7360850
Beschreibung
Karteikarten von Andrew Street, aktualisiert more than 1 year ago
|
|
Erstellt von Andrew Street
vor fast 8 Jahre
|
|
| Frage | Antworten |
| Features of upper GI bleeding. | * Haematemesis * Melaena - can occur with bleeding from any lesion proximal to the R colon. Following a bleed from the upper GI tract, unaltered blood can appear PR, but the bleeding must be massive & almost always accompanied by shock. * The passage of dark blood & clots without shock is always due to lower GI bleeding K & C p254. |
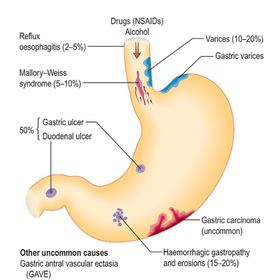
| Causes of upper GI bleeding. Pic from K & C p254. | |
| What factors affect the risk of rebleeding & death? | * Age * Evidence of co-morbidity, eg HF, IHD, CKD & malignant DS * Clinical features of shock (pallor, cold peripheries, tachycardia & low BP) * Endoscopic Dx eg Mallory–Weiss tear, peptic ulceration * Endoscopic stigmata of recent bleeding, eg adherent BD clot, spurting vessel * Clinical signs of chronic liver DS K & C p255. |
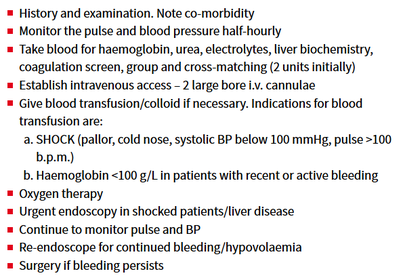
| Mx of acute GI bleeding (in addition to stopping NSAID's, aspirin, clopidogrel, warfarin) From K & C p255. | |
| What role does endoscopy have in Dx & Rx of upper GI bleeding? | Endoscopy will usually make a Dx, risk stratify & enable Rx to be performed. Should be ASAP after pt has been resuscitated. At first endoscopy: * Varices should be Rx'd - usually with banding. Stenting is a recent innovation, not yet widely available. * Bleeding ulcers & those with stigmata of recent bleeding - Rx with two/three haemostatic methods, usually injection with epinephrine and thermal coagulation or endoscopic clipping * Antral biopsies should be taken to look for H. pylori K & C p256. |
| Drug Rx for pt's with actively bleeding ulcers. | After Dx at endoscopy, IV omeprazole 80 mg followed by infusion 8 mg/h for 72 hours. K & C p256. |
| Massive bleeding from the lower GI tract is rare & usually due to diverticular DS or ischaemic colitis. What are some common causes of smaller lower GI bleeds? Pic from K & C p257. | |
| Mx & Ix of lower GI bleeding. | * Most acute lower GI bleeds start & stop spontaneously * If haemodynamically unstable resuscitate as for upper GI bleeding * SX rarely required Dx made using the Hx, exam (including DRE) & following Ix's as appropriate: * Proctoscopy (eg anorectal DS, esp haemorrhoids) * Flexi sigmoidoscopy or colonoscopy (eg inflammatory bowel DS, CA, ischaemic colitis, diverticular DS, angiodysplasia) * Angiography – vascular abnormality (eg angiodysplasia) Rx individual lesions as appropriate. K & C p257. |
| How do pt's with chronic bleeding usually present & what DS's need to be excluded? | Pt's with chronic bleeding usually present with iron-deficiency anaemia. Chronic BD loss producing iron deficiency anaemia in all men, & all women after the menopause, is always due to bleeding from the GI tract. Primary concern is to exclude CA, particularly of stomach or R colon, & coeliac DS. K & C p257. |
| Ix of chronic GI bleeding. | Hx & exam may indicate the most likely site of bleeding, if no clue is available it is usual to Ix both upper & lower GI tract endoscopically. * Upper GI endoscopy usually performed 1st. Duodenal biopsies should always be taken to exclude coeliac DS, which is a recognized cause of iron deficiency. * Colonoscopy follows, any lesion should be biopsied or removed, though it is not safe to assume that colonic polyps are the cause of chronic blood loss. * Unprepared CT scanning is a reasonable test to look for colon CA in frail pt's * If all above fail then capsule endoscopy of small bowel K & C p257. CT colonography can be used as an alternative to colonoscopy. |
| Rx of chronic GI bleeding. | * Cause of bleeding should be Rx'd if found * Oral iron - to Rx anaemia although IV infusions occasionally required. Some pt's will require maintenance with regular transfusion as a last resort. K & C p257. |
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.