4086951
Description
Quiz by Mohammed Al-Dhahir, updated more than 1 year ago
|
|
Created by Mohammed Al-Dhahir
about 9 years ago
|
|
Question 1
Question
A patient presents with a classic type II odontoid fracture. A magnetic resonance image and flexion-extension dynamic radiographs of the cervical spine are consistent with disruption of the transverse ligament. The MOST appropriate
treatment is:
Answer
-
Hard cervical collar
-
Halo immobilization
-
Anterior odontoid screw fixation
-
Posterior C1-C2 fixation
-
Occipital-cervical fusion
Question 2
Question
A 43 year old male with metastatic lung cancer presents with subacute thoracic myelopathy. Imaging studies demonstrate a metastatic lesion at T7 with ventral spinal cord compression and 30 degrees of focal kyphosis. The treatment associated with the BEST outcome is:
Answer
-
High dose steroids
-
Conventional radiation therapy
-
Decompressive laminectomy
-
Transthoracic vertebrectomy
-
Stereotactic radiosurgery
Question 3
Question
Static plain radiographs after a posterolateral lumbar fusion are MOST useful to assess which clinical feature:
Answer
-
Functional outcome
-
Fusion status
-
Pain relief
-
Resting alignment
Question 4
Question
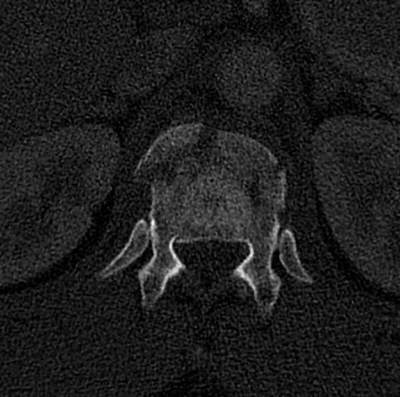
A 36 y/o restrained driver presented after an MVC. He complained of weakness and a numb feeling in his legs. Examination showed 4-/5 strength in his proximal and 3/5 strength in his distal lower extremities and an L1 sensory level. Lumbar spine radiographs and axial CT through the level of injury are shown below. What is the spinal injury type:
{kind=link}
Answer
-
Compression fracture
-
Burst fracture
-
Teardrop fracture
-
Fracture dislocation
-
Chance fracture
Question 5
Question
A 47 year old dentist presents with a 5 year history of intractable low back pain refractory to several courses of physical therapy and numerous medications. He has recently developed bilateral L5 radiculopathy. MR imaging demonstrates grade II anterolisthesis of L4 on L5 with resulting L4-5 central canal stenosis and bilateral neuroforaminal stenosis. The BEST treatment option is:
Answer
-
Laminectomy with facetectomy
-
Anterior lumbar interbody cage fusion
-
Laminectomy and pedicle screw fusion
-
Epidural steroid injection
-
Dorsal column stimulator
Question 6
Question
What are the current evidence-based guidelines regarding posterolateral lumbar fusion for patients with radiculopathy due to intervertebral disc herniation?
Answer
-
A. Recommended for patients who fail to improve with six to eight weeks of conservative management.
-
Not recommended because simple decompression is associated with better outcomes
-
Recommended in patients with recurrent disc herniations without evidence of instability, deformity, or chronic low back pain
-
Not recommended because interbody fusions are associated with better outcomes
-
Recommended for patients with large para-central disc herniations
Question 7
Question
Lumbar orthosis use is MOST effective to:
Answer
-
Predict the success of subsequent lumbar fusion for patients with chronic low back pain
-
Improve functional outcome following lumbar fusion in patients with chronic low back pain
-
Improve fusion rate following lumbar fusion in patients with chronic low back pain
-
Reduce the symptoms reported by patients with chronic low back pain due to back injury
-
Reduce the numbers of sick days used by workers with a history of back injury
Question 8
Question
A normal intraoperative electromyographic study during lumbar fusion surgery has been shown to BEST correlate with:
Answer
-
Pedicle fracture
-
Lack of a neurological injury
-
Improved patient outcomes
-
Improved fusion rates
Question 9
Question
The use of recombinant bone morphogenetic protein in the performance of a lumbar fusion is currently supported by randomized controlled clinical trials for which fusion approach/type:
Answer
-
Anterior lumbar interbody fusion procedures
-
Posterior lumbar interbody fusion procedures
-
Non-instrumented posterolateral lumbar fusion procedures
-
Instrumented posterolateral lumbar fusion procedures
Question 10
Question
A 51 year-old woman presents to the ED with a subcutaneous fluid collection in the lumbar area two days after undergoing a redo L4-5 laminectomy/discectomy at another institution. She is afebrile and has no neurological deficits but complains of headache when she sits up or stands. What is the MOST likely etiology of her fluid collection:
Answer
-
wound infection
-
wound seroma
-
wound hematoma
-
cerebrospinal fluid leak
-
subcutaneous foreign body
Question 11
Question
A 32 year-old I.V. drug user presents with severe low back pain. Lumbar MR imaging demonstrates L4-5 discitis and early osteomyelitis. Blood cultures grow staphylococcus. The MOST appropriate treatment is:
Answer
-
Oral cephalexin
-
Observation with imaging
-
Surgical debridement and fusion
-
Intravenous vancomycin
-
Oral or intravenous steroids
Question 12
Question
A 33 year-old woman with known metastatic breast carcinoma presents with a one day history of paraparesis and bladder incontinence. Her lower extremity motor strength is 2/5 in all groups. An MRI of her thoracic spine reveals dorsal cord compression at T9-T10 with preserved alignment. The MOST appropriate course of treatment is:
Answer
-
oral steroids
-
spinal radiation
-
no treatment
-
T9-10 laminectomy
-
T9-10 spondylectomy/instrumentation
Question 13
Question
A 45 year-old man fell from a horse 2 hours ago. He is neurologically intact but complains of neck pain. X-rays reveal a well aligned type 3 dens fracture. The MOST appropriate initial management of this patient is:
Answer
-
no treatment
-
external orthosis or halo
-
anterior odontoid screw fixation
-
posterior C1-2 fusion
-
occipito-cervical fusion
Question 14
Question
A 61 year old previously healthy man presents with progressive hand weakness, tingling in his fingers, and gait instability. Examination reveals atrophy and weakness of the hands, impaired rapid alternating movements, diminished pinprick sensation in the fingers, diffuse hyper-reflexia, and lower extremity spasticity. What is the MOST likely diagnosis:
Answer
-
Amytrophic Lateral Sclerosis
-
Subacute Combined System Disease
-
Normal Pressure Hydrocephalus
-
Cervical Spondylotic Myelopathy
-
Multiple Sclerosis
Question 15
Question
An isolated posterior approach is contraindicated in the presence of:
Answer
-
Subluxation at C3/4 and C4/5
-
Compressive pathology across multiple levels
-
Fixed kyphotic deformity
-
Posterior ligamentous hypertrophy
-
Ventral compressive pathology
Question 16
Question
A 48 year old women presents with progressive complaints of hand paresthesias, loss of fine motor control, gait instability, and urinary urgency (MR imaging is shown below). She undergoes a posterior decompression via an open-door laminoplasty from C3 to C7. On post-operative day number 3, she complains of bilateral shoulder pain and demonstrates mild weakness of her right deltoid. The MOST appropriate next step in the management of this patient is:
Answer
-
Emergent surgery for laminectomy/foraminotomy
-
Administration of corticosteroids
-
Bilateral selective nerve root injections
-
Bilateral upper extremity EMG
-
Orthopedic/Physiatry consult for "frozen shoulder."
Question 17
Question
A 35 year old man presents to your office with an insidious 6 month history of declining ability to walk, leg weakness, stumbling, and shooting pains down both legs. He denies an inciting event. He admits to axial, non-mechanical, thoracic pain that is most prominent at night, especially in the supine position. Physical exam reveals 4-/5 symmetric strength in his lower extremities and decreased sensation to both light touch and pin prick in the lower extremities and trunk up to the umbilicus. Proprioception is absent in the left lower extremity and present in the right. Reflexes are
3+ at the patella and Achilles tendon bilaterally with increased lower extremity tone. Babinski responses are extensor and rectal tone is present. The MOST appropriate initial management step is:
Answer
-
Prescribe non-steroidal anti-inflammatory medications
-
Obtain a contrasted MRI of the thoracic spine
-
Obtain plain radiographs and CT scan of the thoracic spine
-
Prescribe a course of physical therapy
-
Obtain a spinal angiogram from T2 through T12
Question 18
Question
A patient presents complaining of an 8 month history of axial cervical pain, worse when supine and at night, plus leg weakness requiring a walker. Physical exam reveals myelopathy. T1-weighted MRI demonstrates an enlargement of her cervical spinal cord by a hypointense mass in the dorsal cord, which intensely enhances on post-gadolinium images. T2-weighted MRI reveals peritumoral edema and syringomyelia. The neuroradiologist describes the tumor as most consistent with hemangioblastoma. The MOST appropriate first management step is:
Answer
-
External beam radiotherapy
-
MRI of the brain and lumbar puncture
-
Abdominal CT scan and 24 hour urinary catacholamines and metanephrines
-
Biopsy and post-operative radiotherapy
-
6 month follow-up MRI
Question 19
Question
A 43 year old man with a 3 month history of numbness and tingling in bilateral lower extremities, difficulty ambulating, and weakness in both hands and arms undergoes MR imaging of his cervical spine revealing a homogeneously enhancing intramedullary spinal cord tumor. The tumor diffusely and symmetrically enlarges the involved portion of the spinal cord without cyst formation. At surgery, intraoperative frozen section yields ependymoma. The MOST appropriate treatment strategy is:
Answer
-
Tumor debulking and duraplasty
-
Biopsy and external beam radiation
-
Attempted gross total resection
-
Subtotal resection and radiotherapy
Question 20
Question
A 54 year-old female presents 18 months after undergoing instrumented ACDF at C5-6 via a left-sided approach. She has neck pain and radiculopathy with pseudoarthrosis and instrumentation failure. She denies hoarseness or swallowing difficulties with the initial surgery. Being right-handed, you prefer a right-sided approach for her recommended revision surgery. What is the MOST appropriate management of the surgical approach in this case:
Answer
-
Right-sided approach without further work-up
-
Modified barium swallow prior to surgery
-
Laryngoscopic screening prior to surgery
-
Intra-operative EMG monitoring of the laryngeal muscles
Want to create your own Quizzes for free with GoConqr? Learn more.