3886521
Psychoses
- What do we mean by psychotic?
- Community images or stereotypes of
being out of touch with reality
- Symptoms that are out of touch with reality
- Disorders where those symptoms dominate
- Community images or stereotypes of
being out of touch with reality
- Symptom groups in Schizophrenia
- 1. Negative symptoms
- Avolition
- Alogia
- Affective flattening
- Avolition
- 2. Psychotic symptoms
- Delusions
- Hallucinations
- Delusions
- 3. Disorganisation symptoms
- Thought disorder
- Bizarre behaviour
- Thought disorder
- 1. Negative symptoms
- Schizophrenia Spectrum & other
psychotic disorders
- Schizotypal (Personality) Disorder
- Delusional Disorder
- Brief Psychotic Disorder
- Schizophreniform Disorder
- Schizophrenia
- Schizoaffective Disorder
- Psychotic disorder due to (medical condition) -
Substance/Medication-Induced Psychotic Dis.
- Schizotypal (Personality) Disorder
- What causes psychotic disorders?
- Genetic model
- 60% of monozygotic twins are concordant for
schizophrenia vs. 10% of fraternal twins
- This is strong evidence that genes can
play a role in causation of schizophrenia
- It is also strong evidence that genes are not a
sufficient condition for emergence of schizophrenia
- 60% of monozygotic twins are concordant for
schizophrenia vs. 10% of fraternal twins
- Neurotransmitter models
- Neurotransmitters such as dopamine can
be overactive (& misdirected) in
schizophrenia
- 'Antipsychotic' medications blocking dopamine
receptors can reduce some symptoms
- Logical Hypothesis: neurotransmitter
dysregulation ‘causes’ schizophrenia
- Neurotransmitters such as dopamine can
be overactive (& misdirected) in
schizophrenia
- Neurodevelopmental model
- Brain maturation processes (e.g., cell
migration, pruning of connections)
seem to be less fully realised in people
with schizophrenia
- Structural brain abnormalities may be
evident before onset of the disorder, and
may change little over time
- Brain maturation processes (e.g., cell
migration, pruning of connections)
seem to be less fully realised in people
with schizophrenia
- Genetic model
- Psychological models
- Both neuropsychological factors (deficits) and
cognitive factors (biases) have been implicated
- Information processing deficits:
e.g. source monitoring – is this
“voice” from me or not?
- Reasoning biases: e.g. Jumping to conclusions –
deluded individuals use insufficient information
before reaching a conclusion
- Distorted appraisals: e.g. In paranoia, an
“external & personalising” bias – i.e.
attribution of negative events to others
rather than self or the situation
- Information processing deficits:
e.g. source monitoring – is this
“voice” from me or not?
- Both neuropsychological factors (deficits) and
cognitive factors (biases) have been implicated
- Cannabis & Schziophrenia
- Cross sectional studies show an
association between cannabis
dependence and schizophrenia
- Longitudinal study: Heavy cannabis users at age
18 were 2.3 times more likely to have a
schizophrenia admission by age 33 after
controlling for pre-existing psychiatric problems
- Implications: Heavy use
of mind altering drugs
can increase the risk for
schizophrenia... ...but
only a minority of drug
abusers will get the
disorder
- Implications: Heavy use
of mind altering drugs
can increase the risk for
schizophrenia... ...but
only a minority of drug
abusers will get the
disorder
- Cross sectional studies show an
association between cannabis
dependence and schizophrenia
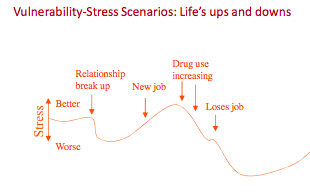
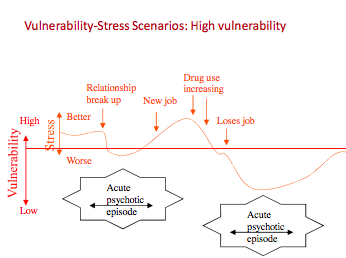
- Vulnerability-stress-coping model
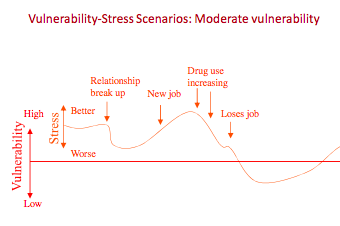
- Vulnerability
- Contributed to by genetic and biological
factors, and other enduring problems
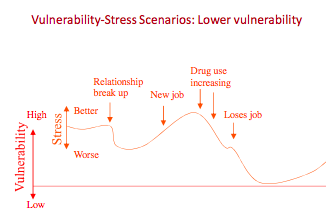
- All people can be considered to have
vulnerability, but to different degrees
- Contributed to by genetic and biological
factors, and other enduring problems
- Stressors
- Any factors that tax our ability to cope
- May arise from life events stressful to anyone, or from
stressors unique to the person, including daily hassles
- Can be external to the person(e.g.,exam stress) or internal
(e.g., using mind altering drugs; maturational changes)
- Any factors that tax our ability to cope
- Coping
- Automatic and deliberate actions
taken to restore well-being
- Automatic and deliberate actions
taken to restore well-being
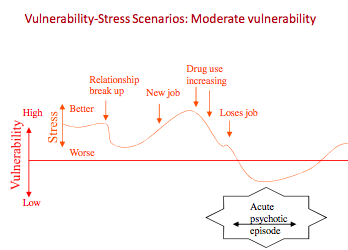
- Central idea
- The occurrence of episodes of a disorder is
dependent on the relative levels of
vulnerability, stress and coping responses
- The experience of stress automatically leads the
person to attempt adaptation
- Successful coping is contributed to by
both “coping effort” and “competence”
- Coping breakdown allows the psychopathology to erupt
- The occurrence of episodes of a disorder is
dependent on the relative levels of
vulnerability, stress and coping responses
- Evidence for vulnerability
- Adolescents at high risk for psychosis
have detectable neurocognitive deficits
- Processing speed, sustained attention, memory
- Processing speed, sustained attention, memory
- People with psychosis have high
incidence of impaired sustained
attention
- so do their children
- so do those who have recovered
- so do their children
- Relatives have increased incidence
of schizotypal personality traits,
auditory processing irregularities
- Adolescents at high risk for psychosis
have detectable neurocognitive deficits
- Does stress precipitate episodes?
- Life event stressors are strongly
associated with worsening symptoms in
the months leading up to relapse of
schizophrenia and with onset of
depression
- Daily hassles are also
implicated in relapses ̶ And in
symptom exacerbation And in
onset of sub-clinical symptoms
in the normal population
- Life event stressors are strongly
associated with worsening symptoms in
the months leading up to relapse of
schizophrenia and with onset of
depression
- Benefits
- Explains the episodic nature of psychosis
whilst recognising the possibility of enduring
deficits in brain structure or function ̶ i.e.,
incomplete cell migration may be a
vulnerability, but an episode of psychosis
requires either an increase in stress or a
breakdown in current coping to emerge
- Can engender hope: people are not simply passive
victims of their vulnerability or of stressors ̶ Stress
can potentially be managed by coping actions
- Prompts a wide range of interventions ̶ e.g., if
medication (a way of reducing vulnerability) is
insufficient to restore equilibrium, reduction of
stressors, or coping skills development can be instituted
- Explains the episodic nature of psychosis
whilst recognising the possibility of enduring
deficits in brain structure or function ̶ i.e.,
incomplete cell migration may be a
vulnerability, but an episode of psychosis
requires either an increase in stress or a
breakdown in current coping to emerge
- Vulnerability
- Evidence-based treatments for Schizophrenia
- ‘Antipsychotic’ medications
- Theoretical rationale
- Excess release of a
neurotransmitter can be
treated by blocking its
receptors (with an alternative
chemical).
- Antipsychotics target
dopamine D2 receptors,
(and others)
- Excess release of a
neurotransmitter can be
treated by blocking its
receptors (with an alternative
chemical).
- Antipsychotics include:
- risperidone, olanzapine,
amisulpride, aripiprazole,
clozapine
- risperidone, olanzapine,
amisulpride, aripiprazole,
clozapine
- Benefits
- Reduction/cessation of positive
(‘psychotic’) symptoms in a majority of
patients
- Reduction/cessation of positive
(‘psychotic’) symptoms in a majority of
patients
- Limitations
- Incomplete remission of positive
symptoms in many patients
- Little benefit for negative
symptoms, except for Clozapine
- Side effects may include akathisia, weight gain,
hypersalivation, photosensitivity, impotence, fits, etc.
- Incomplete remission of positive
symptoms in many patients
- In general, antipsychotics have
similar efficacy in reduction or
cessation of positive symptoms in
the acute phase: 2/3 patients
show considerable gain
- However, some patients
recover from acute phases
without medication
- Maintenance antipsychotic medication
following an acute episode is effective
in reducing the risk of relapse
- 14 -21% of patients on medication relapse
within 9 months, Vs. 55% of patients on
placebo relapse within 9 months
- 14 -21% of patients on medication relapse
within 9 months, Vs. 55% of patients on
placebo relapse within 9 months
- Maintenance antipsychotic medication
following an acute episode is effective
in reducing the risk of relapse
- However, some patients
recover from acute phases
without medication
- Theoretical rationale
- Family Interventions
- Strong evidence for
relapse reduction
- Strong evidence for
relapse reduction
- CBT for psychosis
- Can improve symptoms persisting
despite antipsychotic use and
possibly other challenges of
adaptation
- Can improve symptoms persisting
despite antipsychotic use and
possibly other challenges of
adaptation
- Social Skills Training
- Improves skills, but generalisation
to everyday life is difficult
- Improves skills, but generalisation
to everyday life is difficult
- Supported
Employment and
similar programs
- ‘Antipsychotic’ medications
- Symptom focussed interventions
- Three types of symptom
interventions for hallucinations
and delusions
- 1. Coping Enhancement:
builds on the person’s
‘natural’ ways of coping
- Natural’ ways of coping
with hallucinations and
delusions
- Natural’ ways of coping
with hallucinations and
delusions
- 2. ‘Information Processing’ techniques:
theoretically- derived ways of avoiding or
inhibiting the symptoms
- Vocalisation and subvocalisation
- Vocalisation and subvocalisation
- 3. Cognitive Therapy interventions:changing
appraisals or beliefs to reduce distress and
undermine the power of the symptom
- Identifies irrational (erroneous) beliefs and thoughts
that lead to distress and disruption in the person’s life
- Belief Modification techniques
- 1. ‘Analysis of evidence’ technique
- Elicit evidence given for the delusion; explore
alternative explanations for this evidence rather
than the delusion itself
- Elicit evidence given for the delusion; explore
alternative explanations for this evidence rather
than the delusion itself
- 2. Challenging belief
inconsistencies technique
- Gentle raising of doubts by noting
inconsistencies within the delusional
system, or between delusional beliefs and
other beliefs
- Gentle raising of doubts by noting
inconsistencies within the delusional
system, or between delusional beliefs and
other beliefs
- 3. Reality test technique
- Jointly construct a test that will prove
the delusion to be true or false to the
client’s satisfaction
- Jointly construct a test that will prove
the delusion to be true or false to the
client’s satisfaction
- 1. ‘Analysis of evidence’ technique
- Identifies irrational (erroneous) beliefs and thoughts
that lead to distress and disruption in the person’s life
- 1. Coping Enhancement:
builds on the person’s
‘natural’ ways of coping
- Three types of symptom
interventions for hallucinations
and delusions
- Is symptom reduction or
elimination all that is needed in
treatment of psychosis?
- Person-focused intervention
- Recovery Therapy
- 1. Engagement and assessment - Flexible
and unhurried getting to know you, and
goal setting
- 2. Everyday coping and problem solving
practical ways of coping with smaller
problems or symptom distress
- 3. Working with hallucinations and delusions - symptom
control, coping, belief modification, prevention
- 4. Learning about psychosis -
developing a more adaptive ‘story’ of
what has happened
- 5. Strengthening adaptive views of self
- rediscovering, extending and building
a positive sense of self
- 6. Addressing personal issues and emotional disturbance
impeding adaptation Includes: - concurrent disorders
(substance use, social phobia) - pre-existing developmental
issues such as sexuality - trauma and grief of psychosis
- 7. Practical relapse prevention -early signs
identification, preferably including a
significant other
- 8. Family and social re-integration -includes
facilitating a low EE environment -support and
facilitation of social roles
- 9. Completion and follow-up
- 1. Engagement and assessment - Flexible
and unhurried getting to know you, and
goal setting
- Recovery Therapy
- Person-focused intervention
- Relapse Prevention
- Rationale for Relapse Prevention
- A vulnerability-stress-coping
model of disorder suggests that
- the experience of a disorder may be episodic, depending on
relative levels of stress and coping.
- Interventions to reduce stressors, or boost
coping may prevent or forestall further episodes.
- the experience of a disorder may be episodic, depending on
relative levels of stress and coping.
- A vulnerability-stress-coping
model of disorder suggests that
- Doesn’t ordinary treatment prevent relapses?
- Yes - Good ‘bio-psycho-social’ management goes beyond acute treatment ...
- It may: reduce exposure to vulnerability via medication; reduce impact
of stressors via extra supports; enhance coping, etc. These should
reduce the likelihood of further episodes Relapse prevention via
monitoring for early warning signs ̶ Interventions to reduce stressors,
or boost coping may prevent or forestall further episodes. ...This is
“tertiary prevention”.
- It may: reduce exposure to vulnerability via medication; reduce impact
of stressors via extra supports; enhance coping, etc. These should
reduce the likelihood of further episodes Relapse prevention via
monitoring for early warning signs ̶ Interventions to reduce stressors,
or boost coping may prevent or forestall further episodes. ...This is
“tertiary prevention”.
- “Relapse prevention” programs are more specific.
- They target at-risk sub-groups (selective prevention) or
focus on early warning signs of relapse (indicated
prevention) and They include specific additional
assessment and interventions
- They target at-risk sub-groups (selective prevention) or
focus on early warning signs of relapse (indicated
prevention) and They include specific additional
assessment and interventions
- Yes - Good ‘bio-psycho-social’ management goes beyond acute treatment ...
- Necessary conditions for relapse prevention using early warning signs
- 1. ‘Early warning signs’ of relapse need to exist
- 2. Early warning signs must appear early enough to
be detected and acted upon before relapse
- 3. Realistic and reliable methods for detecting
early warning signs must be available
- 4. Consumers, families, case managers & doctors
must be prepared to commit to an action plan that is
activated by emergence of early warning signs
- 5. Interventions need to delay or prevent relapse
- 1. ‘Early warning signs’ of relapse need to exist
- Early warning signs procedure
- Establish relapse signature using observations
from both patient and others (e.g., family)
- Agree on intervention plan, e.g. ̶ ̶ reduce stress (remove,
medicate) restore coping (re-institute coping actions, boost
supports) treat emerging symptoms (medication, CBT)
- Agree on monitoring method -- Observer and or patient
questionaires, active monitoring by case working
- Establish relapse signature using observations
from both patient and others (e.g., family)
- CBT interventions in the relapse prodrome period
- Key idea: cognitions may accelerate relapse
- Negative appraisals of prodromal symptoms “I’m noticing the
voices more often – I’m going crazy again” Traumatic memories
“It was awful going to hospital”
- Interventions
- Normalise misinterpretations, reduce
catastrophisation, Address key negative beliefs, Boost
coping strategies for distress, & prodromal intrusions
- Normalise misinterpretations, reduce
catastrophisation, Address key negative beliefs, Boost
coping strategies for distress, & prodromal intrusions
- Interventions
- Negative appraisals of prodromal symptoms “I’m noticing the
voices more often – I’m going crazy again” Traumatic memories
“It was awful going to hospital”
- Key idea: cognitions may accelerate relapse
- Relapse
- A full or partial re-emergence of acute episode
symptoms following a period of full or partial recovery
- A full or partial re-emergence of acute episode
symptoms following a period of full or partial recovery
- Rationale for Relapse Prevention
- Family burden
- The impact of bizarre and unpredictable behaviour
- Stigmatisation by friends and the community
- Perceived blame from professionals
- Loss of former personality and expected futures of the ill relative
- Financial impact (less income,costs of support
- Restrictions on own lives due to caring role
- The impact of bizarre and unpredictable behaviour
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.