11812381
Description
Flashcards by Anna Hogarth, updated more than 1 year ago
|
|
Created by Anna Hogarth
almost 7 years ago
|
|
| Question | Answer |
| 1. Draw a labelled diagram showing the anatomy of the microcirculation. 2. Describe the three types of capillaries, continuous, fenestrated and discontinuous, with reference to their structure, distribution and function. 3. Describe how lipid insoluble molecules can move across the capillary endothelium. 4. Draw a labelled diagram showing filtration and reabsorption of fluid along an average capillary. 5. Explain how capillary pressure, plasma colloid osmotic pressure and interstitial colloid osmotic pressure can affect fluid movements between plasma, interstitium and lymph. 6. Know the different causes of oedema and explain the pathophysiology of each. | X |
| What are the three layers of the blood vessel wall? | 1. Tunica intima 2. Tunica media 3. Tunica adventitia |
| What is the average diameter and wall thickness of a capillary? What are capillaries known as? | 1) 8um and 0.2um 2) Exchange vessels - capillaries are the site of exchange nutrients and waste products between the circulation and interstitial fluid which surrounds cells. |
| What is the order of vasculatures from small arterioles structures? | Small arterioles - first-order arterioles - terminal arterioles (precapillary sphincters) - capillaries - venules |
| What is the diameter of small arteries? Terminal arterioles? Capillaries? How long are capillaries? | 1) 100-500 um 2) 10-40 um 3) 5-8 um 4) 500-1000 um |
| Which part of the oxygenated blood system receive sympathetic innervation? | First order arterioles, terminal arterioles receive fewer nerves |
| What forms the vascular shunt? What regulates flow through capillaries? | 1) Metarteriole (oxygenated) and thoroughfare channel (deoxygenated) - bypasses the capillary bed. 2) Capillary sphincters |
| What is the basic structure of capillaries? | Endothelial cells held together by tight junctions surrounded by a basement membrane - no smooth muscle. |
| What are the three different types of capillaries? | 1) Continuous 2) Fenestrated 3) Discontinuous/sinusoidal |
| Describe continuous capillaries (anatomy and characteristics). | Pericytes surround the basement membrane, no gaps, tight junctions and intercellular clefts. Pinocytic vesicles in the endothelial cells. Sealed endothelium means that these are the least permeable of the different classes of capillaries. Only allow small molecules like water and ions to diffuse. |
| What are the two different types of continuous capillaries? | 1) Those with numerous transport vesicles (caveolae) such as in the lungs, skeletal muscle, skin and gonads. 2) Those with fewer vesicles which are found in the central nervous system (such as the BBB) |
| How do fenestrated capillaries differ from continuous? What is their function and where are they found? | 1) Still continuous/closed basement membrane, basal lamina and pericytes but fenestrations (small pores 60-80 nm in diameter) within in the endothelial cells. 2) Permit relatively free passage of salts and water. Found in tissues where bulk exchange is required, such as in exocrine glands, intestines, pancreas and the glomeruli of kidneys. |
| How do sinusoidal/discontinuous capillaries differ from continuous capillaries? What is their function and where are they primarily located? | 1) Contains specialised large fenestrations (30-40 um in diameter), an incomplete basement membrane/basal lamina and there may be very large intercellular clefts/gaps between the endothelial cells. They also lack pinocytic vesicles. 2) Are the most permeable of the different types of capillary. Allow the passage of large solutes, serum proteins and even cells such as WBCs and RBCs - as such are found in the spleen, bone marrow and liver. |
| What are the different types of transport through into the capillary lumen and for what kinds of substances? | 1) Directly through the membrane (lipid soluble) 2) Through the intercellular cleft (water soluble) 3) Through fenestrations (water soluble) 4) Transports via caveolae or vesicles (large substances) |
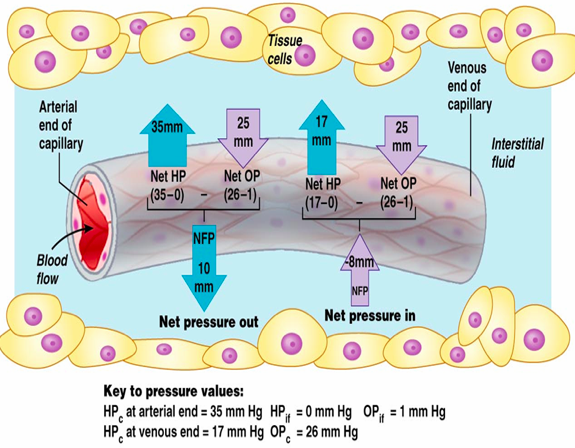
| What regulates the movement of water across capillary endothelium? What values would you expect at the different ends of the capillary beds? | 1) The balance of hydrostatic pressure (generated by heart beat) and oncotic pressure (generated by large solutes) between the plasma and interstitial fluid. 2) Hydrostatic pressure of the capillary at the arterial end is around 35 mmHg at the arterial end and 17 mmHg at the venous end. The interstitial hydrostatic pressure is usually zero. The colloid oncotic pressure of plasma is around 26 mmHg (due to plasma proteins) and 1 mmHg in the interstitial fluid. |
| How is the net filtration calculated? | NF = (HPc - HPif) - (OPc - OPif) |
| Using the values described before, what are the net filtration pressures at the arterial and venous end of the capillary bed? | Arteriole end: NFP = (35-0) - (26-1) = 10 mmHg = water forced out FILTRATION Venous end: NFP = (17-0) - (26-1) = -8 mmHg water force in REABSORPTION Note that overall more fluid is forced out - hence the need for lymphatics. |
| X | |
| What does the Starling hypothesis state regarding capillaries? | Plasma proteins don't tend to leave the capillaries, constant oncotic pressure - as a result fluid tends to leave the capillaries at the arterial end, and be drawn back in at the venous end. Altering either hydrostatic or oncotic pressure will disturb the fluid balance across the capillary. |
| How much plasma passes through the capillaries every day? How much is filtered? What happens to the majority of this? | 1) 4,000 litres 2) 0.1-0.2% = 4.8 litres of fluid moves from the plasma to the interstitial fluid. 3) Some is reabsorbed but the vast majority is drains into the lymphatics. |
| Describe the three key structural aspects of the lymphatic capillaries? | 1) Large intercellular gaps between endothelial cells and a permeable basement membrane. 2) End in blind sacs within tissues 3) Contain one way valves to ensure lymph all travels in one direction. |
| What are the two possible movements of fluid once it has entered the lymphatics? | 1) Enters into the subclavian veins and returns to circulation 2) Water reabsorption into the circulation at the lymph nodes |
| How much of the lymph is returned to circulation everyday? What does a disruption of this lead to? | 1) 2-4L 2) Oedema |
| What is oedema? | Increased fluid in the interstitial fluid leads to swelling leading to FLUID RETENTION |
| What are the main types of oedema? | Systemic and peripheral - systemic tends to originate in the periphery i.e. at the ankles. Can be transient i.e. due to long periods of sitting or standing (long periods of standing increases venous pressure). Oedema can be determined by applying pressure and it leaves an indent in the tissue - pitting oedema. |
| What two things lead to oedema? | Increased filtration and secretion along with impaired removal of fluid - for example if the lymphatics are blocked. |
| What are the four factors which precipitate oedema? | 1) Increased capillary hydrostatic pressure 2) Decreased capillary oncotic pressure 3) Increased water permeability of the capillaries 4) Obstruction of the lymphatics |
| What would cause an increase in capillary hydrostatic pressure? | An increase in venous pressure - this could occur due to an increase in gravitational forces or due to heart failure (blood pools in the vein system) |
| What can cause plasma oncotic pressure to decrease? | Hypoproteinemia - this can occur due to malnutrition or liver disease. |
| What is Kwashiorkor? How does it lead to oedema? What is the common presentation in children? | 1) Severe malnutrition caused by a deficiency in dietary proteins 2) Reduction of capillary oncotic pressure which leads to pitting oedema 3) Water retention in gut - large distended bellies in children |
| Why does increased capillary permeability lead to oedema? How might increased capillary permeability occur? | 1) Allows water to flow more freely and it reduces oncotic pressure difference as proteins are more able to freely leave the vasculature. 2) Vascular damage e.g. burns, trauma and inflammation |
| What conditions might cause obstruction of lymph drainage? | 1) Fibrosis 2) Filariasis (worm infestation, elephantiasis) 3) Inflammation of lymph vessels 4) Tissue injury |
| How is oedema treated? | The underlying pathology needs to be treated. To reduced the symptoms water and salt need to be excreted. Can use osmotic diuretics - increases excretion of water; loop diuretics - increases excretion of sodium, natriuresis |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.