1952594
Beschreibung
Karteikarten von Meghan Childs, aktualisiert more than 1 year ago
|
|
Erstellt von Meghan Childs
vor fast 10 Jahre
|
|
| Frage | Antworten |
| What characteristics of a drug affect absorption? | a. Size of the drug b. Lipid solubility of drug c. Degree of ionization of the drug d. Effect of pH of gut and intestines- influenced by other drugs and food e. food in stomach or gut f. GI blood flow |
| Where are CYP450 enzymes found? | Intestinal mucosa, liver, kidney, placenta, lung, plasma |
| Which CYP450 enzymes metabolizes 50% of prescribed drugs? | 3A4 |
| How does induction of CYP450 enzymes affect the bioavailability of a drug? | Decreases it- CYP450 enzymes digest a drug, decreases the amount available for the body to use. |
| What is the function of P-glycoprotein? | barrier function- acts to expel drugs, decreasing bioavailability. |
| What is the absorption factor of IV drug? | 100% or AF=1 |
| Where does a PO drug go after being absorbed from the stomach? | Portal vein to the liver |
| What is "first pass" metabolism? | The portion of the drug that is eliminated by hepatic metabolism. Never seen in systemic circulation. |
| What affects first pass metabolism? | a. First phase (P450) and second phase (conjugation) b. Lipid solubility c. Hepatic blood flow |
| How can you minimize/avoid the first pass effect? | Administer via different routes- sublingual, transdermal, rectal |
| What are the possible outcomes of first pass metabolism? | 1) Active<--> Inactive 2) Toxic <--> Non-toxic 3) Lipid-soluble --> Water soluble (polarized) |
| Phase I reactions involve______ and ________ type reactions | CYP450 enzymes/ oxidation-reduction reactions |
| What factors affect distribution? | • Blood flow to location of SOA • Water solubility, lipid solubility • Plasma protein binding • Special membranes and transport proteins • Drug reservoirs |
| What affects glomerular filtration rate? | Age, renal disease, protein-binding, hypertension, atherosclerosis, diabetes impaired renal function |
| Define tubular secretion | Movement from plasma to lumen of nephron |
| What are two important concepts for understanding tubular secretion? | (1) Saturability (2) Competitive inhibition |
| Define tubular reabsorption | Drugs move from lumen of nephron to plasma |
| What affects tubular reabsorption? | (1) Unionized versus drugs (2) Transport proteins |
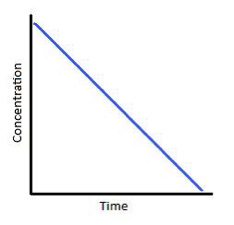
| Define first order kinetics | Constant fraction of the drug is eliminate over time. |
| How many half-lives to essentially eliminate a drug? | 5 |
| How many doses to reach steady state? | 5 |
| Define zero order kinetics | The amount of drug eliminated per unit time is the same. |
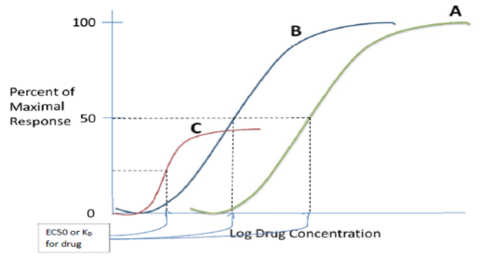
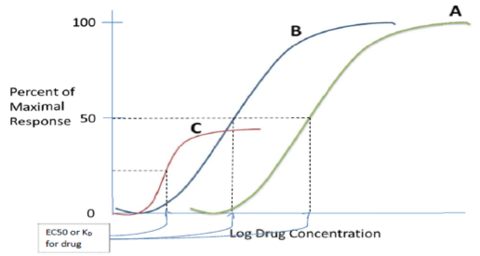
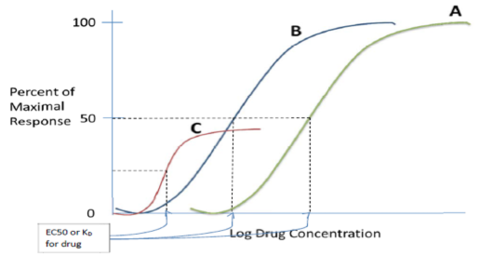
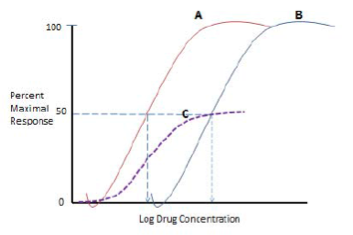
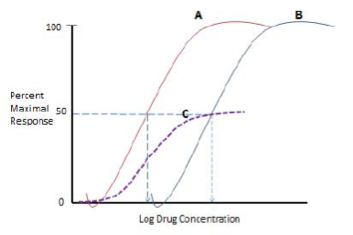
| Define EC50 | Drug concentration with half maximal response (half receptors bound). |
| Define Kd | The equilibrium constant- Koff/Kon, half receptors are bound |
| How is Kd related to affinity? | Inversely- Kd=1/affinity |
| Which curve shows a more potent drug? | C- the EC50 (concentration at half maximal response) is the lowest |
| Which is more potent? Drug A or B? | B- half maximal response occurs at a lower concentration |
| Which drug has the lowest efficacy? | C- the drug produces the lowest maximal effect |
| Which curve shows Drug A in the presence of a non-competitive antagonist? | C- the drug can never achieve the same maximal possible effect because the receptor sites are irreversibly blocked. |
| Which curves shows Drug A in the presence of a competitive antagonist? | B- drug can achieve the same maximal response, but require a greater concentration of the drug. |
| Define ED50 | Dose at which 50% of the subjects respond |
| Therapeutic index= | TI=LD50/ED50 |
| Define additive effect | 1+1=2 |
| Define synergistic effect | 1+1>>2 |
| Define tachyphylaxis | Diminished response to a drug that happens quickly |
| Define down-regulation | Decrease in receptors due to internalization, typically in response to prolonged exposure |
| Define tolerance | Diminished response to a drug, takes longer to develop |
| Define dependence | When the drug is withdrawn, patient will have withdrawal symptoms |
| Gastric pH changes: Premature infants ________ Full term babies___________ | • Premature babies do not produce gastric acid • Full term- at birth it is neutral, then decreases in the first 24 hours to pH 1-3 |
| In neonates: Bile formation _____ Pancreatic enzyme production_____ Gastric emptying____ Intestinal motility____ Bowel length____ Effective absorptive surface ____ | all decreased |
| Infants have a higher volume of distribution for _____-soluble drugs and a lower volume of distribution for _______-soluble drugs | water/fat |
| Blood brain barrier is more/less permeable in neonates | more |
| Neonates have more/less plasma binding proteins and more/less bilirubin, which competes for plasma binding proteins. | Neonates have less plasma binding proteins and more bilirubin, which competes for plasma binding proteins. |
| Generally infants have increased/reduced hepatic blood flow and increased/reduced Phase I metabolism. | Generally infants have reduced hepatic blood flow and reduced Phase I metabolism. |
| Infants have decreased/increased glomerular filtration compared to adults. | Infants have decreased glomerular filtration compared to adults. Reaches adult function 6 months-1 year. |
| Rates of tubular secretion and renal reabsorption are generally lower/higher in pediatrics, especially neonates and young infants. | Rates of tubular secretion and renal reabsorption are generally lower in pediatrics, especially neonates and young infants. |
| Overall lower/higher rates of elimination in peds lead to increased/decreased response to the drug. | Overall lower rates of elimination in peds lead to increased response to the drug |
| Oral absorption in pregnancy: o Gastric emptying/intestinal motility? o Gastric pH? o CO? affects absorption/metabolism? | o Delayed gastric emptying and reduced intestinal motility o Increased gastric pH o Large increase in CO, may increase rate of absorption o Nausea and vomiting o First pass- increased CO to liver, variable alterations in metabolism |
| Inhalation absorption is ______ in pregnancy due to ______CO and _______ tidal volume. | Inhalation absorption is increased in pregnancy due to increased CO and increased tidal volume. |
| IM absorption in pregnancy is ______ due to _______ blood flow to muscles. | IM absorption in pregnancy is decreased due to decreased blood flow to muscles. |
| Plasma volume is _____ during pregnancy, leading to _____ plasma drug concentration. | Plasma volume is increased by 50% during pregnancy, leading to decreased plasma drug concentration. |
| Pregnancy is a state of ____ albuminemia. Hormones cause ______ protein binding. | Pregnancy is a state of hypoalbuminemia. Hormones cause decreased protein binding. |
| Drug metabolism in pregnancy is _____ due to ______ hepatic blood flow and _______ CYP450 enzyme activity. | Drug metabolism in pregnancy is increased due to increased hepatic blood flow and increased CYP450 enzyme activity. |
| Excretion in pregnancy is ________. | Excretion in pregnancy is increased. |
| Characteristics of drugs that are easily transported through the placenta: lipo/hydrophilic? high/low molecular weight? bound/unbound? long/short half-life? ionized/unionized? | Characteristics of drugs that are easily transported through the placenta: lipophilic low molecular weight unbound long half-life unionized |
| Pregnancy Category A | adequate and well-controlled trials have failed to demonstrate a risk to the fetus |
| Pregnancy Category B | animal reproduction studies failed to demonstrate risk, but there are no studies in pregnant women |
| Pregnancy Category C | animal reproduction studies have shown an adverse effect on fetus, there are no adequate and well-controlled studies in humans |
| Pregnancy Category D | positive evidence of fetal risk based ; but potential benefits may outweigh potential risks |
| Pregnancy Category X | studies in animals and/or humans have demonstrated fetal abnormalities; risks clearly outweigh the benefits |
| Phase II metabolism involves what type of reaction? | Conjugation but also alkylation, acetylation, methylation |
| Define side effect | Nearly unavoidable secondary drug effects produced at therapeutic doses. Generally predictable and dose-dependent. |
| Define adverse event | undesirable experience associated with the use of a medical product |
| What are Type A drug reactions? | intrinsic, dose-dependent, ADR is an extension of the normal (therapeutic) pharmacologiacal effects of the drug |
| What are Type B drug reactions? | Idiosyncratic, immune-mediated, can occur at very low doses NOT dose dependent, result in greater morbidity and mortality |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.