5406111
Beschreibung
Karteikarten von Andrew Street, aktualisiert more than 1 year ago
|
|
Erstellt von Andrew Street
vor mehr als 8 Jahre
|
|
| Frage | Antworten |
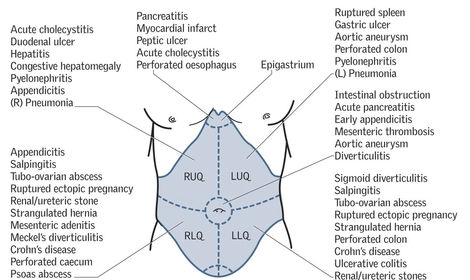
| 269 Common causes of an acute abdomen? | |
| 271 S & Sx of intestinal obstruction? | Vomiting (may be faeculent) / nausea / anorexia / colic (occurs early, may be absent in long-standing complete obstruction) / constipation (may not be absolute if obstruction is high) / distension / active tinkling bowel sounds. |
| 272 DDx for small bowel obstruction? | Adhesions, hernias. |
| 272 DDx for large bowel obstruction? | Colon CA, constipation, diverticular stricture, volvulus (sigmoid, caecal). |
| 272 DDx for rarer causes of bowel obstruction? | Crohn's stricture, gallstone ileus, intussusception, TB, foreign body. |
| 273 Describe mechanical obstruction vs ileus. | Ileus is functional obstruction from reduced bowel motility. Mechanical obstruction has a physical blockage. |
| 274 How would you Ix suspected small bowel obstruction? | FBC, ESR, CRP / AXR (may show dilated loops of bowel), CXR (look for air under the diaphragms) / electrolytes, urea, creatinine, eGFR, LFT's, calcium, amylase. |
| 275 Describe the emergency Mx of small bowel obstruction. | NG tube to empty stomach of fluid & gas / maintain hydration via IV infusion ('drip & suck') / maintain electrolyte balance / reduce opiates and encourage pt to mobilise / consider nutritional status / consider a CT for definitive Dx (ie site of obstruction). |
| 277 S & Sx of peritonitis? What should always be checked? | Prostration / shock / lying still / +ve cough test / tenderness (+/- rebound) / guarding / board like rigidity / loss of BS. Acute pancreatitis may present similarly so always check serum amylase! |
| 278 List causes of peritonitis. | Primary (rare): typically streptococcal with entry probably from BD rather than organs. / Secondary: acute perforated appendicitis (most common esp. <45 YO), acute perforated diverticular (esp. in elderly), upper GI perforation, perforated tumours, perforated ischaemic bowel, acute pancreatitis, peritoneal dialysis related, post-surgery. |
| 279 Outline the Ix and Mx of peritonitis. | Resuscitation: IV access, catheterize and fluid balance chart, BD's (FBC, U & E, CRP, amylase, group & save), ABG. / Establish a diagnosis: CT is no.1 choice, BD's may show neutrophilia & ^ CRP, ^ amylase may suggest pancreatitis, laparoscopy (occasionally used). / Early Rx = ABX's (metronidazole 500mg IV tds + cefuroxime 750mg IV tds). / Definitive MX depends on cause - usually surgery. |
| 280 S & Sx of perforation? | Esophageal, gastric, and duodenal perforation tends to manifest suddenly and catastrophically, with abrupt onset of acute abdomen with severe generalized abdominal pain, tenderness, and peritoneal signs. Pain may radiate to the shoulder. Perforation at other GI sites often occurs in the setting of other painful, inflammatory conditions. Because such perforations are often small initially and frequently walled off by the omentum, pain often develops gradually and may be localized. Tenderness is more focal. Nausea, vomiting, and anorexia are common. Bowel sounds are quiet to absent. |
| 281 List some common causes of bowel perforation. | Gastric & duodenal ulcers / appendicitis / GI CA / diverticulitis / IBD. |
| 283 S & Sx of abdominal abscess? | Malaise / anorexia / localized abdo P - constant / swinging fever, typically peaks >38.5 C occuring twice a day / tachycardia / localized abdo tenderness with a possible mass if abscess is in an accessible position eg paracolic. |
| 284 List causes of intra-abdominal abscesses. | Sigmoid diverticulitis / acute appendicitis / severe acute cholecystitis / upper GI perforation / post-anastomotic leakage / infected acute pancreatitis / post-trauma. |
| 286 Discuss the Ix & Mx of an intra-abdominal abscess. | Emergency Mx - resuscitation: IV access if unwell / catheterize & fluid chart if hypotensive / analgesia (eg 5-10mg morphine IV) / bloods for FBC, U & E, CRP, group & save / establish a Dx (helical CT is Ix of choice or pelvic US transabdominally or vaginally is occasionally used) / early Rx (IV ABx's). Definitive Mx: Drainage guided by US or CT where possible / open surgical drainage if radiologically guided drainage is difficult or is recurrent. See OHCS p308. |
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.