12707028
Description
Quiz by Plymouth Med, updated more than 1 year ago
|
|
Created by Plymouth Med
over 6 years ago
|
|
Question 1
Question
A middle-aged man with longstanding Barrett’s esophagus is referred for specialist review after he reports increasing dysphagia over the last 4 months. He has noted that it initially only affected solids but now struggles with liquids as well.
What is the next most important investigation to aid diagnosis?
Answer
-
Blood investigation for tumour markers
-
Barium swallow
-
CT
-
PET
-
Endoscopy
Question 2
Question
What is the first line maintenance treatment for Ulcerative Collitis?
Answer
-
Mesalazine
-
Ciclosporin
-
Prednisolone
-
Infliximab
-
Azathioprine
Question 3
Question
What do parietal cells produce?
Answer
-
pepsinogen
-
somatostatin
-
gastrin and histamine
-
hydrochloric acid and intrinsic factor
-
histamine only
Question 4
Question
An elderly man with a history of alcohol abuse goes to ED
with hematemesis for 1 day. He has no abdominal or chest pain. His eyes are reddened and he admits to drinking heavily the
night before he vomited several times. What may be the reason for this?
Answer
-
Oesophageal varices
-
Lung Cancer
-
Achalasia
-
Perforated gastric ulcer
-
Mallory-Weiss tear
Question 5
Question
A 20-year-old man presents to the ED with fever and severe right lower quadrant (RLQ) pain for 1 day. Prior to this episode, he reports 2 months of crampy abdominal pain, generalized malaise, a 5kg weight loss, and occasional bloody diarrhoea. On physical exam, the patient appears uncomfortable and has a tender mass is in the RLQ. An abdominal CT scan demonstrates normal appendix and inflammation of the distal ileum and several areas of the colon without rectal involvement.
Which of the following is the most likely diagnosis?
Answer
-
Crohn's Disease
-
Ulcerative Colitis
-
Appendicitis
-
Diverticulitis
-
Pseudomembranous colitis
Question 6
Question
An older woman arrives at ED complaining of abdominal
pain. She states that the pain began as a vague aching but has migrated to
the left side of her abdomen. She had a fever over the past 3 days
and just not feeling like herself. She also complains of being more constipated
than usual. Your abdominal exam reveals normal bowel sounds, mild distension, and tenderness over the left lower quadrant. What is most likely the reason for this
Answer
-
Colorectal cancer
-
Diverticulitis
-
Appendicitis
-
Crohn’s disease
-
Duodenal ulcer
Question 7
Question
What is the blood supply to the superior rectum?
Answer
-
celiac artery
-
superior mesenteric artery
-
inferior mesenteric artery
-
internal iliac artery
-
external iliac artery
Question 8
Question
A elderly man attends your clinic with a three-month history of weight loss of
approximately 9 kg despite a normal appetite. A full blood count reveals that his
hemoglobin is 9.0 g/dL (previous hemoglobin was 13.5 g/dL one year ago) and
the MCV is 71 fL.
The abdominal examination is unremarkable and per rectum exam is
unremarkable. The patient states that he has normal bowel habits and has been feeling
quite tired lately.
What is the most appropriate management?
Answer
-
Reassure and discharge
-
Prescribe iron tablet supplementation
-
have an abdominal ultrasound
-
have an abdominal x-ray
-
have an upper and lower GI endoscopy
Question 9
Question
A middle aged woman has a four-month history of diarrhoea
and bloating. Associated symptoms include lethargy and weight loss.
Full blood count reveals:
hemoglobin of 9.3 d/gL (13.8 to 17.2)
MCV 70 fL. (77-95)
What other investigation allow proper patient diagnosis?
Answer
-
Anti-mitochondrial antibodies
-
Anti-smooth muscle antibodies
-
Anti-nuclear antibodies
-
Anti-tissue transglutaminase antibodies
-
Anti-neutrophil cytoplasmic antibodies
Question 10
Question
You see an elderly man with an acute episode of hematemesis, who was admitted the night before and is awaiting an upper GI endoscopy. You are asked on the ward round about the common causes of upper GI bleeding.
From the list below, which of the following is the most common cause of upper GI bleeding?
Answer
-
Mallory–Weiss tear
-
Peptic ulcers
-
Esophageal varices
-
Drug induced
-
Sporadic malignancy
Question 11
Question
You see a middle aged woman with Crohn’s disease. Due to a severe attack of Crohn’s which failed to respond to medical therapy, she had a small bowel resection. Your registrar tells you that she is at risk of developing vitamin B12 deficiency as a result of her surgery.
Which part of the bowel is responsible for the absorption of vitamin B12?
Answer
-
Ascending colon
-
Terminal ileum
-
Duodenum
-
Jejunum
-
Proximal Ileum
Question 12
Question
You see a middle aged man who was admitted for an elective upper GI endoscopy
due to longstanding GORD which has failed to improve on antacids and PPIs. Your
registrar suspects that this patient may have Barrett’s oesophagus and asks you to define what this is:
Answer
-
Metaplasia of the squamous epithelium of the lower third of the esophagus to columnar epithelium
-
Metaplasia of the columnar epithelium of the upper third of the oesophagus to squamous epithelium
-
Metaplasia of the squamous epithelium of the middle third of the oesophagus to columnar epithelium
-
Metaplasia of the squamous epithelium of the upper third of the oesophagus to columnar epithelium
-
Metaplasia of the columnar epithelium of the lower third of the oesophagus to squamous epithelium
Question 13
Question
Which of the following is the most common cause of duodenal ulcers?
Answer
-
NSAIDs
-
Alcohol Abuse
-
Helicobacter pylori
-
Chronic corticosteroid therapy
-
Zollinger-Ellison syndrome
Question 14
Question
A middle-aged lorry driver presents to the GP with chest pain that usually occurs after having a meal. He has no major past medical history and he takes ibuprofen regularly. He is otherwise fit and healthy.
What is the most important next step in management?
Answer
-
Urgent referral to endoscopy.
-
Routine referral to endoscopy.
-
Prescribe omeprazole, a PPI.
-
Perform a H. pylori urea test.
-
Perform a 12-lead ECG
Question 15
Question
You see a middle aged lorry driver, who presents to you with a three-month history of heartburn after meals which has not been settling with antacids and PPIs. You suspect that the patient has a hiatus hernia.
The most appropriate investigation for diagnosing a hiatus hernia is:
Answer
-
CT scan
-
Chest x-ray
-
Barium meal
-
Ultrasound
-
Upper GI endoscopy
Question 16
Question
A middle-aged woman is referred for upper gastrointestinal (GI) endoscopy following a four-month history of epigastric pain despite treatment with antacids and proton pump inhibitors (PPIs). The results demonstrate a duodenal ulcer coupled with a positive campylobacter-like organism (CLO) test. The patient has no past medical history and has no known drug allergies.
What is the most appropriate treatment?
Answer
-
Seven-day course of twice daily omeprazole 20 mg, 1 g amoxicillin and 500 mg clarithromycin
-
Seven-day course of twice daily omeprazole 20 mg
-
Seven-day course of twice daily omeprazole 20 mg and 1 g amoxicillin
-
Seven-day course of twice daily omeprazole 20 mg and 500 mg clarithromycin
-
Seven-day course of twice daily 1 g amoxicillin and 500 mg clarithromycin
Question 17
Question
You see a middle aged man with a three-month history of epigastric dull
abdominal pain. The pain is worse in the mornings and is better
after meals. There is no history of weight loss and the
patient’s bowel habits are normal. His abdomen is soft and
experiences moderate discomfort on palpation of the epigastric region. What is the most likely diagnosis?
Answer
-
Gastric ulcer
-
Gastro-oesophageal reflux disease (GORD)
-
Gastritis
-
Gastric carcinoma
-
Duodenal ulcer
Question 18
Question
You see an elderly man who comes to ED with epigastric pain. The pain started 3 days ago and today his stools color has changed to a ‘tarry-black’ color. Associated symptoms include nausea and lethargy.
The patient is alert and orientated with a pulse rate of 99 and blood pressure of 98/69, respiratory rate
of 18, oxygen saturations of 98 per cent on room air and temperature of 37.2°C.
The abdomen is soft with marked tenderness in the epigastric region and bowel sounds are present. The rectum is empty, on PR examination, with some traces of melaena. The patient has been started on high flow oxygen and has been given some oral analgesia.
The most appropriate next step in managing this patient is:
Answer
-
ECG
-
Intravenous omeprazole
-
Request an erect chest x-ray
-
Keep nil by mouth and arrange endoscopy
-
Intravenous cannulation and fluids
Question 19
Question
As you palpate the right upper quadrant (RUQ) of a middle aged woman’s abdomen, you notice that she stops her inspiration for a brief moment. The patient states that over the last 2 days she gets pain in her RUQ that radiates to her back shortly after eating.
Her vitals are temperature 38°C, heart rate (HR) 95, blood pressure (BP)
130/75, respiratory rate (RR) 16.
What is the initial diagnostic modality of choice for this disorder?
Answer
-
Plain film radiograph
-
CT scan
-
Ultrasound
-
MRI
-
ERCP
Question 20
Question
A middle-aged woman at ED complains of pain in her RUQ that is steady but gets worse with eating over the past 2 days. The
pain also radiates to the right side of her mid-back. No vomiting.
Her only medication is an oral contraceptive.
Her BP is 140/75 mm Hg, HR
is 80 beats per minute, temperature is 37°C, and RR is 16 breaths per
minute. Laboratory tests are within normal limits.
What is the most likely diagnosis?
Answer
-
Cholangitis
-
Pancreatitis
-
Cholecystitis
-
Peptic ulcer disease
-
Biliary colic
Question 21
Question
A 50-year-old man presents to the ED complaining of abrupt onset of epigastric pain that radiates to his back. He describes the pain as constant and associated with nausea and vomiting. The pain improves mildly if he leans forward. He has a 20-pack-year smoking history and consumes a 6-pack of beer daily for more than 5 years. His BP is 150/80 mm Hg, HR is 98 beats per minute, temperature is 37.8°C, and his RR is 18 breaths per
minute. He is tender to palpation in the epigastric area. His WBC count is normal and lipase 520 U/L (0-160 U/L).
What is the most likely diagnosis?
Answer
-
Cholecystitis
-
Bowel perforation
-
Mesenteric ischemia
-
Abdominal aortic aneurysm
-
Pancreatitis
Question 22
Question
A 55-year-old man presents to the ED complaining of mild diffuse abdominal pain. The pain began upon waking up and is associated with some nausea. He denies fever, vomiting, diarrhoea, and rectal bleeding. His BP is 143/71 mm Hg, HR is 87 beats per minute, temperature is 36°C, and RR is 16 breaths per minute. His abdomen is tense but only mildly tender. You order baseline labs. His chest radiograph is seen below. Which of the following is the most likely diagnosis?
Answer
-
Ascending cholangitis
-
Acute pulmonary edema
-
Ruptured aneurysm
-
Pancreatitis
-
Perforation with pneumoperitoneum
{kind=link}
Question 23
Question
A 33-year-old man presents to the ED complaining of lower abdominal pain. He states that last night he ate pizza with pepperoni for dinner, went to sleep, and awoke several hours later with a vague, periumbilical pain. The pain has been constant since its onset and has migrated to his lower abdomen more on the right than left. Since eating the pizza he has no appetite. He is nauseated and vomited twice in the ED. His BP is 125/70 mm Hg, HR is
88 beats per minute, temperature is 38°C, and his RR is 16 breaths per
minute. On exam, his RLQ is tender to palpation.
What is the most likely diagnosis?
Answer
-
Cholangitis
-
Appendicitis
-
Diverticulitis
-
Pancreatitis
-
Acute cholecystitis
Question 24
Question
Patient presents with painless jaundice and palpable RUQ mass. Which of the following is the most likely diagnosis
Answer
-
Cholecystitis
-
Cholangitis
-
Abdominal aortic aneurysm
-
Crohn’s disease
-
Gall bladder carcinoma
Question 25
Question
A 71-year-old obese man is brought to the ED complaining of constant left middle quadrant abdominal pain with radiation into his back. His past medical history is significant for hypertension, peripheral vascular disease, and kidney stones. He smokes a pack of cigarettes daily. His BP is 145/80 mm Hg, HR is 90 beats per minute, temperature is 37.2°C, and RR is 16 breaths per minute. Abdominal exam shows a pulsatile abdominal mass. An abdominal radiograph reveals normal loops of bowel.
Which of the following is the most likely diagnosis?
Answer
-
Biliary colic
-
Diverticulitis
-
Pancreatitis
-
Small bowel obstruction
-
Abdominal aortic aneurysm
Question 26
Question
A 78-year-old woman is brought to the ED by EMS complaining of vomiting and abdominal pain that began during the night. EMS reports that her BP is 90/50 mm Hg, HR is 110 beats per minute, temperature is 38°C, and RR is 18 breaths per minute. After giving her a 500 mL bolus of normal saline, her BP is 115/70 mm Hg. During the exam, you notice that her face and chest appear jaundiced.
What is the most likely diagnosis?
Answer
-
Cholecystitis
-
Acute hepatitis
-
Cholangitis
-
Pancreatic cancer
-
Bowel obstruction
Question 27
Question
What is NOT true regarding GI anatomy?
Answer
-
The foregut is from the distal (abdominal) esophagus to hepatopancreatic ampulla of the duodenum (2nd part of the duodenum.)
-
The mesentery includes the liver, gallbladder, pancreas, and spleen
-
Midgut ends at 2/3rds along the transverse colon.
-
The Hindgut ends at the anus.
Question 28
Question
The GI wall, from the [blank_start]lower[blank_end] [blank_start]espohagus[blank_end] to the [blank_start]anus[blank_end], has the same 4 layers (from outermost to innermost)
1. [blank_start]Serosa[blank_end]
2. [blank_start]Muscularis[blank_end]
3. [blank_start]Submucosa[blank_end]
4. [blank_start]Mucosa[blank_end]
Answer
-
lower
-
espohagus
-
anus
-
Serosa
-
Muscularis
-
Submucosa
-
Mucosa
Question 29
Question
The foregut is supplied by the [blank_start]celiac[blank_end] [blank_start]trunk[blank_end], which comes off the aorta at level [blank_start]T12[blank_end].
The midgut is supplied by the [blank_start]superior[blank_end] [blank_start]mesenteric[blank_end] artery, which comes off the aorta at level [blank_start]L1[blank_end].
The hindgut is supplied by the [blank_start]inferior[blank_end] [blank_start]mesenteric[blank_end] artery, which comes off the aorta at level [blank_start]L3[blank_end].
Answer
-
celiac
-
trunk
-
T12
-
superior
-
mesenteric
-
L1
-
inferior
-
mesenteric
-
L3
Question 30
Question
The GI tract lymphatics and vasculature is about the same.
Answer
- True
- False
Question 31
Question
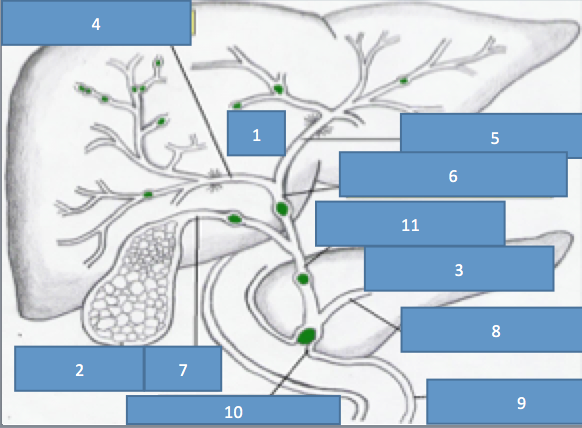
Which is NOT a major lymph structures involved with abdominal drainage?
Answer
-
Celiac nodes
-
Superior Mesenteric Aortic/Caval nodes
-
Inferior Mesenteric Aortic/Caval nodes
-
Renal nodes
Question 32
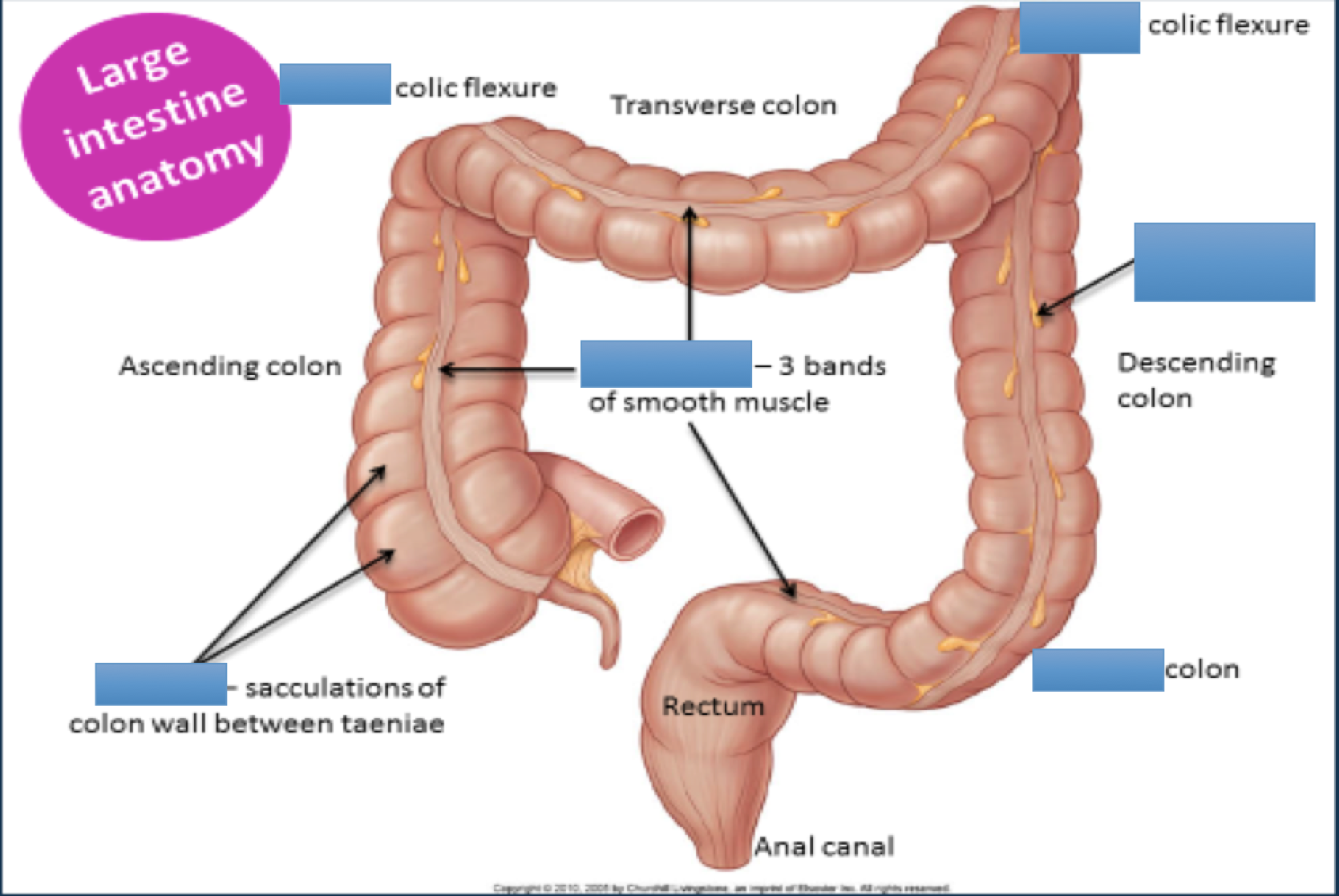{kind=link}
Answer
-
right
-
left
-
hastura
-
tenie coli
-
sigmoid
-
omental appendices
Question 33
Question
Large Intestine Blood Supply:
[blank_start]Superior[blank_end] rectal artery is a branch of the [blank_start]inferior[blank_end] [blank_start]mesenteric[blank_end] artery.
However, the [blank_start]middle[blank_end] rectal and [blank_start]inferior[blank_end] rectal arterys are both branches of [blank_start]internal[blank_end] [blank_start]iliac[blank_end] artery.
Answer
-
inferior
-
mesenteric
-
internal
-
iliac
-
Superior
-
middle
-
inferior
Question 34
Question
What is true regarding the esophagus' histology?
Answer
-
made of nonkeratinized squamous epithelium
-
upper skeletal sphincter
-
lower smooth sphincter
-
upper 1/3 skeletal muscle
-
middle 1/3 skeletal and smooth muscle
-
lower 1/3 smooth muscle
-
cyclic mucus secretions
-
upper 1/3rd squamous cells
Question 35
Question
Pharyngeal Pouch ([blank_start]Zenker[blank_end] diverticulum) is an out-pouching (diverticulum) that develops from the [blank_start]posterior[blank_end] wall of the [blank_start]pharynx[blank_end] just prior to the [blank_start]esophagus[blank_end].
Answer
-
posterior
-
pharynx
-
esophagus
-
Zenker
Question 36
Question
What is true regarding Zenker diverticulum?
Answer
-
management: surgery
-
investigation: barium swallow
-
management: corticosteroids
-
dysphagia
-
halitosis
-
stomach gurgling upon palpatation
-
constipation
-
diarrea
Question 37
Question
What is true regarding achalasia?
Answer
-
affects esophageal motility
-
lower esophageal sphincter unable to relax
-
gradual dysphagia to solids and liquids
-
weight loss
-
form of acid reflux--> damages esophageal cells
-
vomiting
-
prolonged dysphagia
-
drugs trtment: nitrates
-
drugs trtment: caclium channel blockers
-
investiagtion: manometry and endoscopy
Question 38
Question
[blank_start]Gastroesophageal[blank_end] [blank_start]Reflux[blank_end] [blank_start]Disease[blank_end] (GERD/GORD) is a condition in which the stomach contents are regurgitated back the esophagus, usually because the [blank_start]lower[blank_end] [blank_start]esophageal[blank_end] sphincter is unable to fully close after swallowing.
Answer
-
Gastroesophageal
-
Reflux
-
Disease
-
esophageal
-
lower
Question 39
Question
What is true regarding GORD?
Answer
-
dyspepsia is main symptom
-
preferable investigation via endoscopy
-
manage via lifestyle changes
-
manage via proton pump inhibitors
-
manage via gastrin inhibitors
-
risk factors = smoking, alcohol, and obesity
-
risk factor = chocolate
-
risk factor= pregnancy
-
preferable investigation via blood tests
-
preferable investigation via sputum culture
Question 40
Question
A Mallory-Weiss Tear is when there is bleeding from a laceration in the [blank_start]mucosa[blank_end] at the junction of the [blank_start]stomach[blank_end] and [blank_start]esophagus[blank_end]. This is usually caused by severe [blank_start]vomiting[blank_end], such as from [blank_start]alcoholism[blank_end], bulimia, or food [blank_start]poisoning[blank_end].
The signaling symptom is painful hematemesis. It is diagnosed by endoscopy.
Answer
-
mucosa
-
stomach
-
esophagus
-
vomiting
-
alcoholism
-
poisoning
Question 41
Question
Label the diagram showing the GI venous drainage. (the colors are just to differentiate between the various vessels)
{kind=link}
Answer
-
inferior mesenteric vein
-
superior mesenteric vein
-
hepatic portal vein
-
splenic vein
-
splenic vein
Question 42
Question
The liver is supplied by the hepatic portal vein (which is made up of the [blank_start]splenic[blank_end] vein and the [blank_start]superior[blank_end] [blank_start]mesenteric[blank_end] vein) and the hepatic artery.
[blank_start]75[blank_end]% of blood going to the liver is from the hepatic portal vein while [blank_start]25[blank_end]% is from the hepatic artery.
However, [blank_start]oxygenated[blank_end] blood is split ~50:50 between the portal vein and hepatic arteries.
Answer
-
splenic
-
mesenteric
-
superior
-
75
-
25
-
oxygenated
Question 43
Question
Which of these does NOT directly come off of the celiac trunk?
Answer
-
splenic artery
-
common hepatic artery
-
left gastric artery
-
proper hepatic artery
Question 44
Question
The common hepatic artery becomes the proper hepatic artery after the gastroduodenal artery branch.
Answer
- True
- False
Question 45
Question
Label the parts of the GI arterial vasculature. (max amnt words for any answr is 3)
{kind=link}
Answer
-
abdominal aorta
-
celiac artery
-
splenic artery
-
left gastric artery
-
Superior Posterior Pancreatoduodenal
-
Superior Anterior Pancreatoduodenal
-
Superior pancreatoduodenal artery
-
Right gastroepiploic artery
-
common hepatic artery
-
Hepatic artery proper
-
Right gastric artery
-
Gastroduodenal artery
Question 46
Question
Which comes first in the development of a carcinoma?
Answer
-
metaplasia
-
dysplasia
Question 47
Question
[blank_start]Metaplasia[blank_end] is the reversible change of one cell type to another
[blank_start]Dysplasia[blank_end] is abnormal changes in the cell and disorganized [blank_start]growth[blank_end]
Carcinoma is the eventual transformation into malignant [blank_start]neoplastic[blank_end] cells.
Answer
-
Metaplasia
-
growth
-
Dysplasia
-
neoplastic
Question 48
Question
[blank_start]Barrett’s[blank_end] [blank_start]Esophagus[blank_end] is a pre-malignant condition of the lower esophagus. This happens when the [blank_start]squamous[blank_end] cells go through metaplasia and become [blank_start]columnar[blank_end] cells. This change usually happens as defence against an [blank_start]acidic[blank_end] environment, which may be due to conditions like [blank_start]GERD[blank_end]. This condition puts the patient of increased risk of esophageal [blank_start]adenocarcinoma[blank_end].
Answer
-
Barrett’s
-
Esophagus
-
squamous
-
columnar
-
acidic
-
GERD, GORD
-
adenocarcinoma
Question 49
Question
The management of Barret's Esophagus is to do a [blank_start]biopsy[blank_end].
Premalignant changes are indicative of high-grade [blank_start]dysplasia[blank_end]. The treatment for this in younger and more fit individuals is an [blank_start]esophageal[blank_end] [blank_start]resection[blank_end]. For others, it's [blank_start]mucosal[blank_end] [blank_start]ablation[blank_end].
If there are no premalignant channges, the patient will have regular [blank_start]endoscopy[blank_end], biopsy, and other anti-reflux measures, including long term [blank_start]proton[blank_end] [blank_start]pump[blank_end] [blank_start]inhibitors[blank_end] (drugs).
Answer
-
endoscopy
-
proton
-
pump
-
inhibitors
-
dysplasia
-
esophageal
-
resection
-
ablation
-
mucosal
-
biopsy
Question 50
Question
What is true regarding esophageal carcinoma?
Answer
-
symptom: vomiting
-
symptom: weight loss
-
symptom: anorexia
-
presentation: progressive dysphagia
-
investigation: chest xray
-
investigation: urgent endoscopy + biopsy
-
investigation: CT or MRI chest and upper abdomen
-
symptom: hoarse voice
-
symptom: excessive acid reflux
-
investigation: neck ultrasound
Question 51
Question
The stomach has 2 muscle layers: inner oblique and outer longitudinal
Answer
- True
- False
Question 52
Question
The stomach is lined by simple squamous epithelial cells
Answer
- True
- False
Question 53
Question
What controls the secretion of gastric acid?
Answer
-
the parasympathetic nervous system
-
gastrin
-
histamine
-
PGE2
-
PGI2
-
pepsinogen concentration
-
gut bacteria
Question 54
Question
Prostaglandins increase acid secretion
Answer
- True
- False
Question 55
Question
A side effect of NSAIDs is peptic ulcers.
Answer
- True
- False
Question 56
Question
Which of these are considered GI drugs?
Answer
-
proton pump inhibitors
-
histamine receptors
-
synthetic prostaglandins
-
antacids
-
amoxicillin
-
metronidazole
-
clarithromycin
-
calcium channel blockers
-
beta blockers
-
pepto bismol
Question 57
Question
Fill in which drugs go into which parts of the cycle to help with acid control:
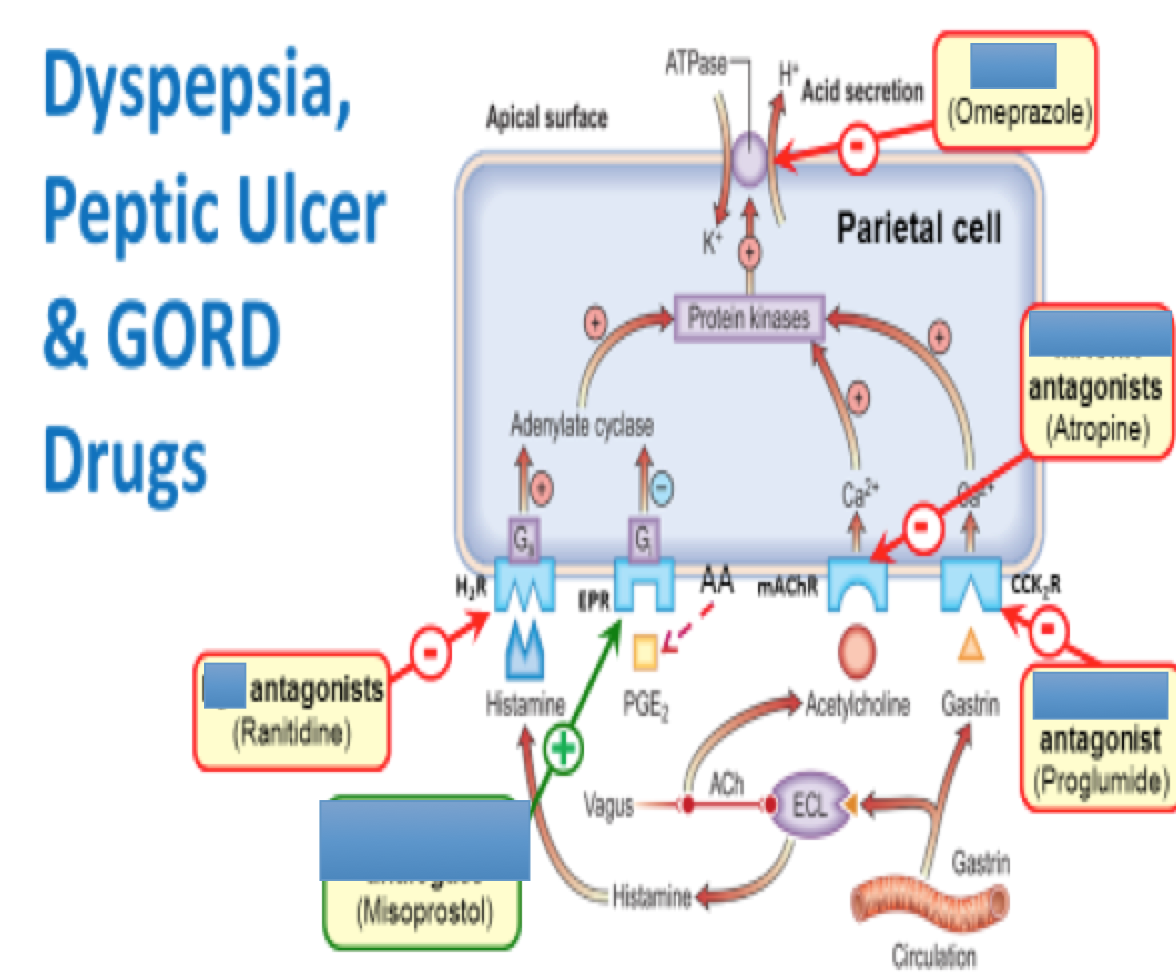{kind=link}
Answer
-
histamine
-
prostaglandin analogues
-
muscarinic acetylcholine
-
proton pump inhibitors
-
gastrin receptor
Question 58
Question
What is not a sign of dyspepsia?
Answer
-
epigastric pain
-
bloating
-
heartburn
-
burning sensation during defecation
Question 59
Question
Worrying symptoms of dyspepsia:
A [blank_start]anemia[blank_end]
L loss of weight
A [blank_start]anorexia[blank_end]
R recent [blank_start]progressive[blank_end] [blank_start]symptoms[blank_end]
M [blank_start]melena[blank_end] (tarry feces) and [blank_start]hematemesis[blank_end]
S wallowing difficulty
Answer
-
anemia
-
anorexia
-
progressive
-
symptoms
-
melena
-
hematemesis
Question 60
Question
What are ways to manage dyspepsia?
Answer
-
simple antacids for 4 weeks
-
test for H. Pylori and eliminate if possible
-
Proton pump inhibitors for 4 weeks
-
urgent endoscopy
-
biopsy
-
blood works
Question 61
Question
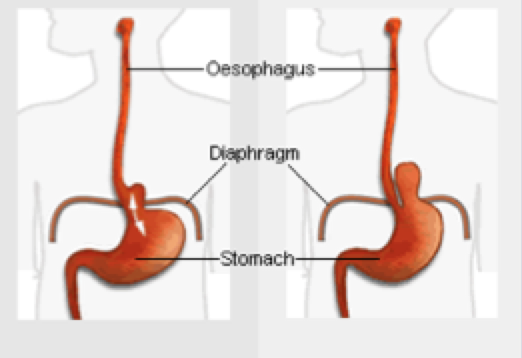
Label the different types of hiatus hernias
{kind=link}
Answer
-
sliding
-
rolling
Question 62
Question
Barium swallow via fluoroscopy is how one is able to diagnose a hiatus hernia.
Answer
- True
- False
Question 63
Question
What is true regarding peptic ulcers?
Answer
-
include duodenal ulcers
-
include gastric ulcers
-
complication: hemorrhage
-
complication: ulcer perforation
-
complication: malignancy (tumor)
-
include jejunal ulcers
-
gastric ulcers > common than duodenal ulcers
Question 64
Question
What is true regarding duodenal ulcers?
Answer
-
epigastric tenderness
-
epigastric pain before meals
-
relief via milk
-
epigastric pain better at night
-
relief via lemon soda
Question 65
Question
Gastric ulcers:
- happens mainly in [blank_start]elderly[blank_end]
- [blank_start]epigastric[blank_end] pain (dependent on [blank_start]meals[blank_end] and can be relieved by antacids)
- weight gain or loss
Answer
-
elderly
-
epigastric
-
meals
Question 66
Question
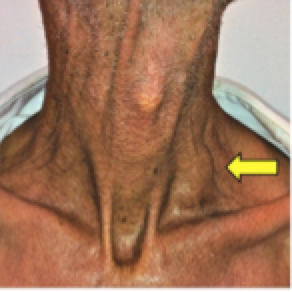
What is this sign and what is indicative of?
{kind=link}
Answer
-
Virchow's node
-
gastric cancer
Question 67
Question
What is true regarding zollinger-ellison syndrome?
Answer
-
gastrinoma--> peptic ulcer
-
usually in duodenum
-
usually in pancreas
-
investigation: endoscopy
-
investigation: very high fasting and then serum gastrin level investigation
-
investigation: biopsy
-
management: surgery
-
management: proton pump inhibitors
-
management: antacids
-
usually in ileum
Question 68
Question
iron is absorbed in the jejunum.
Answer
- True
- False
Question 69
Question
[blank_start]Celiac[blank_end] [blank_start]disease[blank_end] is an inflammation of the proximal small intestine mucosa in response to dietary gluten.
It is Hypersensitivity [blank_start]IV[blank_end]. It is a disease of the small intestines in which [blank_start]prolamin[blank_end] [blank_start]intolerance[blank_end] causes villous atrophy and [blank_start]malabsorption[blank_end].
Answer
-
Celiac
-
disease
-
IV
-
prolamin
-
intolerance
-
malabsorption
Question 70
Question
What are symptoms of Celiac's Disease?
Answer
-
diarrhea
-
malaise
-
abdominal discomfort
-
iron deficiency anemia
-
weight loss
-
steatorrhea
-
weariness
-
concentrated pain
-
bursts of energy
Question 71
Question
Celiac disease makes you at more risk of colon cancer and lymphoma.
Answer
- True
- False
Question 72
Question
Crohn's Disease treatment is a gluten free diet and necessary vitamin supplements.
Answer
- True
- False
Question 73
Question
Which of the following is not a way to diagnose Celiac's disease?
Answer
-
duodenal biopsy via endoscopy
-
blood test: abnormally high levels of IgA endomysial
-
blood test: if anti-tissue transglutaminase antibodies are found
-
abdominal x-ray
Question 74
Question
What is true regarding diverticulitis?
Answer
-
only in relation to the large intestine
-
inflammation of colon's diverticulae
-
more common in elderly patients
-
more common in those chronically constipated
-
more common in women
-
more common in those with acute constipation
-
commonly associated with anal fissures
Question 75
Question
Which are symptoms of diverticulitis?
Answer
-
lower left quadrant pain
-
lower left quadrant tenderness
-
fever
-
tenesmsus
-
diarrhea
-
constipation
Question 76
Question
How can you investigate for diverticulitis?
Answer
-
barium enema
-
colonoscopy
-
CT colonogram
-
rectal biopsy
Question 77
Question
Treatment of diverticulitis:
mild:
at home with [blank_start]paracetamol[blank_end], fluids, and [blank_start]oral[blank_end] [blank_start]antibiotics[blank_end].
severe or ill patients:
admission to hospital (cannot manage [blank_start]pain[blank_end], problems with [blank_start]dehydration[blank_end], [blank_start]frail[blank_end])
Answer
-
paracetamol
-
antibiotics
-
oral
-
pain
-
dehydration
-
frail
Question 78
Question
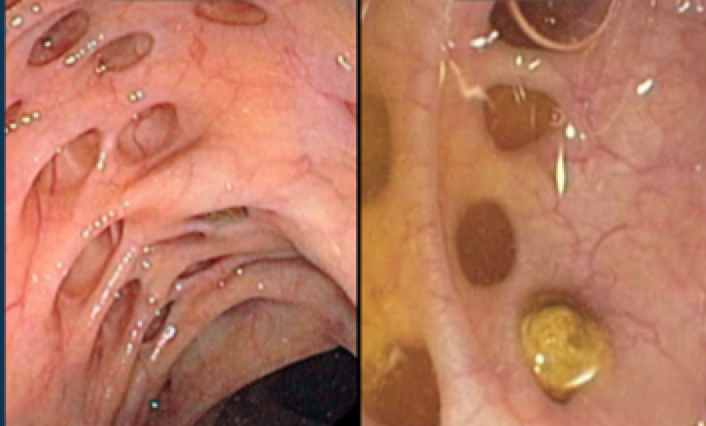
What are these two colon related conditions?
{kind=link}
Answer
-
diverticulitis
-
diverticulosis
Question 79
Question
Which conditions make up inflammatory bowel disease?
Answer
-
Crohn's disease
-
Celiac's disease
-
Ulcerative Colitis
-
Diverticulitis
-
Peptic Ulcers
Question 80
Question
[blank_start]Crohn’s[blank_end] is a chronic inflammatory bowel disease affecting all layers of the GI tract ([blank_start]transmural[blank_end]). Its key characteristic is [blank_start]skip[blank_end] [blank_start]lesions[blank_end], and on a colonscopy there is a “[blank_start]cobblestone[blank_end] [blank_start]appearance[blank_end]." ANY part of the GI tract but most commonly the [blank_start]terminal[blank_end] [blank_start]ileum[blank_end] (can cause [blank_start]vitamin[blank_end] [blank_start]B12[blank_end] deficiency).
Answer
-
Crohn’s, Crohn's Disease
-
transmural
-
skip
-
lesions
-
cobblestone
-
appearance
-
terminal
-
ileum
-
B12
-
vitamin
Question 81
Question
What are symptoms of Crohn's Disease?
Answer
-
diarrhea
-
abdominal pain
-
right lower quadrant mass
-
perianal disease
-
mouth ulcers
-
extra-intestinal manifestations
-
pale and bulky stools
-
right lower quadrant pain
Question 82
Question
What is not an investigation for Crohn's Disease?
Answer
-
stool sample
-
colonscopy and biopsy
-
endoscopy and biopsy
-
Blood: CRP/ESR
-
Blood: FBC
-
Blood: LFTs
-
Blood: B12
-
Blood: ferritin
-
Barium swallow
Question 83
Question
Management of Crohn Disease attacks:
Mild attacks: [blank_start]Prednisolone[blank_end]
Severe attacks: IV [blank_start]steroids[blank_end], nil by mouth, and IV [blank_start]hydration[blank_end].
Answer
-
Prednisolone
-
steroids
-
hydration
Question 84
Question
Label the parts of the biliary tree?
{kind=link}
Answer
-
liver
-
right hepatic tree
-
left hepatic duct
-
common hepatic duct
-
common bile duct
-
pancreatic
-
pancreatic duct
-
duodenum
-
sphincter of Oddi
-
cystic duct
-
gallbladder
Question 85
Question
Bile is produced by [blank_start]hepatocytes[blank_end] and is stored in the [blank_start]gallbladder[blank_end]. Bile [blank_start]emulsifies[blank_end] the fat and allows fat absorption in [blank_start]enterocytes[blank_end]. An example of fat soluble vitamins: [blank_start]ADEK[blank_end]
Answer
-
hepatocytes
-
gallbladder
-
emulsifies
-
enterocytes
-
ADEK
Question 86
Question
An [blank_start]enterogastrone[blank_end] is any hormone secreted by the [blank_start]duodenum[blank_end] mucosa in response to dietary lipids that inhibits the caudal (or "forward, analward") motion of the contents of [blank_start]chyme[blank_end].
Answer
-
enterogastrone
-
duodenum
-
chyme
Question 87
Question
Relapsing inflammatory disorder of [blank_start]colonic[blank_end] mucosa which usually begins in the [blank_start]rectum[blank_end] and doesn’t spread past the [blank_start]ileocaecal[blank_end] valve is ulcerative colitis. This inflammation is not [blank_start]transmural[blank_end] and is [blank_start]continous[blank_end].
Answer
-
colonic
-
rectum
-
ileocaecal
-
transmural
-
continous
Question 88
Question
What is true regarding ulcerative colitis?
Answer
-
bloody diarrhea
-
abdominal pain
-
tenesmus
-
bathroom urgency
-
malaise
-
weight loss
-
extra-intestinal features
-
pale and bulky stool
-
dehydration
Question 89
Question
Which is not a way to investigate for ulcerative colitis?
Answer
-
FBC
-
liver function tests
-
urea and electrolytes profile
-
erythrocyte sedimentation rate
-
c reactive protein
-
ferritin
-
B12
-
folate
-
histamine
Question 90
Question
You can investigat for ulcerative colitis via sigmoidscopy or colonoscopy.
Answer
- True
- False
Question 91
Question
Management of Ulcerative Colitis:
[blank_start]Mesalazine[blank_end] (also known as 5-aminosalicylate) and steroids (such as [blank_start]prednisolone[blank_end]) to induce remission.
Surgery ([blank_start]colectomy[blank_end] for those non-responsive to drugs)
Mesalazine to maintain remission.
Answer
-
Mesalazine
-
colectomy
-
prednisolone
Question 92
Question
Pancreatic secretions are controlled by the [blank_start]parasympathetic[blank_end] nervous system.
[blank_start]Secretin[blank_end] in response to H+ in the duodenum causes the pancreas to secrete [blank_start]bicarbonate[blank_end].
In response to [blank_start]fats[blank_end] and [blank_start]amino[blank_end] [blank_start]acids[blank_end] in the duodenum, the pancreas releases CCK cholecystokinin (CCK). CCK also causes [blank_start]gallbladder[blank_end] contractions.
These proteolytic enzymes are released inactively as [blank_start]zymogens[blank_end] to protect the pancreatic tissue from being destroyed.
Answer
-
parasympathetic
-
Secretin
-
bicarbonate
-
gallbladder
-
fats
-
amino
-
acids
-
zymogens
Question 93
Question
Which of these are pancreatic enzymes?
Answer
-
trypsinogen
-
chymotripsinogen
-
procarboxypeptidase
-
pancreatic amylase
-
pancreatic lipase
-
gastrin
-
pepsinogen
Question 94
Question
pancreatic enzymes:
trypsin, chymotrypsin, carboxypeptidase: act on [blank_start]proteins[blank_end]
pancreatic lipase acts on [blank_start]fat[blank_end]
pancreatic amylase acts on [blank_start]carbohydrates[blank_end]
ribonucleoase/deoyribonuclease acts on nucleic acids
Answer
-
proteins
-
fat
-
carbohydrates
Question 95
Question
What are examples of tumor markers?
Answer
-
CEA
-
alpha fetoprotein (aFP)
-
CA 1999
-
beta HCG
-
Ca 125
-
BRCA 2
-
Ca 187
Question 96
Question
Tumor suppressor genes cause tumors to actually progress.
Answer
- True
- False
Question 97
Question
p53 is a tumor suppressor gene that is important because it can trigger apoptosis.
Answer
- True
- False
Question 98
Question
What is the condition that describes a type of pain related to the gallbladder that occurs when a gallstone temporarily obstructs the cystic duct and the gallbladder contracts?
Answer
-
Biliary Colic
-
Cholangitis
-
Cholecystitis
-
Courvoisier's syndrome
Question 99
Question
What is true regarding biliary colic?
Answer
-
goldstone investigation: ultrasound of right upper quadrant
-
manage: analgesia
-
manage: rehydrate
-
medication given via orally
-
manage: elective cholecystectomy
-
nausea and vomiting
-
indigestion symptoms
-
pain after a fatty meal
-
right upper quadrant pain which radiates
-
acid reflux
Question 100
Question
[blank_start]Acute[blank_end] cholecystitis:
Due to stone impaction in the gallbladder neck
Symptoms:
Continuous [blank_start]RUQ[blank_end] pain or [blank_start]Epigastric[blank_end] pain which radiates to the right shoulder
[blank_start]vomiting[blank_end]
fever
Investigation: [blank_start]Ultrasound[blank_end]
Treatment: Nil by mouth: analgesia; antibiotics; and [blank_start]cholecystectomy[blank_end]
Answer
-
Acute
-
RUQ
-
Epigastric
-
vomiting
-
Ultrasound
-
cholecystectomy
Question 101
Question
[blank_start]Chronic[blank_end] cholecystitis:
Stones cause chronic inflammation of gallbladder +/- [blank_start]colic[blank_end] inflammation
Symptoms:
Abdomen discomfort
[blank_start]distension[blank_end]
nausea
[blank_start]flatulence[blank_end]
fat intolerance
Investigation: [blank_start]Ultrasound[blank_end]
Treatment: [blank_start]cholecystectomy[blank_end]
Answer
-
Chronic
-
colic
-
distension
-
Ultrasound
-
cholecystectomy
-
flatulence
Question 102
Question
Courvoisier's law is that the possible malignancy of the [blank_start]gallbladder[blank_end]/[blank_start]pancreas[blank_end], such as swelling, is not probably due to [blank_start]gallstones[blank_end].
Answer
-
gallbladder
-
pancreas
-
gallstones
Question 103
Question
What is not true regarding cholangitis?
Answer
-
inflammation of the common bile duct due to gall stones obstruction
-
investigation: ERCP
-
Charcot's triad
-
investigation: ultrasound
Question 104
Question
Pancreatitis is due to injuries that lead to autodigestion of the pancreas by its own [blank_start]enzymes[blank_end].
[blank_start]Acute[blank_end] pancreatitis is characterized by reversible pancreatic [blank_start]parenchymal[blank_end] injury associated with inflammation. [blank_start]Biliary[blank_end] [blank_start]tract[blank_end] disease and alcoholism account for approximately 80% of cases of [blank_start]acute[blank_end] pancreatitis in Western countries.
[blank_start]Chronic[blank_end] pancreatitis is defined as prolonged inflammation of the pancreas associated with irreversible destruction of [blank_start]exocrine[blank_end] parenchyma, [blank_start]fibrosis[blank_end], and, in the late stages, the destruction of [blank_start]endocrine[blank_end] parenchyma. The most common cause of [blank_start]chronic[blank_end] pancreatitis by far is long-term [blank_start]alcohol[blank_end] abuse
Answer
-
enzymes
-
Acute
-
Chronic
-
parenchymal
-
tract
-
Biliary
-
acute
-
chronic
-
alcohol
-
exocrine
-
endocrine
-
fibrosis
Question 105
Question
What is NOT true regarding pseudocyst?
Answer
-
most common complication of pancreatitis
-
is the accumulation n of fluid within and around the pancreatic tissue.
-
trtment: drainage of fluid into stomach's lumen
-
investigation: type II MRI
Question 106
Question
Which of these can cause chronic pancreatitis?
Answer
-
alcohol
-
cystic fibrosis
-
hemochromastosis
-
pancreatic duct obstruction
-
renal failure
-
liver disease
-
obesity
Question 107
Question
Ultrasound and CT to check for pancreatic calcifications is how to investigate for chronic pancreatitis.
Answer
- True
- False
Question 108
Question
What are symptoms of chronic pancreatitis?
Answer
-
epigastric pain radiating to the back
-
epigastric pain is less when sitting forward
-
epigastric pain is less with hot water bottles
-
bloating
-
weight loss
-
brittle diabetes
-
steatorrhea
-
manage: lipase and fat soluble vitamins
-
manage: low fat diet
-
manage: surgery
Question 109
Question
CAUSES for acute pancreatitis:
GET SMASHED:
[blank_start]Gallstones[blank_end] (38%)
[blank_start]Ethanol[blank_end] (35%)
[blank_start]Trauma[blank_end] (1.5%)
[blank_start]Steroids[blank_end]
[blank_start]Mumps[blank_end]
[blank_start]Autoimmune[blank_end]
Scorpion venom
Hyperlipidaemia/[blank_start]hypothermia[blank_end]/ hypercalcaemia
[blank_start]ERCP[blank_end] and emboli
Drugs.
Answer
-
Gallstones
-
Ethanol
-
Trauma
-
Steroids
-
Autoimmune
-
Mumps
-
hypothermia
-
ERCP
Question 110
Question
What are the signs and symptoms of acute pancfdatitis?
Answer
-
tachycardia
-
fever
-
jaundice
-
Cullen's sign
-
Gray Turner's sign
-
gradual epigastric pain
-
severe epigastric man
-
vomiting
-
central abdominal pain which radiates to the back
-
investigation: dropped serum levels of amylase
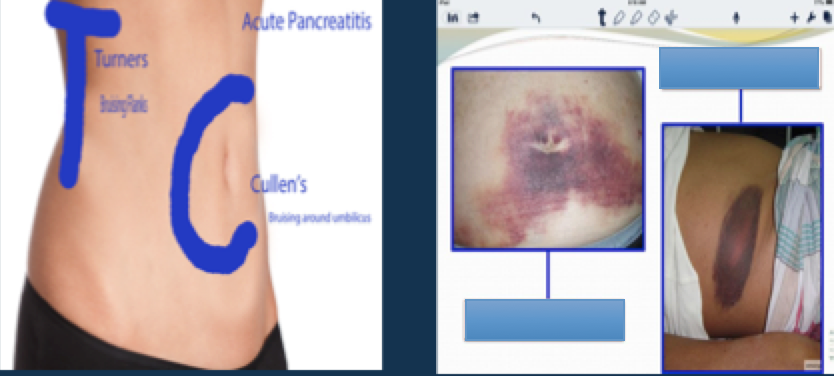
Question 111
{kind=link}
Answer
-
cullen's sign
-
turner's sign
Question 112
Question
Serum lipase is the most reliable investigating factor for pancreatitis.
Answer
- True
- False
Question 113
Question
Management of acute pancreatitis:
Nil by mouth: [blank_start]analgesia[blank_end]
[blank_start]ERCP[blank_end] + [blank_start]gallstone[blank_end] [blank_start]removal[blank_end] may be needed if progressive jaundice.
Answer
-
analgesia
-
ERCP
-
gallstone
-
removal
Question 114
Question
Those at an increased risk of developing cancer often are born with one defective copy of a [blank_start]tumor[blank_end] [blank_start]suppressor[blank_end] gene.
Answer
-
tumor
-
suppressor
Question 115
Question
An oncogene is when a proto-oncogene becomes mutated.
Answer
- True
- False
Question 116
Question
Oncogenes cause uncontrolled tumor growth.
Answer
- True
- False
Question 117
Question
Appendicitis:
presentation:
[blank_start]Fever[blank_end]
RLQ pain or [blank_start]umbulical[blank_end] pain
nausea
vomiting
KEY: loss of appetite
investigation: [blank_start]Xray[blank_end]
Answer
-
Xray, x-ray
-
umbulical
-
Fever
Question 118
Question
How does ischemic bowel NOT present?
Answer
-
severe abdominal pain
-
tachycardia + hypotension
-
raised leukocyte count
-
fever intervals
Question 119
Question
Murphy's sign is for acute cholecystitis.
Murphy's sign is that on palpation of the RUQ, patient stops inspiration for a moment.
Answer
- True
- False
Want to create your own Quizzes for free with GoConqr? Learn more.