2605430
Description
Mind Map by Annie Nguyen, updated more than 1 year ago
|
|
Created by Annie Nguyen
over 9 years ago
|
|
Dermatology
- Pityriasis Rosea
- Who:
young,
female
- Why: mild,
acute,
inflammation
- When: Spring and Fall. Herald
Patch- 1-2 weeks before
eruption. Eruptions last 6-8
weeks.
- What: mild
itching, 2 cm fawn
colored plaques.
• 2 cm diameter;
fawn colored
plaques; with a
crinkled center
and collarated
scale
- No treatment: self-limiting.
Moderate- triamcinolone
crm. Severe: UVB treatment
or prednisone
- DDX: 1. Syphillis- palmar,
planter, mucosa
lesions-serology or RPR: rapid
plasma ragin. 2. Tinea
Corporis- few; red scaly
plaques. 3. Seborrheic
Dermatitis- poorly
demarcated patches on the
body(sternum, groin, and
pubic). Tinea versicolor- lacks
collarette rim.
- Who:
young,
female
- Malignant
Melanoma
- Where:
Primary
malignant
melanomas
- 1. lentigo
maligna
melanoma
(chronically
sun-exposed skin
of older
individuals)
- 2. superficial spreading
malignant melanoma
(two-thirds of all
melanomas arising on
intermittently
sun-exposed skin);
- 3. nodular
malignant
melanoma
ease.
- 4.
acral-lentiginous
mela-nomas
(arising on palms,
soles, and nail
beds);
- 5. ocular
melanoma
- 6. malignant
melanomas on
mucous
membranes.
- 1. lentigo
maligna
melanoma
(chronically
sun-exposed skin
of older
individuals)
- Who: Older- lentigo
maligna; Men, White-
superficial
spreading,
Dark-skin- hesitancy
to Biospy- Acral
Lentiginous
- What: pigmented
lesions suspicious
for melanoma are
an irregular
notched border
where the pigment
appears to be
leaking into the
normal surrounding
skin; See note
Annotations:
- a topography that may be irregular, ie, partly raised and partly flata topography that may be irregular, ie, partly raised and partly flatColor variegation is present, and colors such as pink, blue, gray, white, and black are indications for referral. A useful mnemonic is the ABCD rule: “ABCD = Asymmetry, Border irregularity, Color variegation, and Diameter > 6 mm.” “E” for Evolution can be added. The history of a changing mole (evolution) is the single most important historical reason for close evaluation and possible referral. Bleeding and ulcer-ation are ominous signs. A mole that stands out from the patient’s other moles deserves special scrutiny—the “ugly duckling sign.” A patient with a large number of moles is statistically at increased risk for melanoma and deserves careful and periodic examination, particularly if the lesions are atypical. Referral of suspicious pigmented lesions is always appropriate.
- How: Treatment of
melanoma consists of
excision. After
histologic diagnosis,
the area is excised
with margins dictated
by the thickness of the
tumor. See Note
Annotations:
- Sentinel lymph node biopsy using preoperative lymph scintigraphy and intra-operative lymphatic mapping for staging melanoma patients with intermediate risk without clinical adenopathy. Patients with lesions over 1 mm in thickness or with high-risk histologic features. Referral of intermediate-risk and high-risk patients to centers with expertise The long-term use of beta-blockers may reduce the risk of prog
- Where:
Primary
malignant
melanomas
- Atopic Dermatitis
- WHO: family HX allergic
manifestations (eg,
asthma, allergic rhinitis,
atopic dermatitis). `
Onset in childhood
Annotations:
- in most patients. Onset after age 30 is very uncommon.
- WHAT: Chronic
itching may be
severe and
prolonged. Rough,
red plaques thin
scale and poor
demarcation
Annotations:
- dermatitis must include pruritus, typical morphology and distribution (flexural lichenification, hand eczema, nipple eczema, and eyelid eczema in adults), onset in childhood, and chronicity. Also helpful are: (1) a personal or family history of atopic disease (asthma, allergic rhinitis, atopic dermatitis), (2) xerosis-ichthyosis, (3) facial pallor with infraorbital darkening, (4) elevated serum IgE, and (5) repeated skin infections.
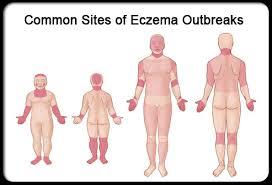
- WHERE: The flexural
surfaces of elbows and
knees are often
involved. Face, neck,
upper trunk, wrists,
and hands and in the
antecubital and
popliteal folds. `
Annotations:
- In black patients with severe disease, pigmentation may be lost in lichenified areas. During
- In chronic
cases, the skin
is dry, leathery,
and lichenified.
a
- Acute flares,
widespread
redness with
weeping, either
diffusely or in
discrete
plaques, is
common.
- HOW: hyperirritable
skin. avoid anything that
dries or irritates the skin,
low humidity (worse in
the winter). bathe once
daily and
immediatelyovered with
a thin film of an
emollient
Annotations:
- Soap should be confined to the armpits, groin, scalp, and feet. Washcloths and brushes should not be used. After rinsing, the skin should be patted dry (not rubbed) and thenemollient such as Aquaphor, Eucerin, petrolatum, Vanicream, or a corticoste-roid as needed. Vanicream can be used if contact dermati-tis resulting from additives in medication is suspected.p.99
- WHY:
hyperirratible;
autoImmune
- DDX-
Psoriasis:
Rough, red
plaques
usually
without the
thick scale
and discrete
demarcation
of psoriasis
Annotations:
- Atopic dermatitis must be distinguished from seborrheic dermatitis (less pruritic, frequent scalp and face involve-ment, greasy and scaly lesions, and quick response to therapy). Secondary staphylococcal infections may exacer-bate atopic dermatitis, and should be considered during hyperacute, weepy flares of atopic dermatitis. Fissuring where the earlobe connects to the neck is a cardinal sign of secondary infection. Since virtually all patients with atopic dermatitis have skin disease before age 5, a new diagnosis of atopic dermatitis in an adult over age 30 should be made cautiously and only after consultation.p.99
- WHO: family HX allergic
manifestations (eg,
asthma, allergic rhinitis,
atopic dermatitis). `
Onset in childhood
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.