4282795
| Question | Answer |
| Classic Community Acquired Pneumonia Characteristics | Acquired in the home or non-hospital environment Most cases, causative agent not identified, but usually bacterial Causative agents include: Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Staphylococcus aureus, Kelbsiella pneumoniae, other gram negative bacilli. Viral causes: influenza, RSV, adenovirus, parainfluenza |
| Community Acquired Pneumonia (CAP) Clinical Features | Typical presentation is 1-10 day history of Increaseing cough, prurulent sputum, SOB, tachycardia, pleuritic chest pain, fever or hypothermia. Physical exam may reveal altered breath sounds and crackles,dullness to percussion if an effusion present, and bronchial breath sounds over an area of consolidation. The chest exam alone is not enough to confirm or exclude the diagnosis. |
| Community Acquired Pneumonia (CAP) Laboratory Findings | Organisms may be detected with conventional stain or sputum culture, although typically not done before starting treatment. The most common bacterial pathogen found ins Streptococcus pneumoniae. CXR shows lobar or segmental infiltrates, air bronchograms and pleural effusions. THere is no pathognomonic radiograph presentation. |
| Community Acquired Pneumonia (CAP) Treatment for otherwise healthy patient | Patient is otherwise healthy and free of respiratory distress or complications. May be treated as an outpatient with oral antibiotics and appropriate supportive care. Doxycycline, erythromycin, Macrolides (clarithromycin, azithromycin), or fluoroquinalines. |
| Community Acquired Pneumonia (CAP) Treatment for more severe or complications | Neutropenia, involvement of more than one lobe, or poor host resistance indicates need for hospitalization. Consider hospitalization for patients older than 50 with Comorbidities, altered mental status, or hemodynamic instability. If inpatient treatment necessary consider coverage for Streptococcus pneumoniae and Legionella sp. with ceftriaxone or ceftaxime plus azithromycin or a fluoroquinalone. |
| Community Acquired Pneumonia (CAP) Vaccines | The polyvalent pneumococcal vaccine (Peumovax) contains antigens of 23 common strains. Efficacy ranges from 51-86%. Pneumococcal conjugate vaccine (PCV) s recommended in children 6 weeks to 15 months. The pneumococcal polysaccharide vaccine (PPV is recommended for children 2-5 not previously immunized and adults 65 or older or any person with chronic illness that increases risk of CAP. Booster shots needed every 6 years. |
| Mycoplasma pneumonia Symptoms | Low-grade fever Cough Bullous my ringgits Cold agglutinins |
| Pneumocystis jerovici Symptoms | Slower onset, immunosuppression Increased lactate dehydrogenase More hypoxemic than appears on chest radiography Interstitial infiltrates |
| Legionella pneumoniae Symptoms | Chronic cardiac or respiratory disease Hyponatremia Diarrhea, other systemic symptoms |
| Chlamydia pneumoniae Symptoms | Longer pro drone Sore throat, hoarseness |
| Streptococcus pneumoniae Symptoms | Single rigor Rust-colored sputum |
| Klebsiella pneumoniae Symptoms | Currant jelly sputum Chronic illness, including alcohol abuse |
| Kelbsiella pneumoniae Patient Group | Alcohol abuse |
| Haemophilus pneumoniae Patient group | COPD |
| Pseudomonas Patient Croup | Cystic Fibrosis |
| Mycoplasma pneumoniae Chlamydia pneumoniae Patient group | Young adults College settings |
| Legionella pneumoniae Patient group | Air conditioning/aerosolized water |
| Encapsulated organisms Streptococcus pneumoniae Haemophilus pneumoniae Patient group | Postsplenectomy |
| Fungus Patient group | Leukemia, lymphoma |
| RSV Patient group | Children, <1 year |
| Parainfluenza Patient group | Children, <2 years |
| Atypical CAP General characteristics | Mycoplasma pneumonia is the most common atypical. Other causes include viruses (influenza A and B and adenovirus), Chlamydia pneumoniae, Legionella sp. and Moraxella sp. |
| Atypical CAP Clinical Features | Presents as a low-grade fever with relatively mild pulmonary symptoms which are self limited, occuring in young, otherwise healthy adults. A non productive cough, myalgia, and fatigue are common. Legionella infection associated with exposure to contaminated water droplets from cooling and ventilation symptoms. Acute development of high fever, dry cough, Dyspnea, and systemic symptoms is common. Viral pneumonias are variable in presentation but are often associated with epidemics and upper resp. symptoms. |
| Atypical CAP Laboratory findings | Organisms are usually not detected with conventional stain or culture of sputum. The WBC count is normal or only slightly elevated. Radiography shows segmental unilateral lower lung zone infiltrates or diffuse infiltrates. |
| Atypical CAP Treatment | Antibiotic treatment is started empirically based on the clinical features. Regimens include erythromycin (for suspected mycoplasma and legionella) and tetracycline (for suspected chlamydia) Viral pneumonias are treated with supportive measures unless influenza is suspected. Neuraminidase inhibitors (inhaled zanamivir or oral oselamivir) may be used. |
| Nosocomial pneumonia General characteristics | Hospital acquired pneumonia is caused by organisms that colonize ill patients, staff, equipment, producing clinical infection more than 48 hours after admission to the hospital. THose at highest risk are in ICU or mechanical ventilation. Pneumonia is second most cause of hospital acquired infection. The causative organisms are unique and mortality is 20-50%. The usual organisms are Stphylococcus aureus and gram negative bacilli, which are easy to recover from respiratory secretions. Pseudomonas aeruginosa is the most likely pathogen in the ICU an carries worst prognosis. Others are Staphylococcus aureus, Klebsiella, Escherichia coli, and Enterobacter. |
| Nosocomial pneumonia Clinical features | Similar to CAP Typical presentation is 1-10 day history of Increaseing cough, prurulent sputum, SOB, tachycardia, pleuritic chest pain, fever or hypothermia. Physical exam may reveal altered breath sounds and crackles,dullness to percussion if an effusion present, and bronchial breath sounds over an area of consolidation. |
| Nosocomial pneumonia Laboratory findings | Diagnosis is clinical and supported with gram stain and culture of sputum and blood. CXR may help support the diagnosis. |
| Nosocomial pneumonia Treatment | Includes use of appropriate empiric antibiotics such as cefepime, ticarcillin/calculatio acid, piper amcillin/tazobactam, meropnem. If an organism is isolated, therapy can be based on the culture results. Patients need aggressive supportive measures including ventilation as appropriate. |
| TB General characteristics | Mycobacterium tuberculosis infection is acquired by inhaling organisms within aerosol droplets expelled during coughing by people with active disease. Most exposed people mount an immune response sufficient to prevent progression from primary infection to clinical illness. Overall, 10% if persons infected with TB will develop the disease. This is called primary TB. Approximately 5% of exposed people fault to contain the primary infection and progress to active TB within 2 years, this is known as progressive primary RB. Approximately 95% of infected persons will contain the bacterium without becoming symptomatic. This is known as latent TB infection. These patients are not considered to be infectious, nor can they spread the disease. Reactivation TB develops from latent TB in the setting of immune compromise. Outbreaks since the 90's have seen an emergence of resistant organisms. |
| TB Clinical features | Cough is the most common symptom. It begins as a dry cough and progresses to a productive cough with or without hemoptysis, typically over 3 weeks or longer. The classic symptom complex includes fever, drenching night sweats, anorexia, and weight loss. Other common classic pulmonary symptoms are cough, pleuritic chest pain, duspnea, and hemoptysis. Posttusive rales are classic. On exam, the patient may appear chronically ill and malnourished. |
| TB Laboratory findings Primary TB | Homogenous infiltrates, hilar/parathracheal lymph node enlargement, segmental Atelectasis, cavitation S with progressive disease |
| TB Laboratory findings Reactivation TB | Fibroma votary apical disease, nodules, infiltrates, posterior and apical segments of the right upper lobe, apical-posterior segments of the left upper lobe, superior segments of the lower lobes. |
| TB Laboratory findings When healed | Ghon complexes (Calcified primary focus) and Ranke complexes (calcified primary focus and calcified hilar lymph node) represent healed primary infection. |
| TB Skin Test (TST) | Identifies individuals who have been infected, but it does not differentiate between active and latent infection. Tuberculin skin testing (such as the PPD) is report according to the diameter of induration, not erythema. |
| TB Diagnosis | Requires the identification of Mycobacterium tuberculosis from cultures by DNA or RNA amplification techniques. Demonstration of acid fast bacilli on sputum supports, but does not confirm a diagnosis. |
| TB Diagnosis Biopsy | Biopsy revealing caseating granuloma (also known as necrotizing granulomas) is the histologic hallmark. |
| TB Treatment | Antituburculosous drugs including isoniazid (INH), rifampin (RIF), pyrazinamide (PZA), and ethambutol (EMB), are the cornerstone of therapy. |
| TB Treatment Side Effects | INH: hepatitis, peripheral neuropathy, coda minister with B6 to reduce risk. RIF: hepatitis, flu syndrome, orange body fluid. EMB: optic neuritis (red-green vision loss) |
| TB Skin Test Interpretation | >=5mm: Considered + in HIV+, recent contacts of those with active TB, persons with evidence of TB on chest radiography, immunosuppressed patients on steroids. >=10mm: Considered + in recent immigrants from countries with high rate of TBm HIV- injection drug users, myco bacteriology lab personnel, residents/employees of high risk congregate settings, persons with certain medical conditions (diabetes, silicosis, chronic renal failure, etc.), children younger than 4, infants, and children/adolescents exposed to adults at high risk. >=15mm: Considered + in those with no risk factors for TB |
| Acute bronchitis General characteristics | More than 90% of cases are caused by viruses including rhinovirus, corona virus, and RSV. Bronchitis is defined as inflammation of the airways (trachea, bronchi, bronchioles) characterized by cough) In patients with chronic lung disease, causes also include Haemophilus influenza, Streptoccocus pneuma, and Moraxella catarrhalis. |
| Acute bronchitis Clinical features | Signs and symptoms include cough (with or without sputum), Dyspnea, fever, sore throat, headache, myalgia S, subset renal discomfort, and expiratory rhonchi or wheezes. Bronchitis can be difficult to distinguish from pneumonia so the examination should be conducted to identify Comorbidities conditions that may influence the treatment. |
| Acute bronchitis Laboratory findings | Generally, no laboratory evaluation is required unless there is a strong need to differentiate bronchitis from pneumonia. The CXR will be negative in acute bronchitis. |
| Acute bronchitis Treatment | Supportive measures include hydration, expectorants, analgesics, β2-agonists, and cough suppressants. For acute exacerbations of chronic bronchitis, in which bacterial causes are more likely, empiric first line treatement is a second generation cephalosporin; second line treatment is a second generation Macrolides or trimethoprim/sulfamethoxazole. Antibiotics are indicated fro elderly patients, those with underlying cardiopulmonary disease and a cough for more than 7-10 days, and any patient who is immunocompromised. For acute exacerbations in otherwise healthy adults, no empiric treatment is needed. |
| Acute bronchiolitis General characteristics | Bronchiolitis refers to inflamation of the bronchioles (airways smaller than 2mm in diameter(. It is primarily an illness of young children and infants. RSV is the most common cause, other agents include parainfluenza, adenovirus, and rhinovirus. |
| Acute bronchiolitis Clinical features | Signs and symptoms include rhinos rhea, sneezing, wheezing, and low-grade fever Nasal flaring, tachyons, and retractions indicate respiratory distress. |
| Acute bronchiolitis Laboratory findings | The CBC is usually normal. Nasal Washington for RSV culture and antigen assay often are done in infants. CXR normal but can show air trapping and peribronchial thickening. |
| Acute bronchiolitis Treatment | If RSV is present, consider hospitalization and administration of ribavirin. This is especially important for infant born premature or who are severely ill. Supportive measures, such as nebulized albuterol, IV fluids, antipyretic S, chest physiotherapy, and humidified O2. |
| Bronchogenic carcinoma General | Bronchogenic carcinoma is the leading cause of cancer deaths in men and women. There are more deaths from lung cancer than from colon, breast, and prostate combined. The overall 5 year survival rate is 15%. Smoking is the #1 risk factor. |
| Bronchogenic carcinoma SCLC General | Accounts for 25-35% of cases; it is more likely to spread early and rarely is amenable to surgery. Mean survival is 6-18 weeks. Tends to originate in the central bronchi and to metastasize to regional lymph nodes. It is prone to early metastasis and an aggressive clinical course. Assume micrometasteses at presentation. |
| Bronchogenic carcinoma NSCLC General | Grows more slowly and is more amenable to surgery. Includes squamous cell carcinoma, adenocarcinoma, and large cell carcinoma. |
| Bronchogenic carcinoma NSCLC - Squamous Cell Carcinoma General | Represents 25-35% of cases. Bronchiole in origin and a centrally located mass. More likely to present with hemoptysis and there fore more likely to be diagnosed via sputum cytology. |
| Bronchogenic carcinoma NSCLC - Adenocarcinoma General | The most common type of bronchogenic carcinoma, accounting for 35-40% of cases. Typically metastatic to distant organs This tumors arises from mucous glands, usually appears in the periphery of the lung, and is not amenable to early detection through sputum examination. Bronchoaveolar cell carcinoma, a subtype, is a low-grade carcinoma. |
| Bronchogenic carcinoma NSCLC - Large Cell Carcinoma General | A heretogenous group of undifferentiated types that do not fit elsewhere. Cytology typically shows large cells. Doubling time is rapid. Metastasis is early. There may be central or peripheral masses. |
| Bronchogenic carcinoma Clinical features | Symptoms include cough, hemoptysis pain, anorexia, weight loss, or asthenia. Patients may also exhibit lymphadenopathy, hepatomegaly, and clubbing. Paraneoplastic syndromes occur in 10-20% of patients with lung cancer. |
| Bronchogenic carcinoma Laboratory findings | CXR and CT scans usually demonstrate abnormalities. Cytologic examination of sputum, if adequate cells re obtained, permits definitive diagnosis of specific cell type in many cases. Bronchoscopy, examination of pleural fluid, and biopsy are also used to establish a diagnosis by looking at specific cell types through direct visualization. PET scans may also aid in diagnosis and prevent unnecessary surgery. |
| Bronchogenic carcinoma Treatment NSCLC | Surgery remains the treatment of choice. The 5 year survival rate after resection is 35-40% |
| Bronchogenic carcinoma SCLC | Combination chemotherapy is the treatment of choice and results in improved median survival, although patients rarely live for more than 5 years after diagnosis. |
| Bronchogenic carcinoma Complications SVC Syndrome | Compression of SVC: plethora, headache, mental status change |
| Bronchogenic carcinoma Complications Pancoast's tumor | Tumor of the lung apex Causes Horner's syndrome and shoulder pain Affects brachial plexus and cervical sympathetic nerve |
| Bronchogenic carcinoma Complications Horner's syndrome | Unilateral facial anhidrosis, ptosis, miosis |
| Bronchogenic carcinoma Complications Endocrine | Carcinoid syndrome: flushing, diarrhea, telangiectasis |
| Bronchogenic carcinoma Paraneoplastic Syndromes Endocrine/metabolic | Small Cell: Cushing's syndrome, SIADH Squamous cell: Hypercalcemia Large cell: Gynecomastia |
| Bronchogenic carcinoma Paraneoplastic Syndromes Neuromuscular | Small cell: Peripheral neuropathy, myasthenia (Eaton-lambert), cerebellum degeneration |
| Bronchogenic carcinoma Paraneoplastic Syndromes Hematologic | All: Anemia, DIC, eosinophilia, thrombocytosis |
| Bronchogenic carcinoma Paraneoplastic Syndromes Cardiovascular | Adenocarcinoma: thrombophlebitis |
| Bronchogenic carcinoma Paraneoplastic Syndromes Cutaneous | All: Acanosis nigricans |
| Solitary pulmonary nodule General characteristics | Pulmonary nodules are also known as coin lesions. If the lesion measures greater than 3 cm, it is referred to as a mass. Most solitary nodules are infectious granulomas from old or active TB, fungal infection, or foreign body reaction. Approximately 40% are malignant and represent carcinoma, hamartoma, or metastasis (bit these are usually multiple) as well as bronchial adonoma (95% are carcinoid tumors). Malignancy is rare in patients younger than 30 years. Smears have an increased risk of malignancy; risk increases with number of pack-years smoked. |
| Solitary pulmonary nodule Clinical features | Most pulmonary nodules are found unexpectedly at radiography and are asymptomatic. |
| Solitary pulmonary nodule Laboratory findings | A solitary pulmonary nodule is a round or oval, sharply circumscribed mass up to 5cm in diameter surrounded by normal lung tissue. Central cavitation, calcification, or surrounding (satellite) lesions may occur. A lesion that has not enlarged in more than 2 years suggests a benign cause. Most are infectious granulomas. Malignant lesions occasionally are symptomatic, tend to occur in patients older than 45 years, usually are greater than 2cm in diameter, often have in distinct margins, exhibit rapid progression in size and rarely are calcified. |
| Solitary pulmonary nodule Treatment | Lesions with a low probability of malignancy can be watched. Patients should undergo CT every 3 months for a year, if stable, frequency of CT can be reduced to every 6 months for the next 2 years. Lesions with high probability of malignancy should be resected as soon as possible. An interim biopsy is not recommended. Lesions with intermediate probability of malignancy should be biopsied. Use transthoracic needle biopsy or bronchoscopy if the lesion is peripheral. False-positive rates can be as high as 25%. high res CT or PET may aid in diagnosis. High res CT is best to delineate the mass and detect adenopathy Ro the presence of multiple nodules. |
| Obstructive Pulmonary Disease Asthma General Characteristics | Asthma is characterized by three components: Obstruction of airflow Bronchial hyperreactivity Inflammation of the airway -It is a disease of chronic inflammation leading to airway narrowing and increased mucus production. |
| Obstructive Pulmonary Disease Asthma Epidemiology | Asthma effects 7% of the population. Most common among pediatric patients 3rd leading cause of preventable hospitalization Significant mortality (4000/yr) (on the rise) 5-15% of asthmatics are severe. Half of $56 billion costs are spent on severe asthma. |
| Obstructive Pulmonary Disease Asthma Strongest Predisposing Factor | Atopy The atopic triad consists of wheeze, eczema and seasonal rhinitis |
| Obstructive Pulmonary Disease Asthma Common Precipitants/Triggers | *Environmental triggers are the most important Precipitants of severe asthma exacerbations. Allergens (especially dust and dust mites, dander, cockroaches, pollen) Exercise Upper respiratory tract infections Post nasal drip Gastroesophageal reflux disease Drugs (β-blockers, ACEi, aspirin, NSAIDs,) Stress Cold air or weather change Environmental irritants |
| Obstructive Pulmonary Disease Asthma Morphological Changes | Basement membrane thickening/fibrosis Mucus gland hypertrophy and hypersecretion Smooth muscle hypertrophy Epithelial damage Inflammatory cell infiltration Edema Vascular dilation |
| Obstructive Pulmonary Disease Asthma Clinical features | Patients have intermittent occurrence of cough, chest tightness, shortness of breath, and wheezing (associated with coughing). Asthma is classified according to the frequency of symptoms and PFTs. |
| Obstructive Pulmonary Disease Asthma Laboratory Findings Spirometry | Airflow obstruction is indicated by DECREASED ratio of FEV1/FVC. A greater than 10% in FEV1 after bronchodilator therapy is supportive of the diagnosis. |
| Obstructive Pulmonary Disease Asthma Laboratory Findings ABG | ABG (arterial blood gas) measurements may be normal in mild asthma ut in severe cases may show hypoxemia and hypercapnia with a PaO2 < 60mmHg and PaCO2 > 40mmHg. ABGs rarely used unless patient non responsive to treatment. |
| Obstructive Pulmonary Disease Asthma Laboratory Findings CXR | May show hyperinflation. Want to have one on file. Should be <= 5 years. If already on file, then indicated only if pneumonia is suspected, asthma is complicated, or other disorder suspected. |
| Obstructive Pulmonary Disease Asthma Laboratory Findings FeNO (Inflammometer) | Exhaled Nitric Oxide measurement. Correlated with eosinophilia inflammation. Levels decrease with ICS Can predict asthma exacerbations/compliance May correlate with decline in FEV1 FeNO 5-20 NL/controlled FeNO 20-35 NL/elevated FeNO > 35 Elevated |
| Obstructive Pulmonary Disease Asthma Laboratory Findings IgE, Immunocap testing | Specific allergen testing +/- CBC with differential (looks for eosinophils in the blood) 70% of patients are allergic |
| Obstructive Pulmonary Disease Asthma Laboratory Findings Methacholine challenge | Bronchial provocation test An FEV1 decrease of more than 20% is diagnostic. Useful when spirometry is nondiagnostic |
| Obstructive Pulmonary Disease Asthma Treatment Goals | The goals of treatment are to minimize chronic symptoms, prevent recurrent exacerbations and minimize need for urgent care visits, and maintain near-normal pulmonary function. |
| Obstructive Pulmonary Disease Asthma Treatment Medications (Generally) | Long-term Control: Corticosteroids, chromodynamics, LABA, leukotrine modifiers, theophylline. Quick Relief: SABA, ipratropium bromide, systemic corticosteroids) |
| Obstructive Pulmonary Disease Asthma Classification of Severity Intermittent | Symptoms: <= 2 days/week Nighttime: <= 2/month Use of Rescue Meds: < 2 days/week FEV1 > 80% predicted FEV1/FVC normal No interference with daily activities |
| Obstructive Pulmonary Disease Asthma Classification of Severity Mild Persistant | Symptoms: >2 days/week but not daily Nighttime: 3-4/month Use of Rescue Meds: > 2 days/week, but not daily and not more than once per day FEV1 > 80% predicted FEV1/FVC normal Minor limitation on daily activities |
| Obstructive Pulmonary Disease Asthma Classification of Severity Moderate Persistant | Symptoms: Daily symptoms Nighttime: > 1/week, but not daily Use of Rescue Meds: Daily FEV1 > 60% but < 80% predicted FEV1/FVC reduced 5% Some limitation in daily activity |
| Obstructive Pulmonary Disease Asthma Classification of Severity Severe Persistent | Symptoms: Continual symptoms Nighttime: Often 7/week Use of Rescue Meds: Serveral/day FEV1 < 60% predicted FEV1/FVC reduced > 5% |
| Obstructive Pulmonary Disease Bronchiectasis General Characteristics | Defined as abnormal, permanent dilation of the bronchi and destruction of bronchial walls. It can be congential (system fibrosis) or acquired from recurrent infections (TB, fungal, lung abscess) or obstruction (tumor). results from bronchial injury subsequent to severe infection and/or inflamation. Cystic Fibrosis causes half of all cases. |
| Obstructive Pulmonary Disease Bronchiectasis Clinical Features | Symptoms include chronic prurulent sputum (often foul smelling), hemoptysis, chronic cough, recurrent pneumonia. Physical exam may reveal localized chest crackles and clubbing. |
| Obstructive Pulmonary Disease Bronchiectasis Laboratory Findings CT | High resolution Chest Ct is imaging modality of choice. It reveals dilated, tortuous airways. |
| Obstructive Pulmonary Disease Bronchiectasis Laboratory Findings CXR | Will be abnorma. The degree of abnormality depends on the extent and severity of the disease. Crowded bronchial markings and basal cystic spaces are characteristic. May reveal train-track lung markings, honey combing, atelectasis. |
| Obstructive Pulmonary Disease Bronchiectasis Laboratory FIndings Bronchoscopy | Warranted to evaluate hemoptysis, remove secretions, and rule out obstructing lesions. |
| Obstructive Pulmonary Disease COPD General Characteristics | Clinical and pathophysiologic syndrome that includes emphysema and chronic bronchitis. *Smoking is the most important cause of COPD. Other causes include environmental pollutants, recurrent upper respiratory tract infections, eosinophilia, bronchial hyperresponsiveness, and α1-antitrypsin deficiency. |
| Obstructive Pulmonary Disease COPD Epidemiology | ~15 million Americans diagnosed with COPD 63% remain undiagnosed Common, treatable, preventable (except α1-antitrypsin deficiency) |
| Obstructive Pulmonary Disease COPD Clinical Features | Patients present with history of progressive SOB, excessive cough, and sputum production. Advanced COPD may reveal asthenia, dyspnea, pursed lip breathing, grunting expirations. |
| Obstructive Pulmonary Disease COPD Chest Examination | Signs of hyperinflation with increase in the anteroposterior dimension are noted. Percussion yields increased resonance. Auscultation reveals decreased breath sounds and early inspiratory crackles. Wheezing may not be present at rest but can be evoked with forced expiration or exertion. Duration of experiation is prolonged. |
| Obstructive Pulmonary Disease COPD Clinical FIndings Emphysema Predominant | "Pink Puffers" Exertional dyspnea, cough is rare (may be dry), quiet lungs, no peripheral edema, thin (recent weight loss), barrel chest, hyperventilation Radiography: Decreased lung markings at apicies, flattened diaphragm, hyperinflation, small thin appearing heart. Loss of both vessels and surface area for gas exchange, so minimal V/Q mismatch. Oxygenation maintained by increased breathing effort |
| Obstructive Pulmonary Disease COPD Clinical Findings Bronchitis Predominant | "Blue Bloaters" Rhonchi reflect secretions in the airways and breathing typically is raspy and loud. Mild dyspnea, chronic productive cough, noisy lungs (rhonchi and wheeze), peripheral edema, overweight and cyanotic, pursed lip breathing. Radiography: Increased interstitial markings at bases, diaphragm NOT flattened, parenchymal bullae and blebs. Obstruction with preservation of distal parenchyma leads to V/Q mismatch and hypoxemia |
| Obstructive Pulmonary Disease COPD Laboratory Findings CXR | Not sensitive or specific enough to serve as diagnostic or screening tool. May show hyperinflation, flat diaphragm. |
| Obstructive Pulmonary Disease COPD Laboratory Findings PFT | Airflow obstruction demonstrated on forced expiratory spirometry is suggestive. The FEV1/FVC ratio is DECREASED. |
| Obstructive Pulmonary Disease COPD Laboratory FIndings CBC | May show polycythemia caused by chronic hypoxemia. |
| Obstructive Pulmonary Disease COPD Treatment - Generally | *Smoking cessation is the single most important intervention. Anticholiergic inhalers are superior to B-adernergic agonists in achieving bronchodialtion. SABA for acute exacerbations. Antibiotics often necessary. Supplemental O2 therapy in patients with resting hypoxemia (PaO2 <55 or SaO2 <88) Graded aerobic physical exercise encouraged. Use steroids with caution. Pneumococcal and flu vaccines. |
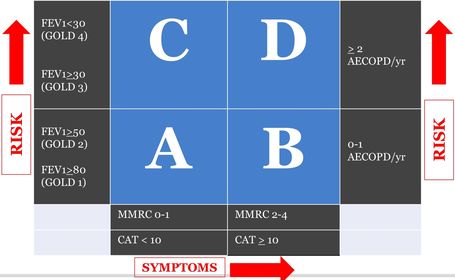
| Obstructive Pulmonary Disease COPD GOLD 2014 Characterization | MMRC = medical research council dyspnea scale AECOPD = acute exacerbation of COPD |
| Obstructive Pulmonary Disease COPD MMRC Scale | Modified Medical Research Council Dyspnea Scale 0 = Not troubled by breathlessness except on strenuous exercise 1= Shortness of breath when hurrying on the level or walking up a slight hill 2 = Walks slower than people of the same age on level because of breathlessness or has to stop for breath when walking at own pace on the level. 3 = Stops for breath after walking about 100m or after a few minutes on the level. 4 = Too breathless to leave the house or breathless when dressing or undressing. |
| Obstructive Pulmonary Disease COPD Hospital Readmissions Reduction Program | COPD affects 24 mil in USA, 65 mil worldwide > 700,000 hospitalizations/year $35 bill in inpatient costs 1 in 5 readmitted within 30 days 3rd highest rate of readmission 3rd highest source of cost Half admitted without interim office visit Critical inhaler technique errors prevalent Treatments fall short of guidelines |
| Obstructive Pulmonary Disease COPD Comorbidities | Environmental Factors: Smoking, sedentary lifestyle, diet, obesity Biologic Factors: Systemic inflammation, oxidative stress, endothelial dysfunction, genetics, age, hypoxemia. |
| Obstructive Pulmonary Disease COPD Impact of Comorbidities | Chronic State: Higher symptom burden, lower quality of life, higher costs of care. Exacerbations: prolonged recovery times, more frequent complications, higher admission/readmission rate Survival: Higher all-cause mortality, higher disease specific mortality |
| Obstructive Pulmonary Disease COPD COPD + Cardiovascular Disease (CVD) | Patients with CVD have higher burden of chronic respiratory symptoms. CVD increases risk of hospitalization and death at any stage of COPD. |
| Obstructive Pulmonary Disease COPD Palliative Care | Only 13 of patients with O2 dependent COPD discuss palliative care with Dr. Patients with COPD are less likely to receive palliative care than other advanced illnesses. Palliative care improves patient satisfaction, decreases hospitalization admissions (36% v 59%), reduces overall costs of care > 50%. |
| Pleural Diseases Pleural Effusion General Characteristics | The accumulation of significant volumes of pleural fluid. May result from inflammation of structures adjacent to the pleural space or lesions within the chest. Small effusions may not cause symptoms and are discovered on routine radiography. About 25% of effusions are associated with malignancy. |
| Pleural Diseases Pleural Effusion 4 Types | 1. Exudates are associated with leaky capillaries. Examples include infection, malignancy, trauma. 2. Transudates (intact capillaries) are associated with increased hydrostatic or decreased oncotic pressure. Examples include CHF, Atelectasis, renal or liver disease (cirrhosis) 3. Empyema is an infection within the pleural space. 4. Hemothorax indicates bleeding into the pleural space, commonly as a result of trauma or malignancy. |
| Pleural Diseases Pleural Effusion Clinical Features | With a small inflammatory effusion, patients are usually asymptomatic. Large or bilateral effusions may lead to dyspnea. A dull to flat percussion note over the area of fluid may be heard with reduced or absent breath sounds. The mediastinum is usually shifted away from the side of the large effusion. |
| Pleural Diseases Pleural Effusion Laboratory FIndings | Radiographic findings include blunting of the costophrenic angle, loss of sharp demarcation of the diaphragm and hear, and mediastinal shift to the uninvolved side. Lateral deficits radiographs can help to identify small effusions and differentiate free-flowing versus loculated fluid. CT may be useful if plain film cannot differentiate between parenchymal and pleural densities. |
| Pleural Diseases Pleural Effusion Laboratory Findings Thoracentesis | Gold standard. Fluid sent for protein, LDH, pH, total WBC and differential cell counts, glucose, cytology and gram stain with culture and sensitivity. |
| Pleural Diseases Pleural Effusion Laboratory Findings Transudates v Exudates | Light's Criteria. Fluid is considered an exudate if it meets any ONE of the following. 1. Pleural fluid protein to serum protein ratio > 0.5 2. Pleural fluid LDH to serum LDH ratio > 0.6 3. Pleural fluid LDH greater than 2/3 the upper limit of normal for serum LDH. |
| Pleural Diseases Pleural Effusion Treatment | Unless the cause has been clearly established, the presence of fluid is an indication for thoracentesis. Transudates pleural effusions resolve when underlying causes are treated. Emphysema requires drainage and antibiotic therapy. |
| Pleural Diseases Pneumothorax General Characteristics | The accumulation of air in the pleural space. The cause may be spontaneous (primary pneumothorax), traumatic, or iatrogenic. Tall, thin males between 10-30 are are greatest risk for primary pneumothorax. Tension pneumothorax is secondary to a sucking chest wound or a pulmonary laceration that allows air to enter the chest with inspiration but does not allow it to leave on expiration. |
| Pleural Diseases Pneumothorax Clinical Features | Characterized by the acute onset of ipsilateral chest pain and dyspnea. Physical findings depend on the size of the pneumothorax and may include unilateral chest expansion, decreased tactile fremitus, hyperresonance, diminished breath sounds. Tension pneumothorax is associated with a mediastinal shift to the contra lateral side and impaired ventilation leading to cardiovascular compromise. |
| Pleural Diseases Pneumothorax Laboratory Findings | CXR reveals the presence of pleural air. A visceral pleural line may be the only evidence of a small pneumothorax. ABG analysis (if done) reveals hypoxemia. |
| Pleural Diseases Pneumothorax Treatment | Depends on Severity Small resolve spontaneously Severely symptomatic or large, chest tube. Tension pneumothorax is medical emergency. Large bore needle should be inserted to allow air to move out of the chest then chest tube. Patients should be followed with CXR every 24 hours until resolved. |
| Pulmonary Circulation Pulmonary Embolism General Characteristics | PE arises from thrombi in the systemic venous circulation or the right side of the heart. More than 90% of pulmonary embolism originate as clots in the deep veins of the lower extremities. Others include air emboli from central lines, amniotic fluid from active labor, and fat from long bone femur fracture. |
| Pulmonary Circulation Pulmonary Embolism Risk Factors | Virchow's triad 1. Hypercoagulable state 2. Venous stasis 3. Vascular inflammation or injury Specific risks include surgical procedures, cancer, oral contraceptives, pregnancy. |
| Pulmonary Circulation Pulmonary Embolism Epidemiology | Approx 50-60% of patients with deep vein thrombosis will experience a PE. Half of those will be asymptomatic. Often, PE is found only on autopsy. Symptomatic PE is a serious and potentially fatal condition. PE is the third leading cause of death in hospitalized patients. |
| Pulmonary Circulation Pulmonary Embolism Clinical Features | Symptoms include pleuritic chest pain, dyspnea, apprehension, cough, hemoptysis, diaphoresis. Signs include tachycardia, tachypnea, crackles, accentuation of the pulmonary compartment of the second heart sound, and a low-grade fever. |
| Pulmonary Circulation Pulmonary Embolism Laboratory Findings ABG | Measurements show acute respiratory alkalosis secondary to hyperventilation |
| Pulmonary Circulation Pulmonary Embolism Laboratory Findings Electrocardiography | Shows tachycardia and nonspecific ST-T wave changes. The classic S1Q3T3 pattern, indicating corpulmonale, is seen in fewer than 20% of patients with symptomatic PE. |
| Pulmonary Circulation Pulmonary Embolism Laboratory FIndings CXR | May show nonspecific abnormalities such as basilar Atelectasis. The main purpose of getting a CXR is to rule out other abnormalities and aid in interpreting a ventilation/perfusion scan. |
| Pulmonary Circulation Pulmonary Embolism Laboratory Findings Ventilation - Perfusion Scan | Shows perfusion defects with normal ventilation. A normal scan rules out clinically significant thromboembolism. Nondiagnostic scans warrant further testing. |
| Pulmonary Circulation Pulmonary Embolism Laboratory Findings Pulmonary Angiography | Remains the definitive test for diagnosis but is reserved for cases in which the diagnosis is uncertain after noninvasive testing. |
| Pulmonary Circulation Pulmonary Embolism Laboratory Findings D-dimer | May be useful to rule out PE if clinical suspicion is low and D-dimer is negative. |
| Pulmonary Circulation Pulmonary Embolism Laboratory FIndings Spiral CT | Initial method of identifying pulmonary embolus |
| Pulmonary Circulation Pulmonary Embolism Treatment | Anti coagulation therapy is initiated. Heparin is the anticoagulant of choice. Low molecular weight heparin or warfarin is continued after the acute phase. Duration of therpay depends on clinical situation. Filter is helpful in patients at high risk for recurrence who are unable to tolerate anticoagulants. High Risk Patients: Early ambulation, Intermittant pneumatic compression stockings |
| Pulmonary Circulation Pulmonary Hypertension General Characteristics | Present when the pulmonary arterial pressure rises to a level inappropriate for a given cardiac output. Once present, it is self-perpetuating. Primary HTN is rare and has a fatal outcome. Secondary HTN has many causes that develop as a result of obliteration and obstruction of the pulmonary arterial tree. Hypoxia is the most important and potent stimulus of pulmonary arterial vasoconstriction. Other causes include acidosis and veno-occlusive conditions. |
| Pulmonary Circulation Pulmonary Hypertension Clinical Features | Dyspnea, retrosternal chest pain, weakness, fatigue, edema, sacites, cyanosis, syncope. Signs may include marrow splitting and accentuation of the second heart sound and systolic ejection click. |
| Pulmonary Circulation Pulmonary Hypertension Laboratory Findings CXR | May show enlarged pulmonary arteries. |
| Pulmonary Circulation Pulmonary Hypertension laboratory Findings Electrocardiography | May show right ventricular hypertrophy, atrial hypertrophy, and right ventricular strain. May be useful in estimating pulmonary arterial pressure, but right heart catheterization offers more precise hemodynamic monitoring. |
| Pulmonary Circulation Pulmonary Hypertension Treatment | Treatment of primary pulmonary HTN may include chronic oral anticoagulants, calclum channel blockers to lower systemic arterial pressure and prostacyclin (a potent pulmonary vasodilator). Heart-lung transplant is usally needed. Treatment of secondary pulmonary HTN consists of treating the underlying disorder in addition to anticoagulants. |
| Restrictive Pulmonary Disease Idiopathic fibrosis interstitial pneumonia General Characteristics | This is the most common diagnosis among patients with interstitial lung disease. There are three histologic patterns with different natural histories and treatments. 1. Usual interstitial pneumonia 2. Respiratory bronchiolitis associated interstitial lung disease 3. Acute interstitial pneumonitis |
| Restrictive Pulmonary Disease Idiopathic fibrosis interstitial pneumonia Clinical FIndings | Symptoms include insidious dry cough, exertion all dyspnea, fatigue, malaise. Examination may reveal clubbing and inspiratory crackles. |
| Restrictive Pulmonary Disease Idiopathic fibrosis interstitial pneumonia Laboratory FIndings CXR | Demonstrates evidence of progressive fibrosis over several years |
| Restrictive Pulmonary Disease Idiopathic fibrosis interstitial pneumonia Laboratory Findings CT | Shows diffuse, patchy fibrosis with pleural based honeycombing. |
| Restrictive Pulmonary Disease Idiopathic fibrosis interstitial pneumonia PFTs | May show restrictive pattern (decreased lung volume with a normal to increased FEV1/FVC ratio) |
| Restrictive Pulmonary Disease Idiopathic fibrosis interstitial pneumonia Treatment | Controversial. None has been shown to improve survival or quality of life compared to no treatment. |
| Restrictive Pulmonary Disease Pneumoconioses General Characteristics | Chronic fibrotic lung diseases caused by the inhalation of coal dust or various inert, inorganic, or silicate dusts. Clinically important because include coal workers pneumoconiosis, silicosis, and asbestosis. |
| Restrictive Pulmonary Disease Pneumoconioses Asbestosis | Occupation: Insulation, demolition, construction Diagnosis: Bx asbestos bodies Complications: Increased risk of lung cancer and mesothelioma, especially if a smoker. |
| Restrictive Pulmonary Disease Pneumoconioses Coal workers' pneumoconiosis | Occupation: Coal mining Diagnosis: CXR nodular opacities at upper lung fields Complications: Progressive massive fibrosis |
| Restrictive Pulmonary Disease Pneumoconioses Silicosis | Occupation: Mining, sand blasting, quarry work, stone work Diagnosis: CXR nodular opacities at upper lung fields Complications: Increased risk of TB; progressive massive fibrosis. |
| Restrictive Pulmonary Disease Pneumoconioses Berryliosis | Occupation: High tech fields, aerospace, nuclear power, ceramics, foundries, tool and die manufacturing. Diagnosis: CXR diffuse infiltrates and hilar adenopathy Complications: Requires chronic steroids |
| Restrictive Pulmonary Disease Pneumoconioses Clinical Features | In simple cases, usually asymptomatic. In complicated cases patients have dyspnea, inspiratory crackles, clubbing, and cyanosis. |
| Restrictive Pulmonary Disease Pneumoconioses Laboratory Findings PFTs | Show restrictive dysfunction and reduced diffusing capacity. |
| Restrictive Pulmonary Disease Pneumoconioses Laboratory Findings Chest radiography | Coal Workers' pneumoconiosis: small opacities are prominent in the upper lung fields Silicosis: Small rounded opacities are seen throughout the lung and hilar lymph nodes may be calcified. Asbestosis: Interstitial fibrosis, thickened pleura, calcified plaques appear on the diaphragm or later chest wall. |
| Restrictive Pulmonary Disease Pneumoconioses Treatment | Treatment is primarily supportive as no effective treatment is available. Supportive therapy includes O2, vaccinations (pneumovax, influenza), and rehabilitation. Corticosteroids may relieve the chronic alveoli tis of silicosis. Smoking cessation is equally important for patients with asbestosis because soling intereferes with short asbestos fiber clearance from the lung. Smoking and asbestos are linked synergistically to lung cancer. |
| Restrictive Pulmonary Disease Sarcoidosis General Characteristics | Sarcoidosis is a multi organ disease of idiopathic cause. Characterized by noncaseating Granulamatous inflammation in affected organs. Approximately 90% have lung involvement. Incidence is highest in North American blacks (esp. Women) and Northern European whites. |
| Restrictive Pulmonary Disease Sarcoidosis Clinical Features | Common respiratory symptoms include cough, dyspnea of insidious onset, chest discomfort. Patients may present with malaise, fever and symptoms consistent with the he involvement of various organs. Extra pulmonary findings are common and include erythema nodosum or enlargement of parotid glands., lymph nodes, liver or spleen. |
| Restrictive Pulmonary Disease Sarcoidosis Laboratory Findings Serum Blood Tests | May show leukopenia, eosinophilia, elevated erythrocyte sedimentation rate, hypercalcemia, hypercalciuria. ACE levels are legates in 40-80% of patients. |
| Restrictive Pulmonary Disease Sarcoidosis Laboratory Findings Radiographic | Demonstrate bilateral hilar and right parathracheal adenopathy and bilateral diffuse reticular infiltrates. |
| Restrictive Pulmonary Disease Sarcoidosis Laboratory Findings Transbronchial biopsy or Fine needle biopsy | Confirms diagnosis. Biopsy shows noncaseating granulomas. |
| Restrictive Pulmonary Disease Sarcoidosis Treatment | Approximately 90 of cases are responsive to corticosteroids and can be controlled with modest maintenance doses. |
| Acute (adult) Respiratory Distress Syndrome (ARDS) General Characteristics | Three clinical setting account for 75% of ARDS. 1. Sepsis (most important) 2. Severe multiple trauma 3. Aspiration of gastric contents Other causes include shock, toxic inhalation, near-drowning, multiple transfusions. The underlying abnormality is increased permeability of the alveolar capillary membranes which leads to development of protein-rich pulmonary edema. |
| Acute (adult) Respiratory Distress Syndrome (ARDS) Clinical features | Rapid onset of dyspnea occurring 12-24 hours after the precipitating event. Physical exam shows tachypnea, frothy pink or red sputum, and diffuse crackles. Many patients are cyanotic with increasingly severe hypoxemia that is refractory to administered oxygen. |
| Acute (adult) Respiratory Distress Syndrome (ARDS) Laboratory Findings CXR | Maybe normal at first. Infiltrates tend to be peripheral (spares the costophrenic angles) with are bronchograms in 80% of patients. The heart is normal in size. Upper lung venous engorgement is uncommon. Pleural effusions are small to absent. |
| Acute (adult) Respiratory Distress Syndrome (ARDS) Laboratory FIndings | Pulmonary capillary wedge pressure is normal. Multiple organ failure is common. |
| Acute (adult) Respiratory Distress Syndrome (ARDS) Treatment | Includes identification and specific treatment of underlying precipitating and secondary conditions. Supportive care required to compensate for the severe respiratory dysfunction. O2 should be delivered via endo tracheal intubation with positive pressure ventilation and low levels of positive and end-expiratory pressure (PEEP). Hypoxia is often refractory to treatment. Mortality rate is high. 1/3 of deaths occur withing 3 days of onset of symptoms. Remaining deaths within 2 weeks of diagnosis and are caused by infection and multiple organ failure. |
| Aspiration of Foreign Bodies General Characteristics | May be of gastric contents, inert material, poorly chewed food. Degree of injury depends on the substance aspirated. |
| Aspiration of Foreign Bodies Clinical Features | An episode of choking and coughing or unexplained wheezing or hemoptysis should raise the suspicion of foreign body aspiration. Asphyxia may result from the aspiration of osbstructing material. Pneumonia may develop secondary to aspiration of toxic materials. Acute gastric aspiration is one of the most common causes of ARDS. |
| Aspiration of Foreign Bodies Laboratory FIndings | Expiratory radiography may reveal regional hyperinflation caused by a check valve effect |
| Aspiration of Foreign Bodies Treatment | Bronchoscopy may help establish the diagnosis but also can be the treatment of choice for removal of the object. Cultures should be obtained if post obstructive pneumonia is suspected. |
| Hyaline membrane disease General Characteristics | The most common cause of respiratory disease in the preterm infant. It is caused by a deficiency of surfactant. |
| Hyaline Membrane Disease Clinical Features | The infant will demonstrate typical signs of respiratory distress |
| Hyaline Membrane Disease Laboratory Findings | CXR demonstrates air bronchograms, diffuse bilateral atelectasis causing a ground glass appearance and coming of the diaphragm. |
| Hyaline Membrane Disease Treatment | Synchronized intermittent mandatory ventilation should be used. Administration of exogenous surfactants can be used in the delivery room as prophylaxis or as rescue in established hyaline membrane disease. |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.