Description
|
|
Created by jessica.wilson1
about 10 years ago
|
|
Page 1
Speech: the motor act of verbal expressionThe Five Subsystems of Speech:1. Respiration2. Phonation3. Resonance4. Articulation5. Prosody
Dysarthria - Defining Characteristics It is a group of speech disorders caused by disturbances of neuromuscular control of the speech production systems A disruption to the execution of speech movements It can result from underlying neuromuscular disturbances to muscle tone, reflexes and kinematic aspects of movement, such as speed, range, accuracy and steadiness Generally more consistent in its errors and amount of intelligibility compared to apraxic speech
Seven Types of Dysarthria Spastic Dysarthria Flaccid Dysarthria Hypokinetic Dysarthria Hyperkinetic Dysarthria Ataxic Dysarthria Unilateral UMN Dysarthria Mixed Dysarthrias
Assessment MethodsPerceptual: listening; audio visual and tactileAcoustic: measurement of speechPhysiologic: measurement of physiological processes (electrical measurement)
SPASTIC DYSARTHRIA
Quick Overview: associated with bilateral damage that affects the UMN - direct and indirect activation pathways of the CNS this means the PYRAMIDAL and EXTRAPYRAMIDAL motor pathways Px has increased muscle tone (spasticity) Weakness Reduced speed and range and force of movements Hyperreflexes Can be a result of bilateral lesions in the motor cortex and its pathway to the LMN that are responsible for muscle contraction
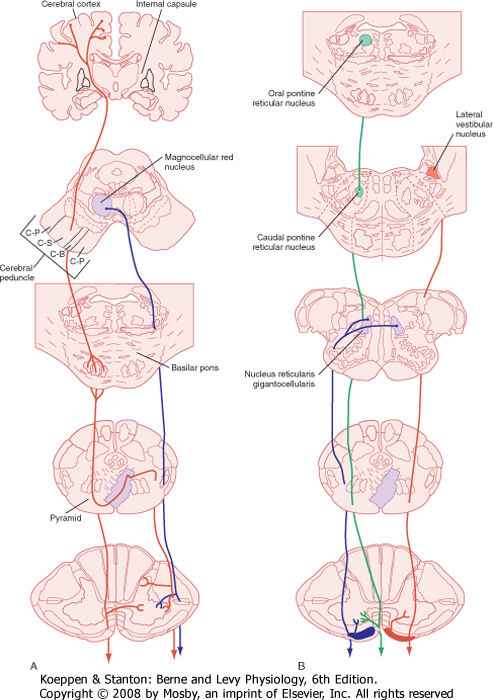
Pyramidal Descending Motor Pathway Motor impulses at the cortical level Corticospinal and corticobulbar tract Controls speech movements, which are discrete and skilled movements Works at a conscious level - voluntary movements Direct Pathway - this is because its axons descend without synapsing from the pyramidal neurones to the spinal cord Large neurons with long axons that project into the spinal cord Control the precise or skilled voluntary movements of our skeletal muscles If damaged: Leads to weakness and slowness of movements Further info: the pyramidal cells that control foot movements are in one place and those that control hand movements are in another
Extrapyramidal Descending Motor Pathway Motor impulses in the cerebral cortex Rubrospinal, reticulospinal, vestibulospinal and tectospinal tract These pathways are involved in: Maintaining posture Regulation of reflexes Monitoring muscle tone More unconscious and therefore involuntary motor control Indirect Pathway - this is because they project to influence the activity of most extrapyramidal nuclei Involved in: maintaining balance and posture controlling coarse limb movement head, neck and eye movements that follow objects in the visual field If damaged: Weakness of movements Spasticity Abnormal reflex movements
{kind=link}
{kind=link}
PresentationMay affect one or a combination of: Respiration Phonation Resonance Articulation Prosody
Diagnosis of spastic dysarthria = bilateral damage to UMN Unilateral UMN damage = Upper Motor Neuron Dysarthria - generally less severe due to bilateral CN innervation THEREFORE: Result of combined effects of: Bilateral damage to pyramidal motor tracts Bilateral damage to extrapyramidal motor tracts THIS THEN LEADS TO: Weakness Slowness Spasticity Abnormal reflexes
AETIOLOGIESThose conditions that can impede the function of UMN of DESCENDING pathways BILATERALLYThese include: Degenerative conditions (MND, MSA etc) Degenerative causes make up the largest group Spastic dysarthria may be evident if degeneration begins in the UMN Vascular (CVA, anoxia) CVA need to be at brainstem to cause bilateral damage, multiple CVA in both hemispheres or one CVA in one hemisphere plus pre-existing condition in other hemisphere Vascular dementia can also cause spastic dysarthria Idiopathic causes Congential Traumatic (TBI) Demyelinating Conditions (MS)
CLINICAL CHARACTERISTICS The weakness and spasticity we can see in the Px speech may also present elsewhere in the body Keep in mind their gag reflex might be hypersensitive, but this is generally a redundant procedure Babinski Reflex - this may reappear even though previously diminished. Px toes may curl up if bilateral damage Jaw Jerk Reflex - this is only carried out on Px suspected of having neurological damage and is an indicator of spastic dysarthria
DYSPHAGIA may be present Px may be able to swallow food, but chewing may take a long time Due to reduced swallowing frequency and control over saliva secretion, there may be drooling
LABILITY Px may be emotionally labile Excessive and uncontrollable laughter or crying
CLONUSShivering or rapid tremor-like appearance
ORO-MOTOR Slow movements Symmetrical appearance of structures
IMPACT ON SPEECHAccording to Duffy, spastic dysarthria will most likely impact all speech systems, as it is associated with impaired patterns of movement that use muscle groups and not just individual musclesDAB - MOST COMMON CHARACTERISTICS Imprecise consonants Monopitch Reduced stress Harsh voice quality Monoloudness Low pitch Slow rate Hypernasality Strained-strangled voice quality Short phrases Distorted vowels Pitch breaks Breathy voice Excess and equal stress REMEMBER: You can't rely on the presence of one of these features to make a differential diagnosis; look for clusters or patterns of features
CLUSTERS
CLUSTER ONE: PROSODIC EXCESS Result of slowness of repetitive movements that are associated with speech Evident when there is: Excess and equal stress Slow rate of speech
CLUSTER TWO: ARTICULATORY-RESONATORY INCOMPETENCE Result of the decreased range and force of movement by the articulators Evident when there is: Imprecise consonants Distorted vowels Hypernasality
CLUSTER THREE: PROSODIC INSUFFICIENCY It is the reduced ability to vary the patterns of movement (in speech) This is apparent through: Monopitch Monoloudness Reduced stress Short phrases
CLUSTER FOUR: PHONATORY STENOSIS When there is over-adduction of the vocal chords as as result of spasticity This is apparent due to: low pitch harshness strained-strangled voice pitch breaks short phrases slow rate
{kind=link}
IMPACT ON THE SPEAKER
PERSONAL IDENTITYSomebody who has had a bilateral stroke may also have cognitive deficits, therefore they may be unaware of their limitations
WHAT THE PATIENT MIGHT TELL YOU ABOUT THEIR SPEECH
Speech might be slow or effortful Speaking against resistance Speech will deteriorate when patient becomes fatigued May need to speak slower Speech may be nasalised Swallowing difficulties and drooling Emotional lability
INTRO
SPASTIC DYSARTHRIA
SPASTIC DYSARTHRIA - CHARACTERISTICS
Want to create your own Notes for free with GoConqr? Learn more.