6744618
Descripción
Fichas por Andrew Street, actualizado hace más de 1 año
|
|
Creado por Andrew Street
hace alrededor de 8 años
|
|
| Pregunta | Respuesta |
| 3614 List causes of burns. | * Wet heat/scalds - most common * Dry heat * Chemical * Electrical * Radiation * Cold See lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Burns+-+Miss+J.+Odili.pptx |
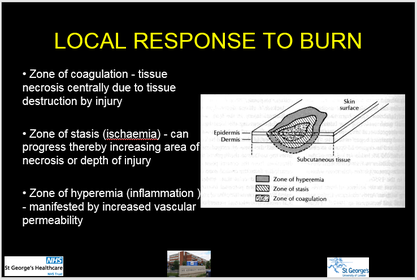
| 3615 What three zones are seen within a burn injury? | |
| 3615 Outline the local response to a burn. | * Inflammatory mediators cause increased micovascular permeability, oedema formation, microvascular stasis, thrombosis * These responses can lead to progressive injury & cell death leading to deeepening of the wound See lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Burns+-+Miss+J.+Odili.pptx |
| 3617 Explain how burns can affect tissues & organs other than the skin. | Systemic response to burns: * In larger burns (>25-30% TBSA) mediators are released into the circulation (PG's, LT's, free radicals, histamine)- these effect all organs * Burn oedema - oedema of burned & non-burned tissues. Pro * Impaired microvascular integrity leads to burn oedema (oedema of burned & non-burned tissue). Protein loss peaks at 8-12 hrs. * Hypovolaemia * Myocardial depression * RBC destruction - up to 40% of circulating volume * Glucose intolerance See lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Burns+-+Miss+J.+Odili.pptx |
| 3616 Describe the classification of burns by thickness of burn. | * Erythema: > Epidermal damage > No skin loss > Heals within days without scarring Superficial partial thickness (eg's flash burns, sunburn, some hot water scalds): > Pink, moist, blistered > Blanch on pressure > Very painful > Predominantly epidermal loss (germinal layer intact) > Heals within 3 weeks > Minimal scarring * Deep partial thickness (eg's some hot water scalds, hot fat, contact burns): > White / red with fixed staining > No blanching on pressure > Loss of germinal layer epidermis > Prolonged healing by migration of epidermal cells from appendages & edges > Scarring > Sometimes/often needs skin grafting * Full thickness (eg's flame burns, prolonged contact burns, corrosive chemicals): > Leathery & insensate > Loss of entire dermis > Will not heal unless very small > Scarring & contractures > Needs skin grafting See lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Burns+-+Miss+J.+Odili.pptx |
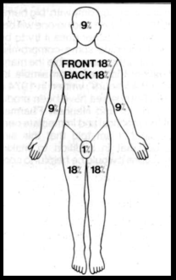
| 3618 Describe the use of the rule of nines in the assessment of a pt with burns. | |
| 3620 Discuss factors which influence prognosis following a burn. | Factors in burn severity: * Burn location - hands, feet, genitalia * Age * Pre-existing medical conditions * Medications * Presence of multi-systems trauma * Inhalation injury See lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Burns+-+Miss+J.+Odili.pptx |
| 3621 Describe the immediate first aid steps in the management of a pt with burns. | STOP THE BURNING WOUND! * Extinguish flames - pt horizontal * Remove affected clothing (unless melted to skin) * Cold water or wet towels (beware hypothermia) * Clingfilm * Continuous irrigation of chemical burns * No other topical agents (toothpaste, butter, eggs) See lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Burns+-+Miss+J.+Odili.pptx |
| 3622 Explain which pt's with burns need in-pt Mx. | Criteria for referral to burns unit: * >10% TBSA in children * >15% TBSA in adults * Face, hands, feet, genitalia, perineum, major joints * Circumferential burns * Electrical burns * Inhalation injury * Significant pre-existing medical conditions, co-existing trauma * NAI See lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Burns+-+Miss+J.+Odili.pptx |
| 3623 Describe the emergency Mx of pt's with severe burns. | * Airway & C-spine: > Deal with any obstruction > Collar if suspicion of spinal injury > If any evidence of impending obstruction (stridor, oropharyngeal swelling) get senior help/anaesthetist * Breathing: > High flow O2 > Check COHb & ABG > If circumferentional burns of chest consider escharotomy > CXR * Analgesia: > IV access - large bore x 2 > BD's - x-matching, FBC, COHb, U & E, glucose, coagulation > IV morphine titrated to response + antiemetic (eg 50mg cyclizine IV) * Fluid resuscitation: > Start with isotonic crystalloid (eg 0.9% saline) at 2-4mL/kg per % TBSA burned over 24 hrs (half of the volume in 1st 8 hrs) > Catheterise & test urine (myoglobinuria = ^risk of renal failure) > R/V fluids frequently - aim for urine output >50mL/hour in adults > Monitor BP & RR > Burns >10% TBSA may require RBC transfusion Oxford Handbook of Emergency Medicine. |
| 3624 List the acute complications of burns & describe measures to prevent them. | Early complications: * Impaired renal function * Haemoglobinuria * Overtransfusion * Infxn & impaired immune function * Pulmonary damage * Burn encephalopathy * Toxic shock syndrome * Malnuitrition (may occur later) See lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Burns+-+Miss+J.+Odili.pptx |
{kind=link}
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.