6853266
Newborn Complications
Descripción
Diapositivas por Allie Winningham, actualizado hace más de 1 año
Más
Menos
|
|
Creado por Allie Winningham
hace alrededor de 8 años
|
|
Resumen del Recurso
Diapositiva 1
Newborn Complications
Amniocentesis
Fetal Lung Maturity (Transient Tachypnea of the Newborn (TTN) & Meconium Aspiration Syndrome)
Jaundice
Infection/Sepsis
Polycythemia
Phenylketonuria (PKU)
Neonatal Alcohol Withdrawals (NAS)
Intraventricular Hemorrhage
Retinopathy
Necrotizing Enterocolitis
Pie de foto: : APGAR Scoring
Diapositiva 2
Amniocentesis (pg. 306 McKinney)
What is it? Aspiration of amniotic fluid from amniotic sac for examinationWhen is it performed?
Best between 15 and 20 weeks due to increased amniotic fluid
Can be done as early as 11 to 14 weeks
Why is it performed?
Second Trimester:
detect fetal abnormalities such as Rh incompatibility
AFAFP (amniotic fluid alpha fetal protein) level indicates neural tube defects (only when Maternal Serum AFP was abnormal)
Third Trimester
Fetal lung maturity
Evaluate hemolytic disease of the newborn
Reduction amniocentesis (extra fluid removed or fluid removed for evaluation of infection or harmful substances)
Diapositiva 3
Amniocentesis
How is it performed?
woman lies supine
FHR and maternal BP monitored
US used to locate fetus, placenta, and location of amniotic fluid
About 20 mL removed for analysis
Rhogam given to Rh- women
EFM for 30 to 60 min
Diapositiva 4
Fetal Lung Maturity (amniocentesis)
Lecithin/Sphingomyelin (L/S) ratio
best test for estimation
L&S are lipoproteins that make up surfactant
Surfactant keeps alveoli open by decreasing surface tension, preventing collapse with exhalation, and reducing effort of breathing
Interpretation: both L&S are equal until about 30 weeks, then Lecithin is produced more
Want 2:1 ratio by week 34/36
Diapositiva 5
Extrauterine Transition of Lungs (pg. 467 McKinney)
Before BirthFetal lungs are filled with fluid that aids in development, production of fluid decreases closer to termDuring LaborFluid begins to shift from alveoli into the interstitial spaces where it can be absorbed (may last hours after birth)As baby cries fluid shifts into the
Diapositiva 6
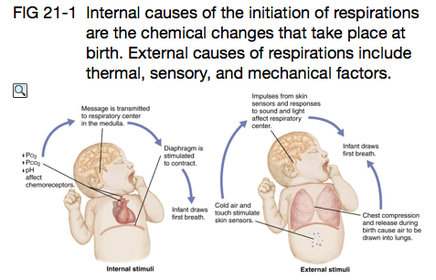
Causes of Respirations: Chemical stimuli (decreased oxygen, increased CO2, decreased pH)Thermal stimuli (temperature change)
Sensory (touch)
Mechanical (compression and release of thorax when passing through birth canal
Transition of Lungs
{kind=link}
Pie de foto: : Causes of Respirations
Diapositiva 7
Transition of Lungs
Babies at risk for complicationsThose under weeks 34/36Give mothers in preterm labor steroids to increase surfactant productionLungs should be clear by 24 hours
Diapositiva 8
Transient Tachypnea of Newborn (TTN)
Rapid respirations after birth d/t inadequate absorption fetal lung fluid, usually resolves within 24 to 72 hours
Risk Factors: C-section, fast delivery, male, perinatal asphyxia, maternal diabetes or asthma
S/S: 60 to 120 breaths/min within hours of delivery, retractions, nasal flaring, grunting, cyanosis
DX: chest x-ray shows hyperinflation and streaking of fluid
TX: oxygen, gavage feedings, observe for sepsis (similar S/S)
Diapositiva 9
Changes in Cardiovascular System
Ductus VenosusVein carries maternal oxygenated blood past liver and into inferior vena cava that closes with cutting of the cordDuctus ArteriosusConnects pulmonary artery and aorta before delivery, is stimulated to constrict when oxygen levels rise with first breathForamen Ovale Foramen between R and L atrium. Closes with increase pressures in L. side of heart as pulmonary vessels are utilized with breathing
Diapositiva 10
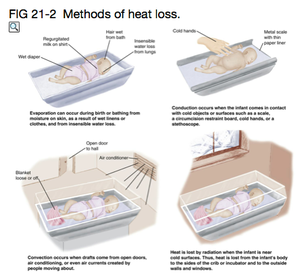
Thermoregulation
Predisposing factors:thin skin, blood vessels close to surface, little white (SQ) fat, increase body surfaces area related to massMethods of heat loss: Evaporation: air drying/insensible water lossConduction: removal of heat with contact of cold objects/surfacesConvection: transfer of heat to cooler surrounding air/draftsRadiation: transfer of heat to objects not in direct contact with infant
{kind=link}
Diapositiva 11
Effects of Cold Stress
Increased metabolism (loss glucose, increased oxygen needs, decreased brown fat reserves)
Risk for respiratory distress d/t decrease in production of surfactant, increased oxygen needs, and vasoconstriction of pulmonary blood vessels
hypoglycemia/ increased acid production
metabolism of brown fat increases release fatty acids (further increases acidity and can interfere with transport bilirubin-lead to hyperbilirubinemia)
Vasoconstriction of peripheral blood vessels to conserve heat
Prevention:Neutral thermal environment (89-92 degrees when undressed, 75 to 80 degrees when dressed)NOTE: hyperthermia can also cause hypoglycemia in newborn and should be prevented
Diapositiva 12
{kind=link}
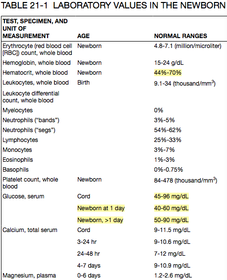
Hematologic differences in Newborns
Increased Hgb (25-24 g/dL) that also has higher affinity for oxygen!
Increased Hct (40-70%)- Polycythemia (>65%) increases blood viscosity and risk for hyperbilirubinemia and complications of blood clots
Glucose is lower (40-60 mg/dL day 1 and 50-90 mg/dL after)
WBC's increased (9000-34000 at birth, falls to 12,000 by day 4 or 5)
Clotting deficiency (little Vit. K)
Diapositiva 13
Meconium Aspiration Syndrome (719)
Meconium: First stool, passed within 12 hours of birth typically, 48 hours at the latest. Appears greenish black with a thick, sticky consistency.Let provider know as soon as you identify meconium in the amniotic fluid!!!!! MAS:
Obstruction, air trapping and chemical pneumonitis cause by meconium in infants lungs.
Most common on post term infants
Caused by hypoxia that increases peristalsis of intestines during labor
S/S:Respiratory distress, tachypnea, cyanosis, retractions, nasal flaring, grunting, rales, barrel chest shape with hyperinflation, see-saw breathingManagement: Suctioning as soon as head comes out, warm humidified oxygen, extensive respiratory support
Diapositiva 14
Bilirubin
Unconjugated (Indirect bilirubin): not soluble in water, must be changed to water soluble form by liver by conjugationFat soluble may be absorbed by SQ fat causing JaundiceConjugated (Direct bilirubin): soluble in water and can be excreted and is not toxic to the bodyJaudice is normal and occurs in about 60% of term and 80% of preterm infants!
Diapositiva 15
Hyperbilirubinemia
Causes/Risk Factors: Excess production of bilirubin d/t polycythemia and RBC breakdownFaster breakdown of fetal RBC'sLiver immaturityBlood incompatibility (Rh, ABO)Gestation: preterm and late term have immature conjugation abilitiesFeeding: delayed feeding decreases amount of bilirubin excreted in fecesTrauma from birth (cephalohematoma) increases RBC destructionFamily background: native american, asian, or eskimo infants have increased risk
Diapositiva 16
Types of Jaundice
Physiological/Non-pathological:Appears 2nd or 3rd dayTSB is 5-6 mg/dLShould be gone by 1 week!Breastfeeding JaundiceBegins first week of life, may last monthsTSB may be > 12 mg/dLCaused by insufficient breast milk for feeding or bad feeding patterns (decreased bilirubin excretion)
Non-physiologic/ Pathologic:Appears within first 24 hours lifeBilirubin rises fast and quick Caused by Rh incompatibility, infection, excessive RBC damage or problems with conjugation, and certain metabolic disorders
Diapositiva 17
Complications of Hyperbilirubinemia
Bilirubin Encephalopathy: increased bilirubin deposits in brain and can cause neurological changesLethargy, decreased muscle tone, poor feeding, decreased reflexes, crying, and seizuresKernicterus: permanent neurological damage from bilirubin encephalopathy/prolongued untreated hyperbilirubinemia
Diapositiva 18
Management Hyperbilirubinemia
PHOTOTHERAPY (Bilirubin lights):
begin at lower TSB levels for premies, protect eyes, keep unclothed and warm
light conjugates bilirubin to be excreted
Frequently check TSB levels (every 8 hours)Can measure TCB (transcutaneous bilirubin) with BilirubinometerExchange transfusion: removes RBC's and bilirubin and replaces with healthy bloodGet the baby feeding!!! (Every 2 to 3 hours) increase excretion, milk also has laxative effectINDIRECT COOMBS TEST: identify Rh incompatibility
Diapositiva 19
Infection in Neonates (pg. 724)
Transmission:Before birth: rubella, cytomegalovirus, syphilis, HIV, toxoplamosis can cross the placentaDuring birth: group B streptococci (GBS), herpes, hepatitis may infect infant after ROM
Diapositiva 20
Sepsis in Neonates
Infants are at great risk d/t immature immune system!
Common causes: GBS, E. coli, Staphylococcus, Hib, Candida albicans. Pneumonia and Meningitis most commonly seen
Early onset Sepsis: within first 24 hours, may be first week. HIGH mortality
Late onset Sepsis: after 1st week of life, usually a localized infection such as meningitis
DX: CBC (WBC's might not increase, decrease in platelets), elevated C-RP, blood, urine and CSF cultures
Diapositiva 21
Sepsis in Neonates
SymptomsMay be subtle but include temperature change, respiratory complications, altered feeding, changes in color of skin, changed blood glucose readings, lethargy, irritability, decreased muscle tone, high pitch cryTXAntibiotic therapy during labor for mother infected with GBS, antibiotic therapy after birth for infected infant, symptom management (oxygen, mechanical ventilation), garage feedings, fluid monitoring, vitals
Diapositiva 22
Prenatal Drug Exposure (pg. 729)
Most drugs readily cross the placenta and cause a variety of problems
NAS (neonatal abstinence syndrome)
Symptoms depend on substance used and usually appear within first 24 to 72 hours and can last up to 4 weeks!
Drugs that cause withdrawals: Codeine, hydroxyzine, amphetamines, antidepressants, heroin
SX: lethargy, irritability, tremors, increased tone, easily distressed, crying, poor suck reflex, vomiting/diarrhea
Increased risk for: SIDS, FAS, decreased growth/fetal maturity, respiratory distress, jaundice
Diapositiva 23
Prenatal Drug Exposure
Treatment: Specific to symptoms.May test infant meconium or urine to detect substance50-60% need Rx therapy: Tincture of Opium, oral morphine, methadone, phenobarbitolGavage or IV feedingsDecreased stimulation (noise, light, calm/slow approach, few people at a time, swaddle)Breast feeding may be indicated as it contains trace amounts of substance which will help with withdrawals
Diapositiva 24
Phenylketonuria (PKU)
Genetic disorder that causes CNS injury from toxic levels of amino acid phenylaline in blood
Deficiency in enzyme (phenylaline hydrolase) that converts phenylaline to tyrosine
SX: digestive problems (vomiting), seizures, intellectual impairment
TX: low phenylaline diet for life!
All infants are screened for PKU after 24 hours before they leave the birthing center
Diapositiva 25
Maternal Child Book
McKinney, E., James, S., Murray, S., Nelson, K., & Ashwill, J. (2013). Maternal child nursing (4th ed.). St. Louis, MO: Saunders Elsevier.
¿Quieres crear tus propias Diapositivas gratis con GoConqr? Más información.