346085
Beschreibung
Karteikarten von Joanna Elliott, aktualisiert more than 1 year ago
|
|
Erstellt von Joanna Elliott
vor etwa 11 Jahre
|
|
| Frage | Antworten |
| What are the 4 different ways in which a Doctor can examine a patient | Inspection (look), Palpation(feel), Ascultation (hear) & Percussion (tap to elicit sound) |
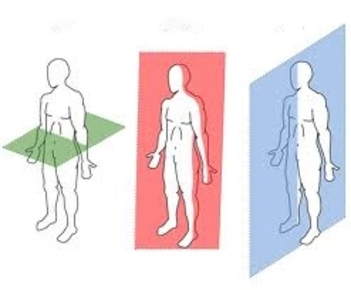
| Describe the anatomical position | Upright facing forward, palms facing forward and feet together |
| What is the Supine position, and what is the Prone position | Laying on your back = Supine, Laying on your front = Prone |
|
Image:
download (image/jpg)
|
(From left to right) - Transverse plane, Frontal/Coronal plane, Midsagittal plane |
| The Heart is _ in relation to the Ovaries | Superior |
| Which definitions are used to describe 'towards the front' and 'towards the back' | Anterior and Posterior |
| What are 'Superior' and 'Inferior' used to describe | Superior = towards the head, Inferior = towards the legs/away from the head |
| Which definitions are used to describe the position of something in relation to the midline | Medial & Lateral |
| If something is Superficial it is ... | Towards the surface |
| What definitions are used to describe things in relation to the Origin | Proximal & Distal |
| Name 5 functions of the skin | Protection, Containment, Heat regulation, Sensation, Synthesis and Storage of Vitamin D |
| Which layer of the skin has no blood supply, the Epidermis or the Dermis | The Epidermis doesn't have it's own blood supply |
| What type of tissue is the Epidermis | Epithelial tissue: Keratinised Stratified Squamous Epithelium |
| What are the 2 types of Epithelial tissue and what is the differences between them | Stratified & Simple. Stratified has more than one layer of cells, Simple has only one layer of cells |
| What are the 4 layers of the Epidermis, starting from the top and going down | Stratum Corneum, Stratum Granulosum, Stratum Spinosum, Stratum basale |
| Which layer of the Epidermis is made up of 20 - 35 layers of Dead keratinocytes | Stratum Corneum |
| What does the Stratum Granulosum contain | 3 - 5 layers of Flattened keratinocytes which are beginning to lose their nuclei and die. Also contains lamellar granules, which are full of lipids. |
| Which layer is found only in thick skin? | Stratum Lucidum |
| Which layer contains 8 - 10 layers of Polyhedral keratinocytes with a limited ability to divide | Stratum Spinosum |
| What are cells in the Stratum Spinosum joined together by | Desmosomes |
| What does the Stratum Basale layer contain | A single layer of keratinocytes which are actively dividing, as well as melanocytes |
| Which stains can be used to reveal the extra layer in thick skin | Haemotoxylin & Eosin stains |
| What does the Stratum Lucidum contain large amounts of | Keratin |
| Other than the Stratum Lucidum, what else is different about think skin compared to thin skin | In thick skin the stratum corneum is thicker |
| What happens as you move from the Stratum Basale to the Stratum Corneum, and how long does this process take. | Capacity of keratinocytes to divide decreases. Desmosomes form and attach neighbouring cells together. More keratin aggregates and the type of Keratin changes. Keratinocytes lose their nuclei and die. Extacellular lipids bind cells together. Corenocytes ar shed. This process takes 28 days. |
| What is Psoriasis | A condition where the epidermal shedding cycle shortens, so cells accumulate and form scabs on the skin. There is 'increased epidermal turnover' |
| What is found in the stratum corneum when someone has Psoriasis, and what is this called | Cell nuclei is found in the Stratum Corenum. This is called Parakeratosis. |
| Where does Melanin synthesis take place | In Melanosomes, which are taken up by Keratinocytes and form caps over them, protecting them from UV |
| Where are Melanocytes found | Stratum Basale |
| What are differences in skin colour due to | Number of melanosomes. Type of melanin. The proportion of red/black melanin. |
| Which amino acid residue is involved in the formation of red/black melanin | Tyrosine |
| Name 3 types of tumourous cancers and what they are caused by | Malignant Melanoma, caused by abnormal proliferation of melanocytes. Squamous Cell Carcinoma caused by abnormal proliferation of Keratinocytes. Basal Cell Carcinoma caused by abnormal proliferation of basal cells. |
| What is a Merkel cell and where is it found | It's an endocrine cell found in the lower part of the epidermis |
| What is a Langerhan cell and where is it found | It is an APC which binds antigens entering through the skin and transports them to te lymph nodes. Found in the Epidermis |
| What is Bullous Pemphigold | When there is liquid between the Epidermis and the Dermis due to an immune reaction. Causes Blisters. |
| What is the Dermis-Epidermis junction called | Hemidesmosome |
| What is the function of the Dermis and what does it produce | Provides strength, elasticity, nutrition to the Epidermis, and produces collagen. |
| Name 2 differences between the Dermis and Epidermis | The Dermis is Vascular, the Epidermis is not. The Dermis is thicker than the Epidermis. |
| What is the main cell type in the Dermis | Fibroblast |
| Name the 2 regions of the Dermis | Papillary & Reticular |
| Name the appendages of the Dermis and their functions (if applicable) | Hair. Subaceous gland, secrets Sebum. Arrector pili muscle, contracts to make hairs stand up. Sweat glands called Eccrine and Apocrine. Nerve endings. Lymphatics. Blood vessels. |
| What's the difference between the Eccrine gland and the Apocrine gland | Eccrine gland is more superficial and secretes a more watery odourless substance. Apocrine secretes a thicker substance with an odour, and only starts working during puberty. |
| What is Fascia and what is it's function | Packing material beneath the skin. Insulation. |
| Name the 2 types of Fascia and their functions if applicable. | Subcutaneous tissue and Deep fascia. Deep fascia is a connective tissue with extensions to bones , forming compartments in the arm, restricting infections and tumour spreads |
| What is the downside of Deep fascia | Restricts compartment space in the in muscles |
| Are muscles always attached to bones? | No. They can be attached to skin, deep fascia etc |
| Name the 3 types of muscle | Smooth. Cardiac. Striated. |
| Name 3 functions of Muscle | Movement. Producing heat. Regulating organ volume. |
| What is the connective tissue covering | Fasicle |
| Which type of muscles have an origin and insertion | Skeletal |
| ABduction | Movement AWAY from the midline |
| ADduction | Movement TOWARDS the midline |
| Medial Rotation | Rotation around the long axis towards the midline aka lowering your arm |
| Lateral Rotation | Rotation around the long axis away from the midline, aka Raising your arm |
| Pronation | Moving palm from Anterior facing to Posterior facing |
| What would standing on tiptoes be known as | Plantar Flexion |
| What pointing your toes upward be known as | Dorsiflexion |
| Circumduction | Circular movement |
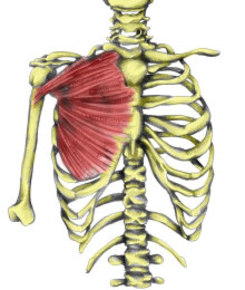
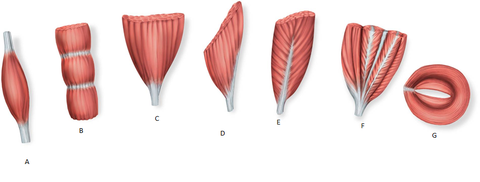
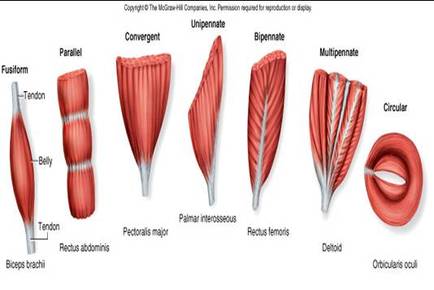
| Name all the types of Muscle | Bipennate. Convergant. Circular. Multipennate. Fusiform. Unipennate. Parallel. |
|
Image:
pec_major (image/jpg)
|
Convergent |
| Tonic contraction | Involuntary |
| Isometric | No movement |
| Concentric | Shortening |
| Eccentric | Lengthening |
| Prime mover | Muscle agonist |
| Antagonist | Initiates opposite action to the agonist |
| Synergist | Helps the Prime Mover |
| Fixator | Stabalises the Origin of the Prime Mover |
| What initiates movement | An action potential in a nerve |
| Motor Unit Recruitment | As strength of contraction increases, more motor neurons are fired |
| Which motor units are used for which movements. | Precise movements use Small motor units. Powerful movements that don't need much precision use Large motor units. |
| Musculcutaneous Nerve | Supplies biceps. If damaged = paralysis |
| What is the difference between Healing in the Epidermis and Healing in the Dermis | Epidermis = can regenerate, no scarring. Dermis = Connective tissue is damaged, scarring occurs and leads to Fibrosis. |
| Fibrosis | Disorganised laying of collagen. Caused my tissue scarring. |
| Satellite cells | Can act like stem cells to generate muscle cells, but have a limited capacity to divide |
| Muscle Pathology | Response to injury is to change the size of muscle cells by decreasing or increasing their size |
| Hypertrophy | Increase in size |
| Atrophy | Decrease in size |
| Hyperplasia | Increase in number of cells |
| Nerve pathology | Leads to loss of muscle movement and atrophy over time |
| Bell's Palsy | Temporary paralysis of one side of the face due to stroke or viral damage. Affects the facial nerve that supplies the muscles of the face. |
| Myasthenia gravis | Autoimmune condition which affects acetylcholine receptors. |
| Duchene Muscular Dystrophy | Is a genetic, recessive, condition. Dystrophin gene, an essential part of muscle, is mutated. Affects large muscles first. |
| What 3 layers do both arteries and veins have | Tunica: Externa, Media & Intima |
| Which layer do the Capillaries have | Only Tunica Intima |
| Arteries vs Veins | Arteries have thick walls, Veins have thin walls. Arteries have elastin and collagen, Veins don't. Arteries have a narrow Lumen, Veins have a wide lumen. Veins have valves, Arteries don't. |
| Does Cardiac muscle have satellite cells | No |
| What are Conducting Vessels, which is the thickest layer, and give an example | Large arteries that come directly from the Heart. Tunica Media is the thickest layer and is made up of elastic fibres. Eg Aorta |
| Distributing Vessels | Can be End Arteries or can form Anastomosis (the connection of 2 structures). Tunica Media is made up of Smooth Muscle. |
| Arteriole | Small artery. Resistance vessel. Regulates blood flow into the Capillaries. |
| Where do Veins end up | Superior or Inferior Vena Cava |
| What regulates the flow from Arterioles in Capillaries | Precapillary Sphincters |
| Capillaries are fenestrated - what does this mean | They contain pores |
| What are the major divisions of the Aorta from the thorax downwards | Aortic arch - Ascending Thoracic aorta - Descending Thoracic aorta - Superior Mesentric - Abdominal aorta - Inferior Mesentric - Common Illiac Artery |
| What is the Portal Venus System responsible for, and what else is it known as | Also known as the Hepatic Portal Circulation, it is responsible for directing blood from the GI tract into the liver before sending it back to the heart |
| Which veins lead into the Hepatic Portal Vein | Superior Mesentric Vein & Splenic Vein |
| Which 2 vessels lead into the Liver | Hepatic Portal vein + Proper Hepatic Artery |
| Which part of the aorta leads into the Proper Hepatic Artery | Abdominal Aorta |
| Which vessel does the Liver deliver blood to | Hepatic Vein, which then delivers the blood to the inferior/superior Vena Cava |
| In limbs what 2 sets of veins are there, and which is more predominant in the Lower limbs | Superficial and Deep set, with Deep set being more predominant in the lower limbs |
| What is the skeleton made up of | Bone and cartilage |
| What the 2 components of the skeleton and what do they include | The main trunk is called the Axial skeleton, and includes the Head, Vertebra, Ribs and Sterbum. The Appendicular skeleton includes the bones of the upper and lower limbs and the girdles that connect them |
| What is bone made up of, and what makes it flexible | Specialised connective tissue and Collagen. Collagen is what determines flexability. |
| What are the functions of the bone | Support. Protection of internal organs. Leverage for motion. Mineral homeostasis. Blood cell production. Triglyceride storage. |
| Difference between children and adults | In children blood cells are produced by all bones, in adults they are only produced by certain bones eg ribs, hip bone, sternum & vertebra |
| What are the different shapes of bones | Long, Flat, Short, Irregular, Sesamoid |
| Example of a Sesamoid bone | Patella (kneecap) A sesamoid is any bone within a joint |
| Example of a Long bone | Humerous(leg), Femur(arm) |
| Example of Flat bone | Sternum |
| Example of an Irregular bone | Vertebra |
| Example of a Short bone | Wrist bone |
| Name the components of a long bone | Epiphysis (ends), Metaphysis (connects ends and shaft), Diaphysis (shaft, more liable to breaks), Cancellous bone (spongy), Compact bone (lines the outside of the shaft) |
| Name the 2 bone coverings and what they provide | Endosteum (inner lining) & the periosteum (outer lining, provides bone with nutrition and blood supply) |
| What arteries supply the Long bone with blood | Epiphyseal, Metaphyseal, Periosteal (supplies periosteum and compact bone) & Nutrient artery (supplies the medullary cavity, spongy bone, and deeper parts of the compact bone) |
| 3 Bone cells | Osteoblasts (build bone) --> Osteocytes (maintain bone) -->Osteoclasts (breaks down bone) |
| Calcification | Initiated by OsteoBlasts. Mineral salts are deposited and crystalise in a collagen fibre framework |
| The digestion of bone by osteoclasts followed by bone formation by osteoblasts is known as what? And how long does this process take | Bone remodelling. Takes 2 months. |
| Which bone is remodelled every 4 months | Distal part of the femur |
| What does calcium do to bone | Hardens it |
| What does Vitamin D do to bone | Increases absorption of Ca2+ |
| Which Vitamin is needed for collagen synthesis in bone | Vitamin C |
| Which 3 things increase the activity of osteoblasts | Estrogen (inhibits bone resorption by osteoclasts), Vitamin A and Thyroxyine |
| Which hormone increases the activity of osteoclasts | Parathyroid hormone |
| What is a repeated unit of compact bone called | Osteon (aka Haversian system) |
| What does an Osteon consist of | Central canal, Blood vessels in the central canal, Concentric lamella, Osteocytes with lacunae, canalicul(which contains the processes of osteoCytes) |
| Which types of bones contain spongy bone | Long, short & flat (both are predominately spongy bone), irregular |
| What does spongy bone contain | Trabeculae, with spaces inbetween them containing bone marrow |
| What is the process of bone formation known as. When does it begin and end. | Ossification. Starts after 6 weeks of fetal life and ends around 23/25 |
| Mesenchyme | Fetal connective tissue |
| Intramembranous ossification | Bone cells develop on mesenchyme and lay down bone |
| Endochondral Ossification | Catilage model. Invasion of blood vessels. 1. Primary ossification centre. Formation of bone collar around Hyaline cartilage model. 2. The hyaline cartilage deteriorates. 3. Invasion of internal cavities by the Periosteal bud. Some cells become osteocytes. Spongy bone formation. 4. Bone is destroyed to form the medullary cavity. Appearence of the Secondary ossification centre in the Epiphyses. 5. Ossification of the epiphysis. Hyaline cartilage remains only in the epipyseal plates and Articular Cartilages/ |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.