11450479
Laila was losing weight
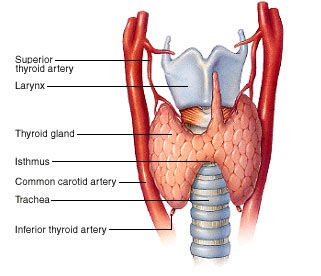
- Thyroid gland
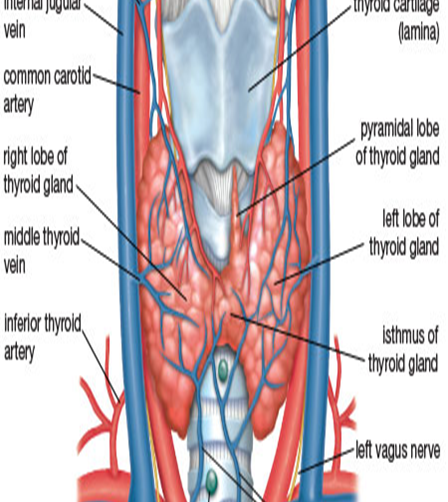
- Anatomy of the thyroid gland
- Blood supply
- Lymphatics
- Upper part of the gland to upper deep cervical nodes via the prelaryngeal, pretracheal & paratracheal
nodes.
- Lower part to lower deep cervical nodes. The lymphatic's form a plexus & lymph can drain in any
direction.
- Upper part of the gland to upper deep cervical nodes via the prelaryngeal, pretracheal & paratracheal
nodes.
- Nerve supply
- Supplied by superior, middle & inferior cervical sympathetic ganglia.
- Fibers: Vasomotor & not secreto-motor
- Supplied by superior, middle & inferior cervical sympathetic ganglia.
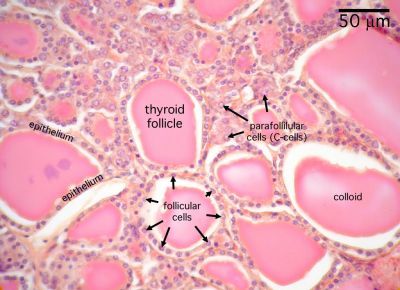
- Histology of the thyroid gland
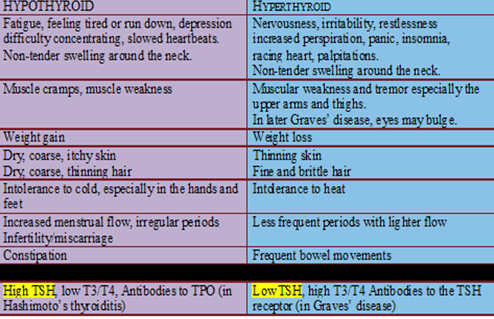
- Hyperthyroidism vs Hypothyroidism
- Hyperthyroidism
- What is it?
- Hyperthyroidism, or overactive thyroid, happens when the thyroid gland produces too much thyroid
hormone. This has an impact throughout the body.
- Hyperthyroidism, or overactive thyroid, happens when the thyroid gland produces too much thyroid
hormone. This has an impact throughout the body.
- Causes
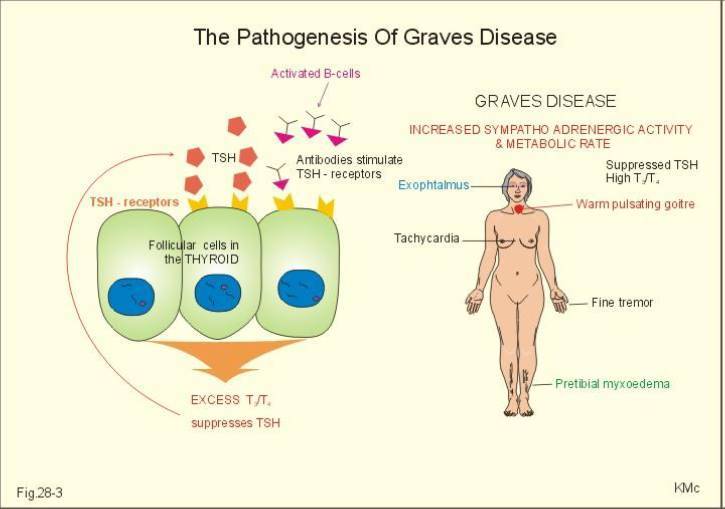
- Graves' Disease
- Functioning adenoma and toxic multinodular goiter (TMNG
- Excessive intake of thyroid hormones
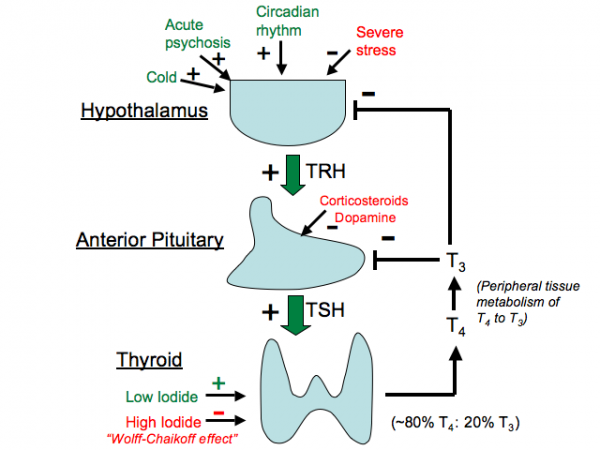
- Abnormal secretion of TSH
- Thyroiditis (inflammation of the thyroid gland)
- Excessive iodine intake
- Graves' Disease
- Risk factors
- Females
- Being older than age 60
- Exposure to radiation in the neck
- Prior thyroid surgery
- Having a family history of thyroid disease
- Having a family history of autoimmune disease
- Having an autoimmune disease
- Being of Caucasian or Asian ethnicity
- Experiencing hormonal changes due to pregnancy, childbirth, or menopause
- Personal history of lithium use
- Having chromosomal abnormalities like Down syndrome or Turner's syndrome
- Females
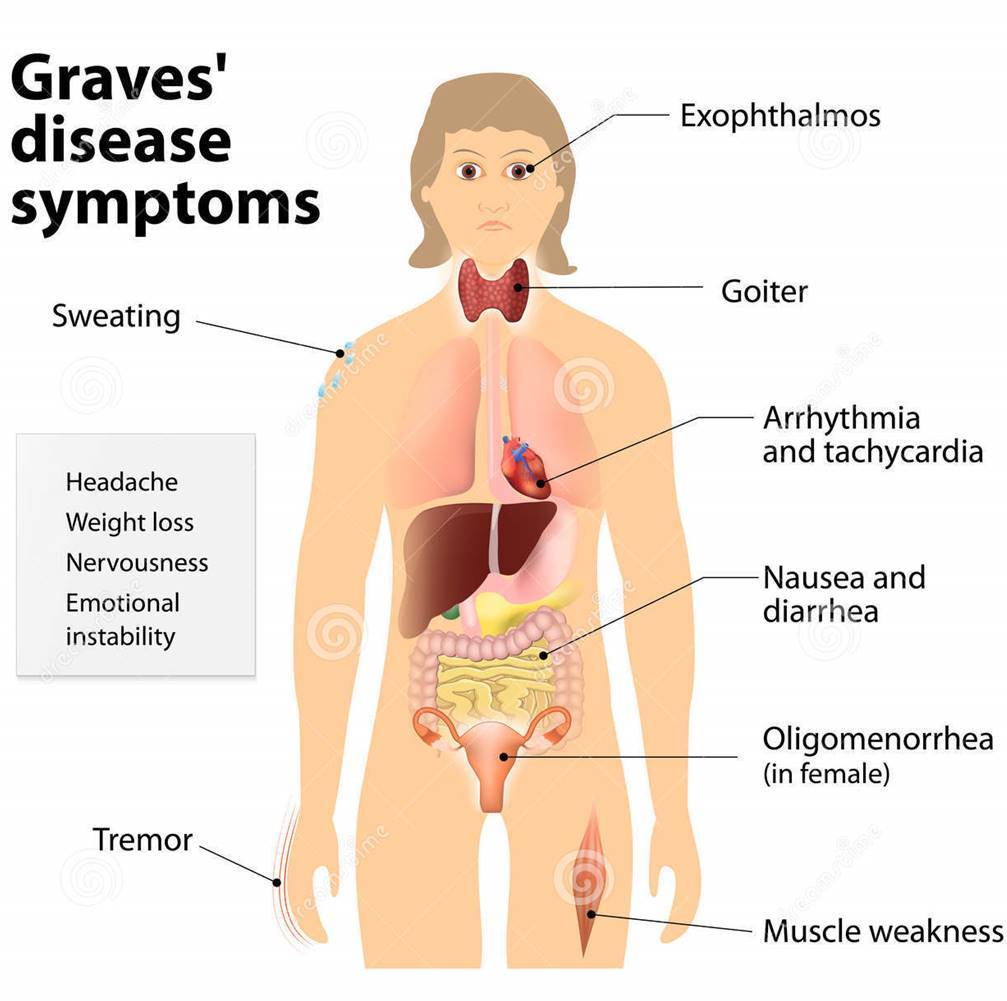
- Sign & symptoms
- Anxiety \irritability
- Fine tremors
- Increase in perspiration or warm, moist skin
- Weight loss
- Goiter
- Change in menstrual cycles
- Erectile dysfunction or reduced libido
- Frequent bowel movements
- Graves' ophthalmopathy
- Fatigue
- Graves' dermopathy
- Palpitations
- Anxiety \irritability
- Epidemiology
- Westernization and nutrition transition in Arab world have increased the burden of
adenocarcinomas, including thyroid cancer
- The review showed that the prevalence of different types of thyroid disease varied between the
reported studies in Arab world ranging from 6.18 to 47.34% prevalence of goiter reported by several
studies conducted in Arab world, such as Egypt, Algeria and Bahrain with 25.25, 86 and 1.7%,
respectively
- Westernization and nutrition transition in Arab world have increased the burden of
adenocarcinomas, including thyroid cancer
- Treatment
- Pharmacological
- Thionamides
- General Pharmacokinetics:
- Rapidly absorbed orally.
- Half life 1-6 hours.
- Metabolized by the liver
- Excreted in the urine
- Both cross the placenta and
appear in breast milk
- Rapidly absorbed orally.
- Methimazole
- Propylthiouracil
- Comparision
- Dosing
- Usual starting dose – Carbimazole(derivative of methimazole) 30 – 60 mg a day or propylthiouracil
50-100 mg/day
- The dose and frequency should be reduced after 4-6 weeks
- Usual maintenance dose of carbimazole is 2.5 – 15 mg/day.
- Usual starting dose – Carbimazole(derivative of methimazole) 30 – 60 mg a day or propylthiouracil
50-100 mg/day
- Side effects
- Agrancylocytosis
- The patient have to stop the medications
if he developed fever –sore thorat –mouth
ulcers
- Vasculitis –hepatitis-lupus like syndrome
- Agrancylocytosis
- General Pharmacokinetics:
- B-Blockers
- Propanolol
- Mechanism of action
- reduce the cardiac manifestations
- help in relaxing the patient (sedation).
- the only BB that can inhibit deiodinase enzyme
- reduce the cardiac manifestations
- Mechanism of action
- Propanolol
- Thionamides
- Surgical
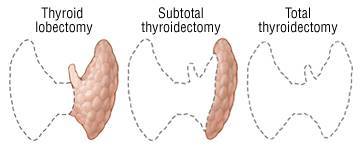
- Thyroidectomy
- What is it?
- Removal of all or part of your thyroid gland.
- Used to treat thyroid disorders, such as cancer, noncancerous enlargement of the thyroid (goiter) and
overactive thyroid (hyperthyroidism).
- Removal of all or part of your thyroid gland.
- Indications
- Thyroid cancer
- Goiter
- Hyperthyroidism
- Thyroid cancer
- Contraindications
- Uncontrolled severe hyperthyroidism (ie, Graves disease) --> intraoperative or postoperative thyroid
storm.
- Uncontrolled severe hyperthyroidism (ie, Graves disease) --> intraoperative or postoperative thyroid
storm.
- Long term effect
- Partial thyroidectomy
- The remaining portion typically takes over the function of the entire thyroid gland, and you might not
need thyroid hormone therapy.
- The remaining portion typically takes over the function of the entire thyroid gland, and you might not
need thyroid hormone therapy.
- Complete thyroidectomy
- Without replacement you'll develop signs and symptoms of underactive thyroid (hypothyroidism). As
a result, you'll need to take a pill every day that contains the synthetic thyroid hormone
levothyroxine.
- Without replacement you'll develop signs and symptoms of underactive thyroid (hypothyroidism). As
a result, you'll need to take a pill every day that contains the synthetic thyroid hormone
levothyroxine.
- Partial thyroidectomy
- What is it?
- Thyroidectomy
- Pharmacological
- Prognosis
- Good with appropriate treatment.
- Patient should be screened & treated for osteoporosis & atherosclerotic risk factors
- Increased risk of obesity & insulin resistance Previously treated for hyperthyroidism
- Good with appropriate treatment.
- Types
- Diffuse toxic goiters- Graves disease
- Pathophysiology
- What is it?
- Autoimmune disorder
- An immunoglobulin called thyroid-stimulating immunoglobin (TSI) found in the blood of all patients;
TSI binds to the TSH receptor and induce TSH-like effects; TSI effects persist longer than TSH (up to 12
hrs vs. 1 hr respectively) Plasma level of TSH is suppressed due to the high level of thyroid hormones
- Females are more at risk
- Autoimmune disorder
- Signs & Symptoms
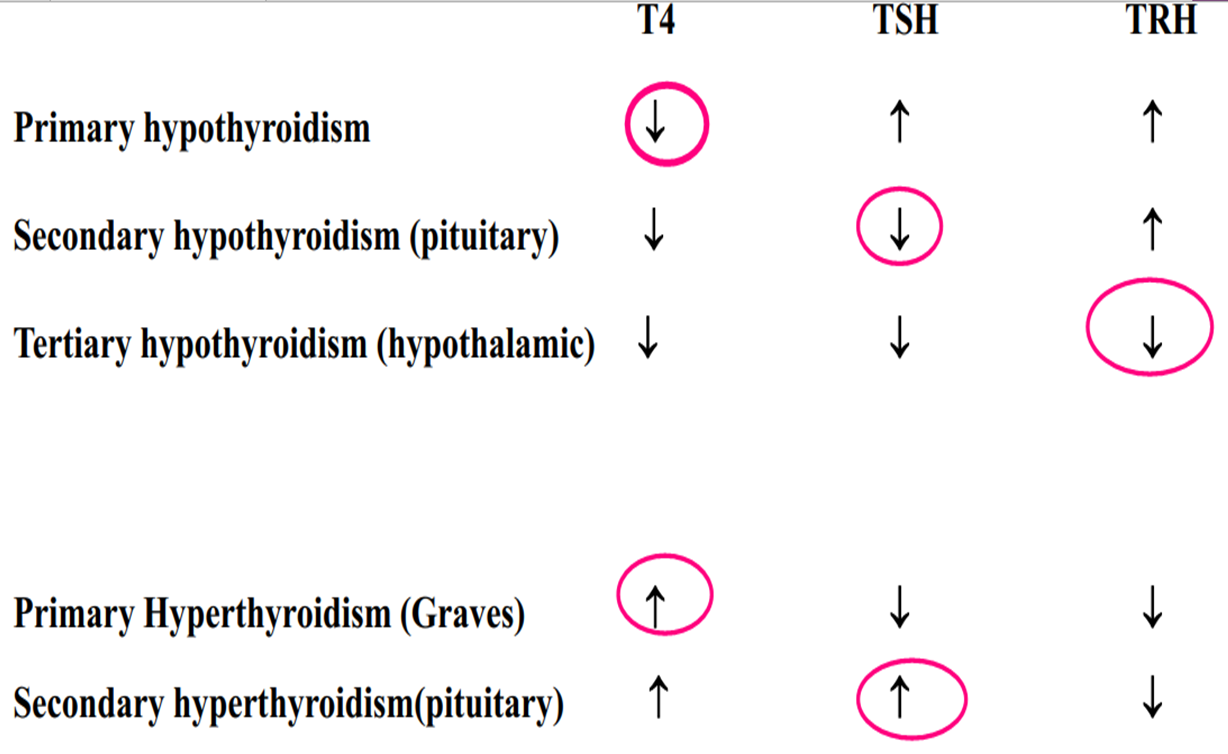
- Diagnosis
- TSH is deccreased & free T4 is increased
- Thyroid auto antibodies
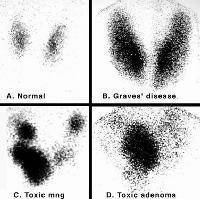
- Nuclear thyroid scintigraphy (I123, Te99)
- TSH is deccreased & free T4 is increased
- Pathophysiology
- Thyroditis
- Pituitary Adenoma (TSHoma)
- Exogenous Administration (Thyrotoxicosis Factitia)
- Toxic Multinodular Goiters
- Diffuse toxic goiters- Graves disease
- Diagnosis
- History taking
- Physical examination
- Lab Investigation
- Blood test
- Blood test
- History taking
- What is it?
- Physiology of thyroid gland
- Anatomy of the thyroid gland
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.