15753120
Descripción
Mapa Mental por Caitlin Parliament, actualizado hace más de 1 año
|
|
Creado por Caitlin Parliament
hace alrededor de 6 años
|
|
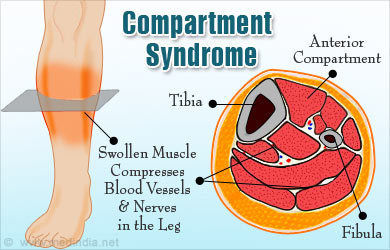
Acute Compartment Syndrome is a
condition that occurs with an
increase in pressure in a confined
space or compartment that results in
decreased blood flow to tissues (Lewis
et al., 2017; Papachristos &
Giannoudis, 2018; Walls, 2017)
- Causes
- Decreased compartment size
(Lewis et al., 2014)
- Restrictive dressings
- can cause
increased
pressure on
the
compartments
- can cause
increased
pressure on
the
compartments
- Splints
- Casts
- Excessive
Traction
- Premature closure of
fascia
- Restrictive dressings
- Increased
compatment
contents (Lewis et
al., 2014; Wall, 2017)
- Fractures
(Wall, 2017)
- Closed
- Open
- Complete
- Incomplete
- Long bone
fractures
including the
humerus and
tibia
- Closed
- Soft Tissue injuries
- More common in older
ages
- Subluxation,
Dislocation, Strains &
Sprains causing
edema and blood to
increase within the
compartments
- More common in older
ages
- Intravenous Infiltartion
- Resulting in an increase
in pressure from fluid
build up
- Resulting in an increase
in pressure from fluid
build up
- Bleeding
- Edema
- Chemical response to snake bite
- Resulting in an increase in
pressure from
inflammation and the
immune response
- Resulting in an increase in
pressure from
inflammation and the
immune response
- Trauma
- Volkmann's
ischemic is
compartment
syndrome in
the upper limb
- Anterior tibial
compartment
syndrome occurs
in the lower limbs
- Volkmann's
ischemic is
compartment
syndrome in
the upper limb
- Crush
injuries
- Blood and swelling cause
an increased pressure
with in the compartment
- Blood and swelling cause
an increased pressure
with in the compartment
- Fractures
(Wall, 2017)
- Decreased compartment size
(Lewis et al., 2014)
- Risk Factors
(Papachristos
& Giannoudis,
2018)
- Age
- Under 35 years old
- This s because younger people
tend to have more muscle in a
compartment compared to older adults
- This s because younger people
tend to have more muscle in a
compartment compared to older adults
- Adolescents
- Have the biggest rate of
tibial fractures
- Have the biggest rate of
tibial fractures
- Under 35 years old
- Male
gendered
Nota:
- (Papachristos & Giannoudis, 2018)
- 7.3 per 1000, 000 in men
compared with 0.7 per
100,000 in wom
- Age
- Pathophsyology
(Lewis et al., 2017;
Papachristos &
Giannoudis, 2018;
Walls, 2017)
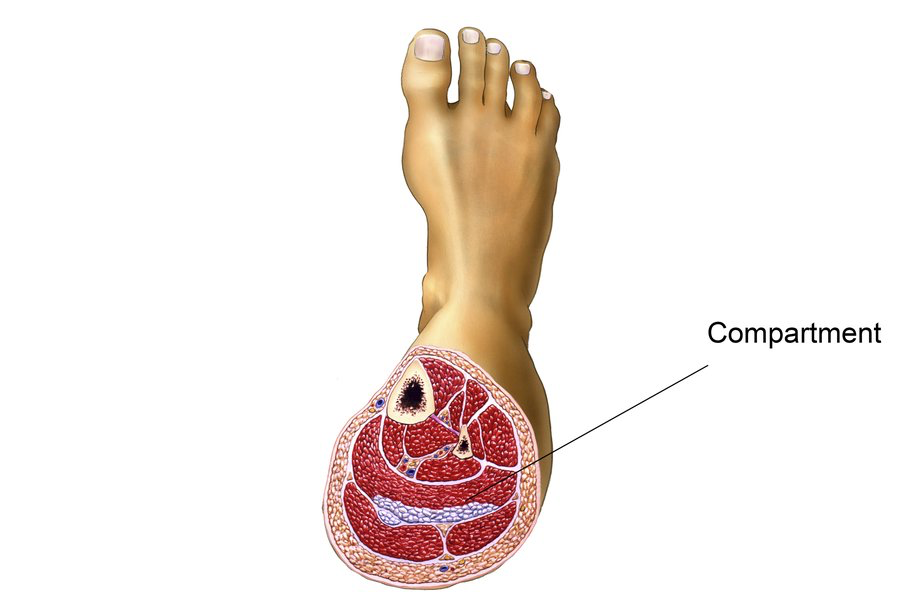
- Muscles
are
made
of
compartments,
which
house
the
nerves
and
blood
vessels.
- When the pressure of
the compartments
increase the fascia does
not stretch which
results in impaired
tissue perfusion. This
leads to ischemia,
capaillary bed damage
causing plasma to leak
out resulting in edema
and nerve damage
- Necrosis of tissue occurs with compartment
pressures over 30 mm Hg, this happens in
about 4-8 hours (Lewis et al., 2014)
- Lack of oxygenated
blood leads to tissue
hypoxia which causes
an increase in waste
product accumulation
and muscle tissue
damage
- Cellular destruction
results in myoglobin being
realesed into the
bloodstream, also there is
a release of creatine
kinase which, in high
amounts, can lead to
rhabdomyolysis. Both are
life threatening
conditions that can cause
acute renal failure
(Papachristos &
Giannoudis, 2018; Walls,
2017)
- Hyperkalemia and acid is
released into the blood
which can cause
dysrhythmias, organ
failure and death
- Cellular destruction
results in myoglobin being
realesed into the
bloodstream, also there is
a release of creatine
kinase which, in high
amounts, can lead to
rhabdomyolysis. Both are
life threatening
conditions that can cause
acute renal failure
(Papachristos &
Giannoudis, 2018; Walls,
2017)
- Necrosis of tissue occurs with compartment
pressures over 30 mm Hg, this happens in
about 4-8 hours (Lewis et al., 2014)
- The outer covering that encloses
and separates muscle from other
organs is called the fascia, it does
not stretch. The normal
compartment pressure range is 0-8
mm Hg.
- When the pressure of
the compartments
increase the fascia does
not stretch which
results in impaired
tissue perfusion. This
leads to ischemia,
capaillary bed damage
causing plasma to leak
out resulting in edema
and nerve damage
- Muscles
are
made
of
compartments,
which
house
the
nerves
and
blood
vessels.
- Clinical manifestations
- The 6 P's (Lewis
et al., 2017;
Papachristos &
Giannoudis, 2018;
Walls, 2017)
- Pain which is described
as intense, deep and
difficult to localize. Pain
increases with passive
stretch and as the
pressure increases
- Paresthesia or pins
and needles is a sign
of impaired
circulation
- Pallor is seen distal to the injury, cyanosis and mottling
may also be present. The affected area can also look
shiny, tense and swollen. This is caused by impaired
circulation and increased capillary pressure
- Paralysis is considered a
late sign and is more
common with crush
injuries. Motor function is
lost if the limb is ischemic
(Wall, 2017)
- Pulselessness at or
just below the injury
due to impaired
circulation, this is
also seen as a late
finding
- Pressure is from decreased
compartment size or
increase in compartment
contents. 30 mm Hg or
higher indicates
compartment syndrome
(Lewis et al., 2014)
- Pain which is described
as intense, deep and
difficult to localize. Pain
increases with passive
stretch and as the
pressure increases
- The 6 P's (Lewis
et al., 2017;
Papachristos &
Giannoudis, 2018;
Walls, 2017)
- Diagnosis
(Papachristos
&
Giannoudis,
2018)
Nota:
- (Papachristos & Giannoudis, 2018)
- Specific clinical
signs- The 6 P's of
compartment
syndrome
- Intra compartmental pressure
(ICP) messurements are
essential, peak pressure is 5
cm distal and proximal to
fracture site. ICP of 30 mm Hg
indicates compartment
syndrome
- Infrared spectroscopy is a
new non-invasive tool that
messures tissue
oxygenation with a probe
that goes on the skin
- pH monitoring- due to
anerobic cellular activity
acidosis can occur,
intra-compartment pH of
<6.4 indicates compartment
syndrome
- MRI to detect
intra-compartmental
swelling however this
finding is non-specific
- Complications if left
untreated (Pearse &
Nanchahal, 2008)
- Complications are directly corrolated with
timing of treatment
- Myoglobin may be realsed from damaged
muscle causing kidney damage and acute
renal failure
- The ischaemic muscle becomes
necrotic and replaced by fibrous
tissue causing weakness,
disfiguration and nerve damage
- Ectensive tissue necrosis may require amputation,
widespread damage may result in death
- Nerve damage leads to lack o
sensation, muscle paralysis
and neurogenic pain
- Infection, locally or systematically
- (Rangel, Hernandez-Castro, Arenas, Dominguez-Cherit,
Vick, Diaz, Rodriguez-Cruz, 2010)
- (Rangel, Hernandez-Castro, Arenas, Dominguez-Cherit,
Vick, Diaz, Rodriguez-Cruz, 2010)
- Ectensive tissue necrosis may require amputation,
widespread damage may result in death
- Further complications are dependent
on the compartment that is affected
- Complications are directly corrolated with
timing of treatment
- Treatment
- Fasciotomy is an incision into the
skin and fascia allowing for the
affected muscle to swell, releasing
tension and pressure (Schmidt,
2017)
- Emergency surgical procedure
- General anaesthesia is used,
offering the highest level of
patient sedation. The patient
loses all sensation, total loss
of consciousness and
inability to self maintain
functional airway.
- Aseptic technique to
minimize risk of
infection
- General anaesthesia is used,
offering the highest level of
patient sedation. The patient
loses all sensation, total loss
of consciousness and
inability to self maintain
functional airway.
- Complications
- Must be done immediately or
irreversible tissue necrosis
occurs
- Additional surgery for delayed
wound closure, skin grafts, cosmetic
issues, pain and nerve injury
- Permanent muscle weakness
- Chronic venous insufficiency
- Must be done immediately or
irreversible tissue necrosis
occurs
- Wound closure (Bengezi &
Vo, 2013)
- Alleviating edema by strictly
elevating the affected limb
- Wound cloure time was
three to five days with
elevation
- Practical in settings with
limited resources
- Wound cloure time was
three to five days with
elevation
- Split-thickness skin grafting,
which involves removal of
the epidermis and a portion
of the dermis
- Six to eight days to
restore full
circulation to the
skin graph
- (Reynolds, Christophersen, Mulcahey, 2017)
- (Reynolds, Christophersen, Mulcahey, 2017)
- Ten to twelve days
for the donor site to
heal
- Six to eight days to
restore full
circulation to the
skin graph
- Alleviating edema by strictly
elevating the affected limb
- Emergency surgical procedure
- Fasciotomy is an incision into the
skin and fascia allowing for the
affected muscle to swell, releasing
tension and pressure (Schmidt,
2017)
- Nursing Interventions
- Drug therapy is individualized (Ersek &
Polomano, 2014)
- Non-opioids/Nonsteroidal
anti-inflammatory drugs
(NSAIDs). Used for mild to
moderate pain, promotes
blood clotting and encourages
normal function of the
kidneys. They work by limiting
the production of
prostaglandins that promotes
inflammation, pain and fever.
- Opioids are used for
moderate to severe acute
pain. They work by
attaching to opioid
receptors in your brain, and
those cells release signals
that muffle the perception
of pain
- Adjuvant analgesic therapy
are drugs used in
conjunction with opioid and
nonopioid analgesics.
- Adjuvant analgesic therapy
are drugs used in
conjunction with opioid and
nonopioid analgesics.
- Non-opioids/Nonsteroidal
anti-inflammatory drugs
(NSAIDs). Used for mild to
moderate pain, promotes
blood clotting and encourages
normal function of the
kidneys. They work by limiting
the production of
prostaglandins that promotes
inflammation, pain and fever.
- Therapeutic Relationships:
Composed of significant knowing
and meaningful connecting with
patients (Mirhaghi, Sharafi, Bazzi &
Hasanzadeh, 2017)
- Barriers
- Staff shortages
- Time restraints
- Sterotyping
- Staff shortages
- To be effective the nurse
needs to be self-conscious,
self-aware, have a philosophy
about life, death and the
overall human situation
- Features
- Mutual targeted
experience
- Meeting nursing
needs of the
individual and family
- Coordination and
cooperation
- Being near the
patients bedside
- Honesty and empathy
- Mutual targeted
experience
- Barriers
- Patient education is put
into place to help patients
and their caregivers focus
on optimizing their health
and to enable them to
cope with health problems
(Goodridge, 2014)
- Clinical patient
education: planned,
systematic,
sequential and
logical process of
teaching and
learning
- Health education:
focuses mostly on
wellness, prevention
and health promotion
- Clinical patient
education: planned,
systematic,
sequential and
logical process of
teaching and
learning
- Use a pressure monitor/catheter to
measure intra-compartmental tissue
pressure to ensure it does not exceed
30mmHg (Harvey, 2006).
- Drug therapy is individualized (Ersek &
Polomano, 2014)
- (Pediatric, 2018)
- (Compartment syndrome- NHS, 2016)
- (Compartment Syndrome, 2018)
- (Vector - Man was Leg Ache and Pain,
2018)
- (Wadhawan, Upadhyay, Sabboubeh, Hussainy& Madan, 2007)
Recursos multimedia adjuntos
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propios Mapas Mentales gratis con GoConqr? Más información.