7462981
Description
Mind Map by Jessica Way, updated more than 1 year ago
|
|
Created by Jessica Way
almost 8 years ago
|
|
Ischemic Stroke
- TRANSIENT ISCHEMIC ATTACK (TIA)
- An episode of neurological dysfunction
WITHOUT infarction of the brain. TIA can be
a warning sign for future stroke (Lewis et al, 2014).
- An episode of neurological dysfunction
WITHOUT infarction of the brain. TIA can be
a warning sign for future stroke (Lewis et al, 2014).
- THROMBOTIC STROKE
- Occurs from injury to a blood vessel wall, clot
formation and if clot leads to total occlusion of the
blood vessel then infarction and cell death will
occur (Lewis et al, 2014).
- Occurs from injury to a blood vessel wall, clot
formation and if clot leads to total occlusion of the
blood vessel then infarction and cell death will
occur (Lewis et al, 2014).
- EMBOLIC STROKE
- Occurs when an embolus blocks a cerebral
artery and results in infarction. Emboli
usually originates in inner layer of heart and
then travels into cerebral circulation (Lewis et al, 2014).
- Occurs when an embolus blocks a cerebral
artery and results in infarction. Emboli
usually originates in inner layer of heart and
then travels into cerebral circulation (Lewis et al, 2014).
- MRI- MAGNETIC RESONANCE IMAGING
- Determines extent of brain
injury (Lewis et al, 2014).
- Determines extent of brain
injury (Lewis et al, 2014).
- HYPERTENSION
- Hypertension is the #1 risk factor for
developing stroke as it causes the development
of atherosclerotic plaque buildup, narrowing
the lumen of the arteries. The more narrow the
lumen the higher chance there is of clots
obstructing the lumen leading to ischemic
stroke (Sacco et al, 1997).
- Hypertension is the #1 risk factor for
developing stroke as it causes the development
of atherosclerotic plaque buildup, narrowing
the lumen of the arteries. The more narrow the
lumen the higher chance there is of clots
obstructing the lumen leading to ischemic
stroke (Sacco et al, 1997).
- HEART DISEASE: MI,
Atrial Fibrillation,
Carotid Stenosis, and
valve diseases
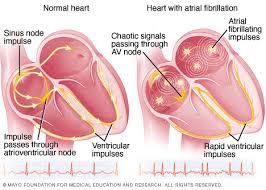
- ATRIAL FIBRILLATION
- With Atrial Fibrillation the atria contract irregularly and at a rapid
rate it causes blood to pool in the atria causing clots to form on
the heart walls. These clots can dislodge from the heart wall
entering the circulation and travel to the brain to cause a stroke.
A Fib patients are at extremely HIGH risk of stroke. Early
detection of A FIb and proper drug therapy of anticoagulants is
recommended to prevent stroke (Shorten, 2014).
- With Atrial Fibrillation the atria contract irregularly and at a rapid
rate it causes blood to pool in the atria causing clots to form on
the heart walls. These clots can dislodge from the heart wall
entering the circulation and travel to the brain to cause a stroke.
A Fib patients are at extremely HIGH risk of stroke. Early
detection of A FIb and proper drug therapy of anticoagulants is
recommended to prevent stroke (Shorten, 2014).
- ATRIAL FIBRILLATION
- SMOKING
- DIABETES
- Increases
development of
atherosclerotic
plaque buildup and
obesity (Sacco et al,
1997)
- Increases
development of
atherosclerotic
plaque buildup and
obesity (Sacco et al,
1997)
- ABDOMINAL OBESITY AND
LIMITED PHYSICAL
ACTIVITY
- Increases risk of HTN, diabetes
and atherosclerosis (Sacco et
al, 1997)
- Increases risk of HTN, diabetes
and atherosclerosis (Sacco et
al, 1997)
- ILLICIT DRUG USE
- Cocaine,
Methamphetamine,
and Heroin
- Cocaine,
Methamphetamine,
and Heroin
- CT: COMPUTED TOMOGRAPHY
- Indicates the size and location of the
lesion and helps to quickly identify the
type of stroke (Lewis et al, 2014).
- Indicates the size and location of the
lesion and helps to quickly identify the
type of stroke (Lewis et al, 2014).
- CTA: COMPUTED TOMOGRPHY ANGIGRAPHY
- Estimates perfusion and detects
any DEFECTS in the cerebral
arteries (Lewis et al, 2014).
- Estimates perfusion and detects
any DEFECTS in the cerebral
arteries (Lewis et al, 2014).
- ANGIOGRAPHY
- Can determine occlusions,
atherosclerotic plaque and malformed
vessels...RISK OF DISLODGING CLOT
(Lewis et al, 2014).
- Can determine occlusions,
atherosclerotic plaque and malformed
vessels...RISK OF DISLODGING CLOT
(Lewis et al, 2014).
- TRANCRANIAL DOPPLER
- Measures the velocity of
blood flow in the cerebral
arteries (Lewis et al, 2014).
- Measures the velocity of
blood flow in the cerebral
arteries (Lewis et al, 2014).
- BLOOD TESTS
- Helps to identify underlying
conditions leading to stroke
(Lewis et al, 2014).
- Helps to identify underlying
conditions leading to stroke
(Lewis et al, 2014).
- Right
Hemisphere
- Hemiplagia to left side (left
sided neglect), Spatial/
perceptual deficits, denial of
any problems, RAPID
performance but SHORT
attention span, impulsive,
impaired judgment and
impaired concept of time.
(Lewis, Heitkemper, Dirksen,
Bucher, Camera, 2014)
- Hemiplagia to left side (left
sided neglect), Spatial/
perceptual deficits, denial of
any problems, RAPID
performance but SHORT
attention span, impulsive,
impaired judgment and
impaired concept of time.
(Lewis, Heitkemper, Dirksen,
Bucher, Camera, 2014)
- Left Hemisphere
- Impaired Speech
and Language
(APHASIAS)
- Expressive
Aphasia:
Difficulty
EXPRESSING
thoughts
- Receptive
Aphasia:
Difficulty
UNDERSTANDING
- Anomic/ Amnesic
Aphasia: unable to find
names for specific
objects and people
- Global
Aphasia: loss
of ALL
receptive and
expressive
abilities
- Expressive
Aphasia:
Difficulty
EXPRESSING
thoughts
- Hemiplagia to the right side
(impaired right to left
differentiation), slow
performance and cautious,
very aware of deficits (can
cause anxiety and depression),
impaired comprehension of
language and math (Lewis,
et al., 2014)
- Impaired Speech
and Language
(APHASIAS)
- Ineffective Airway Clearance
- Demonstrates effective coughing and maintains a clear airway
- Encourage slow, deep
breathing, turning and
coughing (Lewis et al, 2014).
- Patient in sitting
position (Lewis et al,
2014).
- NPO until SLP
swallow
assessment (Lewis
et al, 2014).
- Oxygenation (Lewis et
al, 2014).
- Suctioning as
Needed (Lewis et
al, 2014)
- Encourage slow, deep
breathing, turning and
coughing (Lewis et al, 2014).
- Demonstrates effective coughing and maintains a clear airway
- Impaired Verbal Communication
- Effective use of oral and written communication techniques
- Simple words
and short
sentences
(Lewis, et al.,
2014)
- Alternative
Communication
Aids(Lewis, et al.,
2014)
- LISTEN ATTENTIVELY
AND ALLOW TIME
FOR RESPONSE (Lewis,
et al., 2014)
- Simple words
and short
sentences
(Lewis, et al.,
2014)
- Effective use of oral and written communication techniques
- Impaired Swallowing
- No choking, coughing or aspiration
- HOB = 90 degrees
or as close as
possible (Lewis et al, 2014).
- Chin Tuck
Positioning when
eating (Lewis et
al, 2014).
- Remain Sitting for 30 MINUTES
after ALL meals to prevent
aspiration (Lewis et al, 2014).
- Check for pocketing and
perform mouth care AC
(Lewis et al, 2014).
- NG tube with 30 degree HOB, within
3-4 days of stroke, continued until
swallowing assessment deems
patient safe (Srigresh,
Radhakrishnan, Umamaheswara
Rao, 2014)
- HOB = 90 degrees
or as close as
possible (Lewis et al, 2014).
- No choking, coughing or aspiration
- Preventative Collaborative Care
- HEALTH MANAGEMENT
- Includes: limited alcohol
use, cessation of smoking,
proper diet and exercise,
blood glucose control and
BP control (Lewis et al,
2014)
- Includes: limited alcohol
use, cessation of smoking,
proper diet and exercise,
blood glucose control and
BP control (Lewis et al,
2014)
- PREVENTATIVE DRUG THERAPY
- Antiplatelet Therapy
- ASA- Aspirin
(81-325mg/day)
- Loading dose of atleast
160 should be given to all
patients not already on
antiplatelets. (Candadian
Stroke Strategy, 2010)
- Loading dose of atleast
160 should be given to all
patients not already on
antiplatelets. (Candadian
Stroke Strategy, 2010)
- Clopidogrel- Plavix
- Warfarin- Coumadin: given to
patients with A Fib and previous Hx
of TIA
- ASA- Aspirin
(81-325mg/day)
- Antiplatelet Therapy
- PREVENTION SURGERY
- Transluminal
Angioplasty: inserting a
balloon to open
narrowed artery to
improve blood flow and
prevent future stroke
(Lewis et al, 2014).
- Transluminal
Angioplasty: inserting a
balloon to open
narrowed artery to
improve blood flow and
prevent future stroke
(Lewis et al, 2014).
- HEALTH MANAGEMENT
- Acute Collaborative Care
- Oxygen Administration, artificial airway,
intubation and mechanical ventilation if
indicated (Lewis, et al., 2014)
- O2 Sat <92% O2 set to 2-4l/min. If
92% can't be maintained than ABG's
and chest radiograph are
recommended. (Summers, et al.,
2009)
- O2 Sat <92% O2 set to 2-4l/min. If
92% can't be maintained than ABG's
and chest radiograph are
recommended. (Summers, et al.,
2009)
- ACUTE DRUG THERAPY
- tPA- Tissue
Plasminogen Activator
(Alteplase)
- CT or MRI
needed BEFORE
administering
tPA
- Patients eligible for tPA should
have CT scan within 25 mins of
admittance. (Summers, Leonard,
Wentworth, Saver, Simpson,
Spilker, Hock, Miller, Mitchell,
2009)
- Patients eligible for tPA should
have CT scan within 25 mins of
admittance. (Summers, Leonard,
Wentworth, Saver, Simpson,
Spilker, Hock, Miller, Mitchell,
2009)
- Administered
within 4.5 hours of
clinical symptoms
(Canadian Stroke
Strategy, 2010)
- Ideally, within 60 mins after admittance to
hospital. (Cavalcante, Moreira, Guedes,
Araujo, Lopes, Damasceno, Lima, 2009).
Total dose: 09.mg/kg with 10 percent (0.09
mg/kg) given as IV BOLUS, and remaining
90% (0.81 mg/kg) given as IV infusion over
60 minutes (Canadian Stroke Strategy, 2010)
- Ideally, within 60 mins after admittance to
hospital. (Cavalcante, Moreira, Guedes,
Araujo, Lopes, Damasceno, Lima, 2009).
Total dose: 09.mg/kg with 10 percent (0.09
mg/kg) given as IV BOLUS, and remaining
90% (0.81 mg/kg) given as IV infusion over
60 minutes (Canadian Stroke Strategy, 2010)
- NO ANTIPLATELET
MEDS GIVEN
WITHIN 24 HOURS
of tPA. (Lewis, et al.,
2014)
- Monitor for
manifestations
of bleeding.
(Lewis, et al.,
2014)
- CT or MRI
needed BEFORE
administering
tPA
- Warfarin-Coumadin:
indicated once patient has
stabilized (after 24 hours).
(Lewis, et al., 2014)
- IV Metoprolol: SBP
>220mmHg and DBP
> 130mmHg
- tPA- Tissue
Plasminogen Activator
(Alteplase)
- Oxygen Administration, artificial airway,
intubation and mechanical ventilation if
indicated (Lewis, et al., 2014)
- Psychosocial
- Family Role Alteration due to Decreased
Functionality (Lewis et al, 2014).
- In 30% of stroke patients: depression,
anxiety, fatigue and apathy are
neuropsychiatric outcomes of stroke
(Hackett, Kohler, O'brien & Mead, 2014).
- Post - Stroke Depression (PSD): Causes a decrease in patient
participation in rehabilitiation during the most crucial time of
recovery to prevent negative outcomes. As nurses we should
be monitoring and assessing for symptoms of PSD to prevent
poor outcomes. Early detection, correct diagnosis and
appropriate treatment of PSD increases the chances of good
outcomes after a stroke (Matsuzaki et al, 2015).
- Less common Neuropsychiatric outcomes of
stroke include: emotional liability, personality
changes and psychosis. These are less
common symptoms but are much more
challenging to manage (Hackett, Kohler,
O'brien & Mead, 2014).
- Discharge planning: involve family members/caregivers in
post stroke treatement planning and needs assessment,
enhance their knowledge of illness and encourgae them to
participate in rehabilitation sessions and care. Secondary
prevention education for patients, and link to social
supports and rehab. (Cavalcante, et. al, 2011)
- Family Role Alteration due to Decreased
Functionality (Lewis et al, 2014).
- Non- Modifiable: Previous
family history of stroke,
increased risk if of African
American ethnicity, it is more
common in men but more
fatal in women, and people
over the age of 55 are at
increased risk of stroke
(Lewis et al, 2014)
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.