9588476
Beschreibung
Karteikarten von Mohamed Saad, aktualisiert more than 1 year ago
|
|
Erstellt von Mohamed Saad
vor mehr als 7 Jahre
|
|
| Frage | Antworten |
| Meningitis is defined as inflammation of the ----- matter of the brain? | Pia matter which covers the brain |
| Which of the following is the main mechanism of meningitis? a. Hematogenous spread from a mucosal surface (nasopharynx) b. Direct extension from a parameningeal focus (AOM, sinusitis, orbital cellulitis) | A |
| Majority of organisms causing bacterial meningitis originate in ------ | Nasopharynx |
| Most of agents causing viral meningitis are transmitted by: 1. Respiratory rout 2. Feco-oral route | 1 Feco-oral > resp. |
| The MCCs of bacterial meningitis in neonates are ------? | GBS (S. agalactiae ) E.coli L.monocytogenes |
| MCCs of bacterial meningitis in infants and children > 1 month? | S. pneumoniae and N. meningitidis |
| Mention the most likely bacterial pathogens in the following scenarios: 1. Meningitis in asplenia patients 2. Meningitis in patients with complement deficiency 3. Meningitis in basilar skull fractures 4. Meningitis in patients on excess steroids 5. Meningitis in patients with absent opsonizing antibody 6. Meningitis in HIV patients 7. Meningitis in patients with bacteremia/endocarditis | 1. S. pneumoniae and N. meningitidis 2. N. meningitidis 3. S. pneumoniae 4. L. monocytogenes and C. neoformans 5. S. pneumoniae and H. influenzae 6. C. neoformans, S. pneumoniae and L. monocytogenes 7. S. aureus |
| The MCC of community-acquired bacterial meningitis in adults is ----? | S. pneumoniae |
| The major causes of healthcare-associated bacterial meningitis are ---------? . | Staphylococci and aerobic gram-negative bacteria (e.g., Pseudomonas aeruginosa, Klebsiella pneumoniae) |
| Which factors predispose to L. monocytogenes meningitis? | 1. Defects in cell-mediated immunity, e.g., a. high dose glucocorticoids b. transplantation [esp. renal transplantation] 2. Alcoholism 3. Pregnancy 4. Malignancy 5. Liver disease |
| Give the potential causative agent in each of the following scenario: a. Meningitis after exposure to rodents b. Meningitis after exposure to ticks c. Meningitis after exposure to mosquitoes d. Meningitis after sexual activity e. Meningitis after contact with other individuals with viral exanthems f. Meningitis + VII palsy | a. LCMV b. Lyme borrelia, RMSF, ehrlichia c. West Nile virus, St. Louis encephalitis virus d. HSV-2, HIV, syphilis e. Enteroviruses (echoviruses, coxsackieviruses, poliovirus) f. Sarcoidosis |
| Causes of aseptic meningitis? | 1. Viral (enteroviruses, HSV-2, HIV, VZV, measles, mumps) 2. Bacterial (partially treated bacterial meningitis, epidural/subdural abscess, Leptospira, Lyme disease, TB, endocarditis) 3. Fungal (Cryptococcus neoformans, Coccidioides immitis, Histoplasma capsulatum > Candida, Aspergillus, Blastomyces dermatitidis, Sporothrix schenckii) 4. Parasitic ( Angiostrongylus cantonensis, Toxoplasma gondii > Taenia solium (cysticercosis), Trichenella spiralis) 5. Drugs (lbuprofen > other NSAIDs, TMP/SMX, anti-CD3 monoclonal antibody, azathioprine) 6. Malignancy (leukemia, lymphoma, metatstatic carcinomas, adenocarcinomas) 7. Others (epidermoid cyst, postvaccination) |
| Choose between encephalitis and meningitis? 1. HSV-1 2. HSV-2 3. Rabies 4. Enteroviruses (echoviruses, coxsackieviruses, poliovirus) 5. West Nile virus 6. CMV 7. VZV 8. EBV 9. HIV 10. Infleunza virus 11. Measles and mumps viruses | 1. Encephalitis 2. Meningitis 3. Encephalitis 4. Meningitis 5. Encephalitis 6. Encephalitis 7. Meningitis 8. Encephalitis 9. Both meningitis and encephalitis 10. Encephalitis 11. Meningitis |
| MCC of bacterial meningitis in infants and children > 1 month? | S. pneumoniae and N. meningitidis |
| Mention the most likely bacterial pathogens in the following scenarios: 1. Meningitis in asplenia patients 2. Meningitis in patients with complement deficiency 3. Meningitis in basilar skull fractures 4. Meningitis in patients on excess steroids 5. Meningitis in patients with absent opsonizing antibody 6. Meningitis in HIV patients 7. Meningitis in patients with bacteremia/endocarditis | 1. S. pneumoniae and N. meningitidis 2. N. meningitidis 3. S. pneumoniae 4. L. monocytogenes and C. neoformans 5. S. pneumoniae and H. influenzae 6. C. neoformans, S. pneumoniae and L. monocytogenes 7. S. aureus |
| The classic triad of meningitis include ---? | fever, neck stiffness & altered mental status - NB: this triad is not sensitive for meningitis - NB: This triad is often dramatic in gram-negative bacillary meningitis (e.g., from E.coli) |
| What is Brudzinski's Sign? | Passive neck flexion causes involuntary flexion of hips and knees |
| What is Kernig's Sign? | Resistance to knee extension when hip is flexed to 90º |
| Signs of Meningismus are --------? | "BONK" on the head Brudzinski's sign Opisthotonos (Rigid spasm of the body, with the back fully arched and the heels and head bent back) Nuchal rigidity Kernig's sign |
| Which of the following is more sensitive for meningitis? A. Brudzinski's sign B. Kernig's sign C. Jolt accentuation of headache | C. Jolt accentuation is more sensitive for meningitis than Brudzinski's and Kernig's (headache worsens when head turned horizontally at 2-3 times/second;but further research is needed) |
| Meningitis in neonates can cause hypothermia a. True b. False | A (true) |
| A patient with meningitis developed these skin lesions. What is the most likely causative agent? | S. pneonia is the most likely cause in patients with meningitis and petechial/purpuric rash |
| Hyponatremia in patients with meningitis can be caused by -----? | SIADH (so, restrict water intake till SIADH is excluded) |
| Basilar meningitis occurs in meninigitis caused by -------? | Basilar meninigitis affects the the base of the brain and is usually caused by TB and fungal infection |
| The definitive test to diagnose meningitis is ---? | L.P. for CSF exam. |
| Relative contraindications of LP include ------? | Suspected epidural abscess Thrombocytopenia (platelets <50.000) NB: Bacteremia is not a contraindication for LP |
| Indications for CT or MRI in meningitis? | 1. Immunocompromised state (e.g., HIV infection, immunosuppressive therapy, solid organ or HSCT) 2. If mass lesion is suspected (e.g., papilledema, recent seizures or focal neurologic findings) to avoid cerebral herniation during CSF removal 3. Abnormal level of consciousness 4. History of CNS disease (mass lesion, stroke, or focal infection) NB: A screening CT scan is not necessary in the majority of patients with meningitis NB: If CT came negative, LP can be done |
| Meningitis + low glucose/CSF? | Bacterial, fungal, TB (all except viral) Viruses don't like glucose |
| Meningitis + high opening CSF pressure | Bacterial, fungal, TB Opening pressure may be normal in aseptic meningitis |
| Meningitis + high lymphocytes/CSF? | Fungal TB Viral |
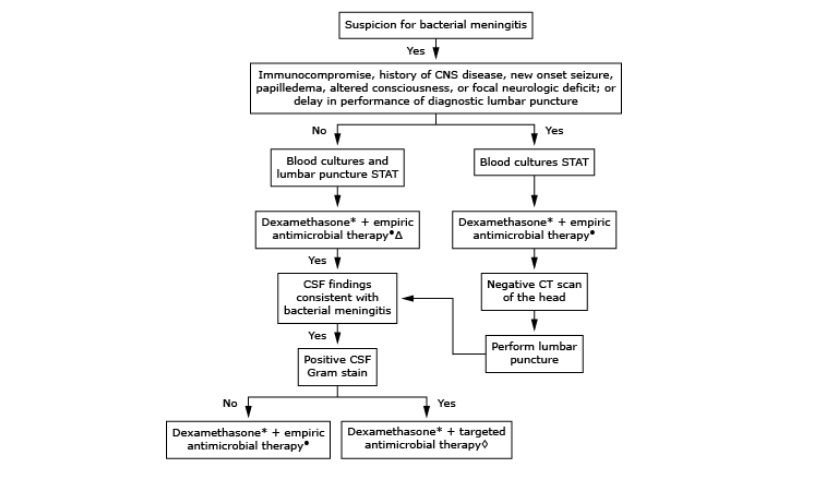
| Can you describe the SEQUENCE of management of meningitis? | a. If LP is not contraindicated: LP + 2 blood cultures, then dexamethasone and empiric antibiotics (to be narrowed according to culture result and gram stain) b. If LP is contraindicated: 2 blood cultures, then dexamethasone and empiric antibiotics, then CT |
| Indications of corticosteroids in meningitis? | If acute bacterial meningitis is strongly suspected clinically until microbiologic results are available - IV dexamethasone should be given shortly before or with first dose of antibiotics (not recommended in patients who have already received antibiotics) - continue if proven pneumococcal meningitis (add oral Rifampin to the standard antibiotic regimen in this case as dexamethasone decrease vancomycin penetration of the CSF) - not recommended for neonatal meningitis (can be used in children) |
| Why is dexamethasone added in bacterial meningitis? | To decrease the rate of hearing loss and other neurologic complications as well as mortality |
| Antibiotics of choice for bacterial meningitis in a neonate baby (<4 weeks)? | Ampicillin PLUS Cefotaxime or, Aminoglycoside |
| Antibiotics of choice for bacterial meningitis in ages 1 month - 50 years? | Vancomycin PLUS 3rd generation cephalosporin |
| When to add ampicillin in treatment for meningitis? | If >50 yrs, or have a risk factor for L. monocytogenes, e.g., 1. Defects in cell-mediated immunity, e.g., a. high dose glucocorticoids b. transplantation [esp. renal transplantation] 2. Alcoholism 3. Pregnancy 4. Malignancy 5. Liver disease |
| A patient with impaired cell immunity developed meningitis, how to treat ? | Vancomycin PLUS Ampicillin PLUS EITHER Cefepime Meropenem |
| A patient with severe allergy to B. lactams develops meningitis, how to treat? | Vancomycin (IV) PLUS Moxifloxacin (excellent CSF penetration) PLUS TMP-SMX (if Listeria coverage is required) |
| Which antibiotic should be added if L. monocytogenes is suspected? | Ampicillin TMP-SMX (if penicillin-allergic) |
| What are the antibiotics of choice in these cases? a. S. pneumoniae meningitis b. N. meningitidis meningitis c. H. influenzae meningitis d. S. agalactiae meningitis e. E.coli meningitis f. Pseudomonas aeruginosa meningitis g. Staph. epidermidis meningitis | a. Vancomycin + 3rd-generation cephalosporin + rifampin (if dexamethasone was used) b. 3rd-generation cephalosporin c. 3rd-generation cephalosporin d. Ampicillin e. 3rd-generation cephalosporin f. Cefepime or ceftazidime g. Vancomycin |
| Medications used for treatment of meningitis are given ---- | I.V (for CNS penetration) except Rifampin which is given orally |
| How to treat meningitis after neurosurgery of peneterating head trauma? | Vancomycin PLUS Cefepime, or Ceftazidime, or Meropenem In this case, common bacterial pathogens include, P. aeruginosa, S. aureus , S. epidermidis. |
| Antibiotics of choice for bacterial meningitis in people >50 years? | Vancomycin PLUS Ampicillin PLUS 3rd generation cephalosporin |
| Ampicillin can be used for treatment of meningitis caused by which pathogens ? | 1. L. monocytogenes 2. GBS (S.agalactiae ) |
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.