15812915
Beschreibung
Mindmap von Violet Biskup, aktualisiert more than 1 year ago
|
|
Erstellt von Violet Biskup
vor etwa 6 Jahre
|
|
Left-Sided Heart Failure
- Main Causes
(American Heart
Association, 2017))
- Coronary Artery
Disease
- The coronary arteries
become narrowed or
blocked, which reduces
blood flow to the heart
(Heart & Stroke Foundation,
2018)
- The coronary arteries
become narrowed or
blocked, which reduces
blood flow to the heart
(Heart & Stroke Foundation,
2018)
- High Blood
Pressure
- The Blood pressure in the arteries
is elevated and the heart must
work harder than normal to pump
blood through the vessels (Heart
& Stroke Foundation, 2018)
- The Blood pressure in the arteries
is elevated and the heart must
work harder than normal to pump
blood through the vessels (Heart
& Stroke Foundation, 2018)
- Previous Heart Attacks
(myocardial infarction)
- Depending on how long the
blood supply is cut off
during a MI, the damage
can be mild, severe or
cause lifelong problems
(Heart & Stroke
Foundation, 2018)
- Depending on how long the
blood supply is cut off
during a MI, the damage
can be mild, severe or
cause lifelong problems
(Heart & Stroke
Foundation, 2018)
- Other Causes
(Heart & Stroke
Foundation, 2018)
- Excessive Use of
Alcohol & Drugs
- Diabetes
- Being obese or
overweight
- High Blood Cholesterol
- Heart Valve Disease
- Myocarditis
- Heart muscle disease of
unknown causes
- Other Medical Conditions;
thyroid diseases or anemia
- Excessive Use of
Alcohol & Drugs
- Coronary Artery
Disease
- Classification
- The Left ventricle of the heart supplies
most of the heart's pumping power
and is the largest chamber making it
essential for normal function
(American Heart Association, 2017)
- Left-sided HF is the most common form of initial HF
and results from left ventricular dysfunction. This
causes blood to back up through the left atrium and
into the pulmonary veins. This increased pulmonary
pressure causes fluid extravasation from the
pulmonary capillary bed into the interstitium and
the the alveoli, which is then manifested as
pulmonary congestion and edema (Lewis 2014)
- There are two types of Left-sided HF
(American Heart Association, 2017)
- Heart Failure with reduced
ejection fraction (HFrEF), also
called systolic failure:
- The left ventricle loses its ability to contract
normally, which means the heart cannot pump
with enough force to push enough blood into
circulation
- The left ventricle loses its ability to contract
normally, which means the heart cannot pump
with enough force to push enough blood into
circulation
- Heart Failure with Preserved
ejection fraction (HFpEF), also
called diastolic failure:
- The Left ventricle loses its ability to relax normally
due to the muscle becoming stiff. This makes it so
the heart cannot fill properly with blood during
the resting period between each beat
- The Left ventricle loses its ability to relax normally
due to the muscle becoming stiff. This makes it so
the heart cannot fill properly with blood during
the resting period between each beat
- Heart Failure with reduced
ejection fraction (HFrEF), also
called systolic failure:
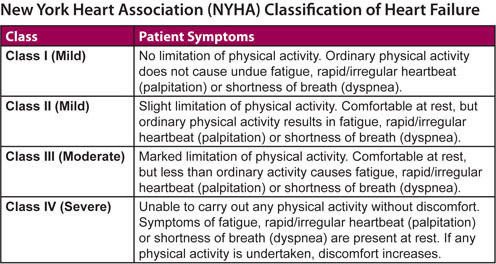
- The Severity of Heart failure
based on symptoms is classified using the
New York Heart Association Functional
Classification (American Heart Association,
2017)
- Figure 1: (Hamilton Cardiology
Associates, 2018)
- Figure 1: (Hamilton Cardiology
Associates, 2018)
- There are two types of Left-sided HF
(American Heart Association, 2017)
- Left-sided HF is the most common form of initial HF
and results from left ventricular dysfunction. This
causes blood to back up through the left atrium and
into the pulmonary veins. This increased pulmonary
pressure causes fluid extravasation from the
pulmonary capillary bed into the interstitium and
the the alveoli, which is then manifested as
pulmonary congestion and edema (Lewis 2014)
- The Left ventricle of the heart supplies
most of the heart's pumping power
and is the largest chamber making it
essential for normal function
(American Heart Association, 2017)
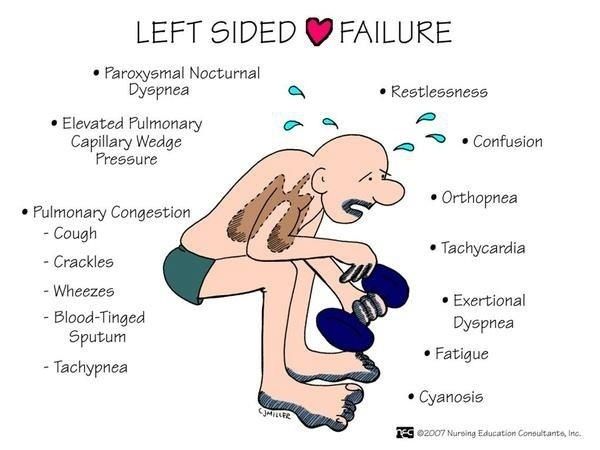
- Manifestations
(Lewis, 2014;
McMaster
Pathophysiology
Review, 2018)
- Signs
- LV heaves
- Cheyne-strokes
respirations
- Pulsus alternans
- alternating pulses: strong -
weak
- alternating pulses: strong -
weak
- Increased Heart Rate
- Crackles
- Pulmonary edema
- Pulmonary edema
- S3 and S4
- Decreased PaO2,
slight increased
PaCO2
- Poor O2 exchange
- Poor O2 exchange
- Cardiac
"asthma"
- Coarse ronchi and wheezing caused by
compression of conduction airways by
pulmonary congestion
- Coarse ronchi and wheezing caused by
compression of conduction airways by
pulmonary congestion
- Mitral Regurgitation Murmur
- cardiomegaly
- chronically increased workload and
excessive volume cause ventricular
dilation and hypertrophy
- chronically increased workload and
excessive volume cause ventricular
dilation and hypertrophy
- PMI displaced inferiorly
and posteriorly
- LV hypertrophy
- LV hypertrophy
- LV heaves
- Symptoms
- Fatigue
- Dyspnea
- shallow respirations < or = 32-40/min
- shallow respirations < or = 32-40/min
- Orthopnea
- SOB in recumbent
position
- SOB in recumbent
position
- Dry Hacking cough
- Pulmonary Edema
- Nocturia
- Paroxysmal nocturnal dyspnea
- Confusion and/or impaired
memory
- Decreased Urine Output
- Chest
pain/pressure
- Palpitations
- Cachexia
- Fatigue
- Figure 3: (Google images, 2016)
- Signs
- Diagnostic Studies
(Lewis, 2014)
- Brain natriuretic peptide
- a biomancer used by left
ventricle when there is
excessive pressure due to
hear failure
- < 100 = no heart failure;
100-300 = HF present
- >300 = mild: >600 = moderate:
>900 = severe HF
- >300 = mild: >600 = moderate:
>900 = severe HF
- < 100 = no heart failure;
100-300 = HF present
- a biomancer used by left
ventricle when there is
excessive pressure due to
hear failure
- Chest
x-ray
- if there is any congestion,
enlarged
- if there is any congestion,
enlarged
- echocardiogram
- Nuclear stress test
- Health History & Physical
Examination
- CBC, Cardiac enzymes, thyroid
function studies, and LFT
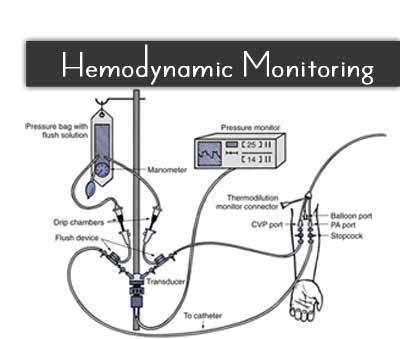
- Hemodynamic Monitoring
- Figure 5: (Google images, 2017)
- Figure 5: (Google images, 2017)
- Figure 4: (Google images, 2015)
- Brain natriuretic peptide
- Treatment &
Managment
- Administering Medications
(Lewis, 2014;
Lilley, Collins,
& Synder,
2014)
- Decrease preload
- Diuretics
- Side effects
- Allergic reaction, low or
high K+, ototoxicity,
nephrotoxicity
- Allergic reaction, low or
high K+, ototoxicity,
nephrotoxicity
- Nursing Consideration
- Assess client's vitals especially BP,
Kidney function tests, allergies,
sigs of ototoxicity , K+ and Na
- Assess client's vitals especially BP,
Kidney function tests, allergies,
sigs of ototoxicity , K+ and Na
- Side effects
- Diuretics
- Decrease afterload
- ACE inhibitors and ARBS
- Side effects
- nagging cough, low BP, high K+,
allergic reactions, mood changes,
angioedema, fatigue, dizziness,
headache
- nagging cough, low BP, high K+,
allergic reactions, mood changes,
angioedema, fatigue, dizziness,
headache
- Nursing Consideration
- Assess for allergies,
BP, electrolytes,
especially K+,
Kidney function
tests
- Assess for allergies,
BP, electrolytes,
especially K+,
Kidney function
tests
- Side effects
- ACE inhibitors and ARBS
- Reduce anxiety
- Morphine
- Side effects
- Low RR, sedation, nausea,
vomiting, constipation,
hypotension, allergic rxns such
as itching and rash
- Low RR, sedation, nausea,
vomiting, constipation,
hypotension, allergic rxns such
as itching and rash
- Nursing Consideration
- Assess for anxiety, allergic rxn, signs of
respiratory depression, encourage clients
to eat food that are high in fiber, monitor
clients vitals, encourage turning and deep
breathing
- Assess for anxiety, allergic rxn, signs of
respiratory depression, encourage clients
to eat food that are high in fiber, monitor
clients vitals, encourage turning and deep
breathing
- Side effects
- Morphine
- Improve cardiac function
- eg digoxin
- side effects
- GI upset, headache, Colored
vision, halo vision, flickering
lights low K+, low Mg, high Ca,
narrow therapeutic index
- GI upset, headache, Colored
vision, halo vision, flickering
lights low K+, low Mg, high Ca,
narrow therapeutic index
- Nursing
consideration
- narrow therapeutic index so monitor Blood
levels, K+, HR, BP, cardiac rhythms, signs of
toxicity, avoid foods high in fiber, weigh daily
- narrow therapeutic index so monitor Blood
levels, K+, HR, BP, cardiac rhythms, signs of
toxicity, avoid foods high in fiber, weigh daily
- side effects
- eg digoxin
- Decrease preload
- Collaborative
Care (Lewis,
2014;
Pasoz-Lopez et
al., 2011)
- High fowler's position
- Administer O2 as required
- Cardiac monitoring and O2 sat
- Monitor BP, HR, RR, Urinary output q1h
- Monitoring IABP, PAOP, CO
- Weighing client's
daily
- Na restriction to 2-3g
- Fluid restriction to 2-3 l
- Regular activity and rest
- Vaccination Flu+ pneumonia
- Smoking cessation and limiting ETOH
- High fowler's position
- Administering Medications
(Lewis, 2014;
Lilley, Collins,
& Synder,
2014)
- Client-Centered
Care (Robbio,
2018)
- Understand that nursing is more than performing technical skills (RNA0, 2015)
- Establish an authentic relationship that is based on trust and respect (Messner, 1993)
- Value the uniqueness of every client (Robbio, 2018)
- Embody holistic and caring attitude (Cara, 2003)
- Implement Watson's theory of Human Caring such as adopting caring consciousness (Cara, 2003)
- Recognize that clients are the expert of their lives (Robbio, 2018)
- Support client's healthcare decisions (Robbio, 2018)
- Adopt a non-judgemental attitude (Robbio, 2018)
- Involve the family in the care (RNAO, 2015; Robbio, 2018)
- Figure 6: (Google images, 2018)
- Understand that nursing is more than performing technical skills (RNA0, 2015)
- Risk Factors
(Heart & Stroke
Foundation, 2018)
- Unhealthy Eating
- Unhealthy Weight
- Not enough exercise
- Smoking
(Tabacco use)
- Too much
alcohol
- Birth control and
Hormone
Replacement
Therapy (HRT)
- Recreational Drug Use
- Stress
- Figure 2: (Heart & Stroke
Foundation, 2018)
- Unhealthy Eating
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.