5291227
| Frage | Antworten |
| What is apoptosis important for? | Removal of damaged cells |
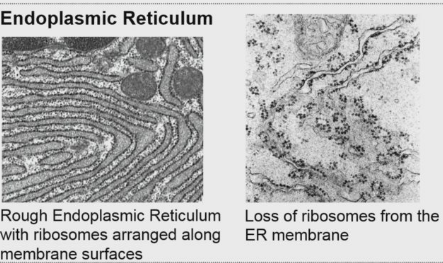
| What are the morphological changes in cells undergoing necrosis? What is the cut off for reversibility? | 1) Cytoplasmic swelling - either due to free radical damage or because ATP pumps stop working allowing water to enter cell. 2) Dilation of endoplasmic reticulum due to stress of cytoplasmic swelling 3) Ribosomes drop of ER due to its swelling - loss of protein production at ER (cells need to proteins to survive) UP TO THIS POINT CHANGES ARE REVERSIBLE if environmental stress is removed 4) Mitochondrial dilation |
| What is the endoplasmic reticulum? | Interconnected membranous sacs which also connect to nuclear envelope. If it has ribosomes = rough endoplasmic reticulum, no ribosomes = smooth endoplasmic reticulum. Ribosomes produce proteins - can happen freely in cytosol but often in ER where proteins are packaged and directed. |
| X | |
| What are mitochondria? What does it have to maintain? | 1) Double membraned organelle. Membrane is organised in christae. Enzymes of the respiratory chain are arranged along the surface of christae. Site of ATP production. 2) Proton gradient across INNER MEMBRANE - proton and O2 are final electron donors resulting in production of H20 and ATP |
| What happens when the mitochondria starts to swell? | Mitochondrial permeabilization transition pore forms in membrane - non specific pore, allows water and ions to flow into mitochondria. Water causes further swelling. Contents of mitochondria leave, loss of proton gradient results in inability to produce ATP. |
| What are the results of mitochondrial swelling? | 1) Detachment of respiratory chain enzymes from the inner membrane into the lumen forming 'matrix densities'. 2) Ca2+ release through pore - increase in Ca2+ concentration stressed nearby mitochondria causing more pore formation - domino effect. NOT REVERSIBLE, TERMINAL NECROSIS. |
| What are the final stages of cell death? | No. free radicals increases as dying cells are no longer able to neutralise them (eg in ATP production. Free radical mediated oxidative injury is the final common pathway in cell death from adverse external events. |
| What are free radicals? What are the most important ones in the biological systems? What are their half lives? | 1) Atoms or molecules with unpaired electrons, are extremely reactive 2) OH- (hydroxyl radical) and O2- (superoxide radical) 3) One nano second |
| What is a reperfusion injury? | 1) Refers to re-entry of oxygen to ischaemic tissue - ie following myocardial infarction try to recover ischaemic damaged tissue by reperfusion of O2. Reoxygenation of tissue causes as much damage as the initial ischaemia. |
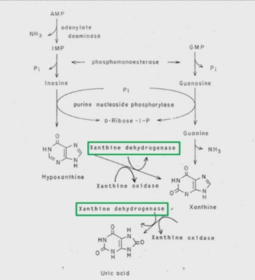
| What causes reperfusion injury? | Xanthine dehydrogenase (enzyme) results in increased production of free radicals - reactive oxygen intermediates (ROI) produced during reoxygenation |
| What is the function of xanthine dehydrogenase? | Catalyses one of the steps of the catabolism of purine - ATP and GTP |
| What is ATP (ADP + AMP) converted into? What is this then converted into and by what? | 1) Hypoxanthine 2) Xanthine by xanthine dehydrogenase |
| What is GTP (GDP + GMP) converted into? | Xanthine |
| What is xanthine converted into? By what? | 1) Uric acid 2) Xanthine dehydrogenase |
| X | |
| What happens to xanthine dehydrogenase when cellular O2 is low? | Converted into xanthine oxidase. |
| What does xanthine dehydrogenase use as its coenzyme? What does this lead to the production of? How is this dealt with? | 1) NADH 2) H+ 3) Fed into ATP respiratory chain |
| How does xanthine oxidase differ from xanthine dehydrogenase? | 1) Same processes ie uric acid production 2) Uses O2 as coenzyme |
| Concerning xanthine what happens during hypoxia? | 1) Xanthine dehydrogenase converted to oxidase 2) Xanthine oxidase cannot function properly due to lack of O2 resulting in buildup of xanthine (can't be broken down into uric acid). Also more ATP is being metabolised in low oxygen conditions increasing xanthine production. |
| What happens when O2 is then returned to ischaemic tissue? | Xanthine oxidase has substrate (O2) available - can convert xanthine to uric acid. Use of O2 as cofactor results in reactive oxygen intermediates (ROI) as byproducts. Free radicals then destroy anything they come into contact with. |
| What are crucial areas which are particularly damaged by free radicals? (3) | 1) Lipids - targets C=C in cell membranes, compromises boundary function allowing ions and water to enter 2) Proteins - cause S=S (disulphide bonds) to form between polypeptide chains, protein loss of function and may also become reactive in their own right - need to be destroyed 3) DNA - single strand breaks at Thymine residues. Damage may be so great that repair isn't possible, cell has to be destroyed. |
| What might be used to treat reperfusion injury? What is the possible drawback of this? | Allopurinol which can block xanthine oxidase - only works half the time. |
| What is apoptosis? When are you likely to see this? Why is this important? | 1) Programmed cell death 2) When damage has been slow and gradual 3) Damaged cells are nonfunctional and also may lead to tumour growth |
| Give two examples of environmental triggers which would result in apoptosis? | 1) UV damage to DNA 2) Accumulation of heavy metals in cell |
| How does apoptosis differ from necrosis in terms of number of cell affected? | Necrosis tends to be widespread whereas apoptosis often just removes one cell |
| Aside from dealing with damage what is apoptotic cell death important for? | Integral part of normal tissue development and management. |
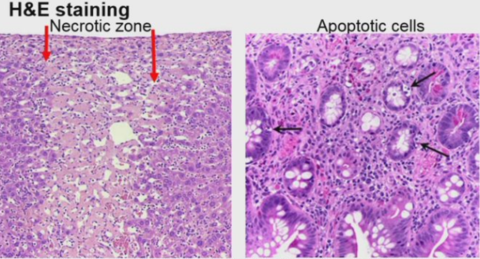
| What are the key differences in cellular morphology between apoptotic and necrotic cell death? | Necrotic cells appear to stay in tissue but architecture has been completely destroyed and is therefore no longer function - cell contents leak into surrounding ECM and trigger inflammatory response. Apoptosis is much harder to see - single cell death but surrounding tissue is fine and continues to function. No infiltration of immune system. |
| X | |
| Compare between apoptosis and necrosis: 1) Histology | A: Single cells affected within living tissue Tissue structure unaffected N: Sheets of cells dying together Tissue architecture is disrupted |
| 2) Cell cytology | A: Cells contract Increased density of cytoplasm and nucleus N: Cell swell (oedema) Loss of intracellular features |
| 3) Ultrastructure | A: Cells pull away from neighbouring cells Plasmas membrane and mitochondria remain intact. N: Plasma membrane and internal membranes ruptured Mitochondria swell |
| 4) Circumstances | A: 'Programmed death' often desirable N: Never physiological |
| 5) Effects in tissue | A: No inflammation Rapid removal of dead cell leaving tissue architecture undisturbed N: Evokes an acute inflammatory reaction Major disturbance of surrounding tissue |
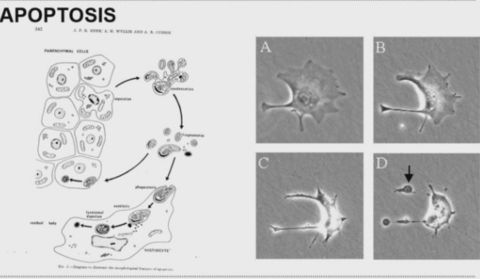
| 1) Cell loses contact 2) Cell contracts but membrane is intact 3) Cell can fragment into apoptotic bodies 4) Fragments taken up by tissue or macrophages in ECM | |
| When is apoptosis needed in development? | DEVELOPMENT 1) Organogenesis (ie during embryonic stages) - Deletion of interdigital webbs - Lumen of formation in hollow organs - Neuronal development 2) Metamorphosis - amphibians |
| How can you visualise apoptosis? | 1) Mark cells with eGFP etc 2) Histologically - stain cells undergoing apoptosis |
| Why is apoptosis important in neurogenesis? | Often too many neurons produced - target cells produce survival factor but only enough to provide the correct number of neurons with a sufficient amount ie one target neuron to one target cell. Uneccessary cells die by apoptosis. |
| Why is apoptosis favourable over necrosis? | 1) Much cleaner way of removing unwanted cells - not other tissue damage. 2) Can recycle material |
| When is apoptosis useful in adults? | Removal of damage or no longer wanted tissue 1) Endocrine tissue - removal of trophic stimuli e.g. when a child is weaned from breast milk need reduction in lactate glands - need to do it in clean way so can regenerate for second pregnancy 2) Immune system - ie used neutrophils 3) Tissue turnover |
| How many cells are lost in an adult per day? | 10 ^10 cells through apoptosis |
| What would happen if there was no tissue turnover? | Potentially tumour development - especially if cells have mutated etc. |
| What do cellular adaptations include? | Changes in cell size, number and type |
| What are the possible types of these adaptations? (6) | 1) Atrophy 2) Hypertrophy 3) Hyperplasia 4) Aplasia 5) Metaplasia 6) Dysplasia |
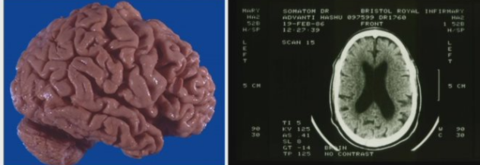
| What is atrophy? How are they deficient? How does this affect tissue? | 1) Shrinkage in size of the cell by loss of cytoplasmic substance. 2) Functionally 3) Decreases in size |
| What are 6 examples of causes of cellular atrophy? | 1) Decrease workload - ie when people stop exercising 2) Loss of innervation 3) Diminished blood supply 4) Inadequate nutrition 5) Loss of endocrine stimulation 6) Increasing age |
| Which tissue type is particularly susceptible to atrophy? | Brain tissue |
| Ventricles should be much smaller than they are if this was a healthy individual | |
| What conditions can cause brain tissue atrophy? (4) | 1) Alzheimer's 2) Huntington's 3) Diabetes due to decreased blood flow 4) Inadequate nutrition |
| Where is atrophy very physically obvious? What can cause this? (2) | Muscle 1) Loss innervation - like in carpal tunnel 2) Going to space |
| Define hypertrophy | Increase in size of cells and as a result increase in the size of tissue |
| Where is hypertrophy most usual? | Muscle - both cardiac and skeletal |
| In which type of muscle is hypertrophy bad? | Cardiac |
| What can cause cardiac hypertrophy? | If ventricles have to harder due to: 1) Hypertension - initially ok, heart is able to keep up and keep enough blood going round system even if this results in high blood pressure 2) Valve disease |
| Why is cardiac hypertrophy bad? | Musculature becomes stiff - heart can't relax enough and doesn't fill properly. Volume of blood it pumps round the body decreases despite increased tension etc. |
| How can you fix hypertrophy? | Can sometimes remove some of the excess muscle but often need to perform heart replacement. |
| When do you see cardiac hypertrophy in the left ventricle? | Due to hypotension |
| What causes cardiac hypertrophy in the right ventricle? | If disease causes decreased O2 levels in lung eg COPD. Levels of O2 are lower causing pulmonary artery to constrict and increase pressure. Right ventricle has to work harder to pump blood through pulmonary loop into lungs. |
| Define hyperplasia. Where is this seen in normal physiology? | 1) Describe the increase in number of cells in an organ or tissue. 2) When children grown |
| How does hyperplasia related to hypertrophy? What tissues does it occur in? | Parallel to hypertrophy and occurs in tissues which are capable of proliferative response to demand for increased function. |
| What are the different types of adult hyperplasia? | 1) Hormonally dependent hyperplasia - eg lactation 2) Compensatory hyperplasia - liver regeneration |
| How much of the liver has to remain in order for it regenerate to its full original size? | 25% |
| What is aplasia? | Zero growth - cells aren't dividing, cessation of proliferation in those which normally undergo continuous proliferation |
| What would you expect to see in bone marrow aplasia (aplastic aplasia)? | Would result in decreased blood cell count |
| What other organs are affected by aplasia? What are the causes of aplasia? How can this be used therapeutically? | 1) Skin - epithelium and gut 2) Lethal irradiation 3) Some toxic agents 4) Virus Try to kill cancer - chemo/radiotherapy, hope to kill fastly dividing cells |
| What are the side effects of chemotherapy? Why? | 1) Loss of neutrophils 2) Hair loss 3) Digestive issues Causing body to enter state of aplasia |
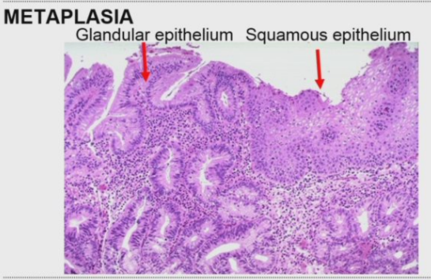
| What is metaplasia? | Reversible change in which one mature cells type is replaced by another cell type, usually as a result of a chronic irritative stimulus. |
| What is the most common type of metaplasia? Why does this happen? What does this result in? | 1) When glandular epithelia is converted to squamous epithelia due to smoking (SQUAMOUS METAPLASIA) 2) Body trying to protect itself from irritant 3) Non-functional area of bronchiole, doesn't produce mucin or CD8 T cells which would usually waft mucin out of airways. |
| What is the other type of metaplasia? What causes this? | 1) Columnar cell metaplasia of the distal oesophagus (Barrett's) 2) Chronic gastro-oesophageal reflux - continuous acid reflux results in body trying to protect the oesophagus by making it more stomach like |
| X | |
| X | |
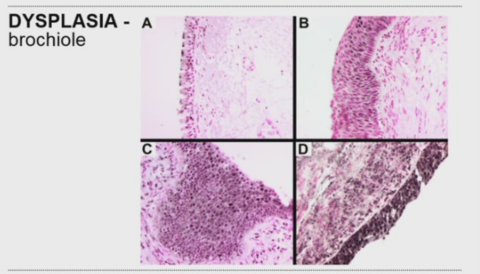
| What does dysplasia mean? | Deranged growth - can mean overgrowth and don't look like the tissue they belong to or anything else. Cells which have undergone abnormal proliferation resulting in abnormality in cell size, shape and reorganisation. |
| What often leads into dysplasia? What does dysplasia often lead to? | 1) Metaplasia 2) Carcinoma |
| A) Epithelial cells B) Cells become irritant but respond to surrounding tissue commands C) Dysplasia growth - benign but cells now don't respond to tissue eg apoptosis commands D) Carcinoma could grow from here. | |
| x |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.