11816729
Description
Flashcards by Anna Hogarth, updated more than 1 year ago
|
|
Created by Anna Hogarth
almost 8 years ago
|
|
| Question | Answer |
| How much of the total ECF does plasma make up? What are the two major components of blood? | 1) 20% 2) Plasma - 55% (solutes - 10%; water - 90%) and haematocrit/formed elements - 45% (Leukocytes and thrombocytes - main proportion is RBCs) |
| What are the components of plasma? | 90% is water which functions as a solvent, lubricant, cushion and heat dissipator. 2% is glucose, salts and other dissolved chemicals. 8% is proteins - albumin, globulin and fibrinogen. |
| How much do each of the three classes of protein contribute to the total amount of protein in the plasma? What is the function of each? | 1) Albumin - 60% - transport and intravascular oncotic pressure 2) Globulin - 36% - immunity 3) Fibrinogen - 4% - blood hemostasis (clotting cascade) N.b. there are also proteins involved in the inflammatory response such as complement proteins (cell lysis, chemotaxis, opsonisation and permeability) and cytokines (such as interferons) |
| What are the different plasma ions? What are their functions? (2) | 1) Inorganic ions - potassium, sodium, chloride, calcium, bicarbonate, phosphate 2) i) Maintain blood pressure and support contraction of skeletal and cardiac muscle. ii) Carbon dioxide is dissolved in the blood and exists as carbonic acid, hydrogen or bicarbonate - either free or bound to proteins, including haemoglobin - maintenance of pH |
| What is the carbonic buffer equation in the blood? What is the point of this? How does haemoglobin bind hydrogen? | 1) H+ + HCO3- --- H2CO3 --- H20 + CO2 2) Can absorb the hydrogen produced from various metabolic activities to prevent metabolic acidosis 3) Hydrogen binds to the histidine residue in the haemoglobin |
| How are nutrients vs. waste products carried in the plasma? What else is carried in the plasma? | 1) Nutrients are dissolved in the plasma whereas waste products (such as aurea, uric acid, creatinine and bilirubin) are bound to plasma proteins. 2) Hormones, drugs and alcohol (e.g. chemicals) |
| Describe the hematopoiesis cascade | Bone marrow cells form either myeloid or lymphoid stem cells. i) Lymphoid stem cells give rise to lymphoblasts --- T cells, B cells and NK cells. ii) Myeloid stem cells give rise directly to RBCs, megakaryocytes and myeloblasts. ---Megakaryocytes give rise to platelets. --- Myeloblasts give rise to eosinophils, basophils and neutrophils |
| What is the function of erythrocytes? What do they contain/not contain? Average lifespan? How many are made per hour? What (mainly) controls RBC production? What does this mean in terms of pathology? | 1) Carriage of O2 from lungs to tissue 2) Haemoglobin - don't contain a nucleus so are biconcave 3) 10^10/hour 4) Erythropoeitin 5) Erythropoietin is produced in the kidneys - kidney failure can lead to anaemia |
| Describe the structure of haemoglobin. What happens when O2 binds? What is the Bohr effect and what triggers it? | 1) Haemoglobin is made of four globin chains (4); 2a and 2B. Contains an iron-containing heme group 2) When O2 binds there is a conformational change from a to B 3) In the presence of H+, CO2 and 2,3-DPG the release of O2 is promoted |
| How many people does anaemia affect worldwide? What are the haemoglobin levels associated with men in anaemia? Women? | 1) 25% 2) 130 g/l 2) 115 g/l |
| What is anaemia? What is the bodies response to anaemia? | 1) Not a diagnosis - there is always an underlying cause. Either decreased production (most common cause) or losing too much 2) Decreased oxygen carriage to kidneys results in increased production of erythropoietin which leads to increased production of RBC in the bone marrow |
| What are the symptoms of anaemia? | 1) Tiredness 2) Faint 3) Worsening of angina 4) Short of breath 5) Rapid heart beat - experienced as palpations |
| What are the signs of anaemia? | 1) Pale 2) Bounding pulse 3) Systolic flow murmur 4) Cardiac failure 5) Rapid heart beat 6) Retinal haemorrhage |
| What are the three different classes of anaemia? | 1) Microcytic (mean cell volume is less than 80 femtoliters) 2) Normocytic (mean cell volume is between 80-100 femtoliters) 3) Macrocytic (mean cell volume is greater than 100 femtoliters) |
| What are the underlying causes of microcytic anaemia? | 1) Iron deficiency 2) Thalassemia Cause the cells to be small due to lack of iron/haemoglobin |
| What causes normocytic anaemia? | 1) Acute blood loss 2) Long term chronic disease (e.g. infection or malignancy) 3) Renal failure 4) Sickle cell disease 5) Leukemia |
| What can cause macrocytic anaemia? | 1) Liver failure 2) B12/folic acid deficiency 3) Alcohol |
| What are the common underlying causes of iron deficiency anaemia (microcytic cells, hypochromic)? | 1) Diet - rare 2) Menstruation 3) Growth spurts, pregnancy 4) Infection (hookworm) 5) Gastrointestinal loss - e.g. bleeding ulcers, IBD and cancers |
| How big are platelets? What is there lifespan? How many are produced every second? | 1) 2-3ul 2) 10 days 3) 1 million/second Come from megakaryocytes produced in the bone marrow |
| What are the two components which contribute to the formation of a thrombus? What happens as a result of too low levels of either of these? | 1) Platelets initiate the clotting cascade - form a platelet plug. Clotting proteins then lead to the formation of a firm thrombus 2) Thrombocytopenia - bruising and bleeding. Too low levels of clotting proteins (haemophilia) does the same. |
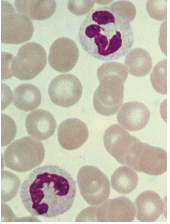
| Which is the most common WBC? Describe its structure. What is its half life? How many are produced per second? What is its function? | 1) Neutrophils 2) Larger than white blood cells, 2-4 lobes, granules don't stain - appear clear 3) 6-8 hours 4) 1 million per second 5) Destruction of bacteria |
| X | |
| When is there an increase in the concentration of neutrophils? What causes a deficiency (neutropenia)? | 1) Infection, inflammation, tissue damage and haemorrhage 2) HIV, B12/folate acid deficiency, leukemia, bone marrow failure, overwhelming sepsis (blood poisoning) |
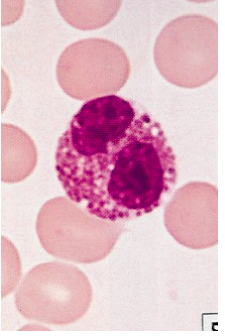
| What is this? Describe its features. When does its concentration increase? | 1) Eosinophil 2) Bilobed and bright orange granules 3) Parasitic infection, asthma, skin disorders |
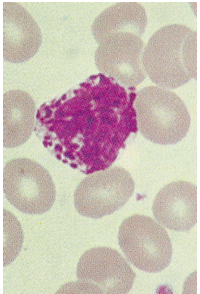
| What is this? Describe its characteristics. | 1) Basophil 2) 2-3 lobed nuclei, blue granules |
| What is this? Describe its characteristics. What is its primary function? When does it increase? | 1) Monocyte - similar to myeloid progenitor cells 2) Kidney shaped nucleus 3) Turns into a macrophage - present antigen to lymphocytes 4) In response to chronic and viral infections (although more important generally to bacterial) |
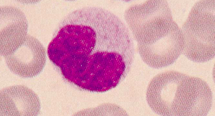
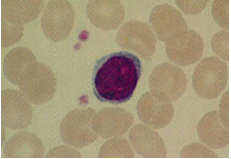
| What is this? Describe its characteristics. What can it become (and what are the function of those cells). When do these increase? Lifespance? | 1) Lymphocyte 2) Small and dense, little cytoplasm, large round nucleus. 3) T cell (coordinate immune response), B cell (produce antibodies), NK cells (viral and tumour immunity) 4) During viral infections (and in cancers) 5) 1 week to 1 year |
| What can bone marrow failure lead to? What can cause bone marrow failure? What tends to actually kill people with bone marrow failure? | 1) Fatigue, bleeding and death 2) Leukemia, aplastic anaemia, chemotherapy, toxins and radiation, B12/folate deficiency 3) The neutropenia |
| What are the different counts which can be done to detect haematological disorders? | Full blood count: 1) RBC - absolute numbers (10^12/L) and mean cell volume 2) Haemoglobin - amount in whole blood; mean cell Hb (pg)(reduced if cells are small); Mean cell Hb (%)(reduced if Hb is low) 3) Packed cell volume/haematocrit (ratio or %) 4) Platelet count - absolute number (x10^9/L) 5) White cell count (X10^9/L) or white cell differential - i.e. different types which are seen |
| What is used to prepare a blood film? What is the purpose of a blood film? What is the final blood test which could be used? | 1) Fixed with alcohol, stained with May-Grunwald Giemsa 2) Used to examine the morphology of cells 3) Bone marrow biopsy |
| X |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.