterior ciliary arteries
resulting in partial or total infarction of the optic nerve head
- Caused by occlusion of the short posterior ciliary arteries
resulting in partial or total infarction of the optic nerve head
- Arteritic aterior ischemic optic neuropathy
- Caused by giant cell arteritis
- Granulomatous necrotizing arteritis with a
predilection for large and medium-sized arteries
- Granulomatous necrotizing arteritis with a
predilection for large and medium-sized arteries
- Presentation with sudden unilateral visual loss
which may be accompanied by periocular pain
- Treatment
- Methylprednisolone
- Antiplatelet therapy
- Immunosuppressives
- Methylprednisolone
- Caused by giant cell arteritis
- Inflammatory, infective or demyelinating
process affecting the optic nerve
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.