12076235
Description
Flashcards by Dolu Falowo, updated more than 1 year ago
|
|
Created by Dolu Falowo
almost 7 years ago
|
|
| Question | Answer |
| How thick is the synovial membrane in a synovial joint? | 2-3 cells thick |
| What gives synovial joints their stability? | Fibrous capsule Ligaments Muscles |
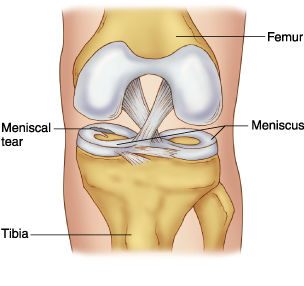
| What does the meniscus in the knee do? | Meniscus: extra area of cartilage in the knee only -Crescentic plates of fibrocartilage -Increases congruity of articular surface |
| What are the clinical presentations of knee pain? | -Pain + stiffness -Overlying skin is hot/red -Swelling in suprapatellar pouch -limited knee movement -limp on walking -history of leg giving way -trauma |
| What are signs of inflammation? | Redness, swelling, warmth |
| What are the common causes of knee pain? | -Infection (septic arthritis-treatable) -Crystal arthritis (ie. gout-caused by increase in uric acid) -Osteoarthritis -Chronic inflammatory arthritis (ie. RI) -Trauma (to menisci, ligaments or tendon) -Bursitis |
| Define infective (septic) arthritis In which populations is it more common in? | Inflammation of a joint caused by bacterial infection Children/elderly People with diabetes Debilitated |
| How do bacteria gain access? | -Local trauma -Spread from adjacent sites of infection -Bloodstream |
| What are the pathological changes due to septic arthritis? | -Ioint destruction (osteomyelitis) -Can drain to the surface via a sinus -Bone formation stimulated -Ankylosis -Dislocation |
| What are the signs on a X-ray of septic arthritis? | -Loss of joint space -Lytic areas -Erosion on bone edge -New bone formation (looks denser) |
| What is gout? In which populations is it more common in? | A crystal induced arthritis due to the deposition of uric acid crystals in joints which leads to inflammation -Men (middle age onwards) -Post-menopause -Hypertensive patients |
| Describe the aetiology of gout | Primary: idiopathic -impaired excretion of uric acid by kidney (?genetic) Secondary: -Increased production of uric acid eg. in high alcohol consumption -Impaired excretion by kidneys due to disease/drugs (diuretics) |
| What are the pathological changes of goat? | -Cartilage degeneration -Synovial hyperplasia -Erosion of bone -Secondary degenerative change (eg. osteoarthritis) -Tophaceous depositis of uric acid in skin |
| What is osteoarthritis/crepitus? In which populations is it more common in? | Degenerative disease leading to joint failure. There is a disregulation of normal tissue turnover + repair 60+ years |
| Describe the aetiology of osteoarthritis | Primary Secondary: -complications of other joint disorders |
| Pathological changes with osteoarthritis? | -Involve cartilage, bone, synovial and joint capsule with secondary effects on muscle -Fibrillation/erosion of articular cartilage -Pseudocysts |
| What are the radiological changes of osteoarthritis? | -Joint space narrowing -Subchondral bone sclerosis and cysts -Marginal osteophyte formation |
| What is rheumatoid arthritis? In which populations is it more common in? | Chronic inflammatory joint disease -Females -Onset occurs between 35-45 years old |
| What is the aetiology of rheumatoid arthritis? Clinical manifestations? | Autoimmune -Symmetrical deforming polyarthritis -Diffuse small joint involvement (hands/feet. Larger joints can be affected) -Can be associated with non-articular disease |
| What pathological changes does rheumatoid arthritis result in? | -Rheumatoid synovial hyperplasia and inflammatory infiltration which can result in pannus formation (abnormal layer of fibrovascular/granulation tissue) -Invasion + destruction of articular cartilage -Erosions |
| What radiological changes would be seen in rheumatoid arthritis? | -Soft tissue swelling -Joint space narrowing -Osteopenia (reduce bone density) -Erosions |
| What is the temporomandibular joint (TMJ)? Where is it found? | The joint formed by the articulation of the mandible with the cranium. Modified synovial joint Anterior to and vertically level with the tragus of the ear |
| What are the superior and inferior articulatory surfaces of the TMJ? | Superior: -Under surface of the squamous part of the temporal bone -2 articular sites: mandibular fossa (posterior and concave) and articular tubercle (anterior and convex) Inferior: -Condyle of the mandible has a rounded superior edge and ellipsoid circumference with its major axis postero-mandial (oblique) |
| Describe the movement of the TMJ | Movement in the mediolateral plane and opening/closing |
| Describe the features of the TMJ | -Fibrous capsule -Capsule is very strong -Capsule is thin and loose to permit movement (has laxity) -Has a meniscus to prevent bony surfaces making direct contact -Upper and lower cavity present on either side of the meniscus |
| What does the presence of the upper/lower cavities of the TMJ allow? | Upper cavity: translational movements due to a gliding joint Lower joint: rotational movements due to a modified hinge joint |
| What are the articulating surfaces of the upper/lower joint cavity? What is the purpose of the meniscus? | Upper: under surface of the temporal bone and upper surface of the articular disc Lower: inferior surface of the articular disc and the mandibular condyle Meniscus improves congruity |
| What lines the articulatory surfaces of the TMJ? | -Fibrocartilage (can withstand big forces eg. bites) -At birth, the fibrocartilage is lined by synovial membrane |
| Describe the articular disc/meniscus of the TMJ | -Composed of dense fibrous connective tissue -Upper surface is concavo-convex (antero-posteriorly) -Under surface is concave to fit condyle of mandible -Thicker at periphery where it attaches to the articular capsule (thinner centrally) -Incompressible -Can recoil/stretch a bit due to its attachments |
| What are the capsular attachments of the TMJ? | Superior: circumference of the mandibular fossa and articular tubercle Inferior: neck of condyle of the mandible |
| Green- TMJ ligament Orange- Joint capsule Red- Stylomandibular ligament Purple- Sphenomandibular ligament | |
| Describe the TMJ ligament | -Strongest ligament of TMJ -Deep fibres blend with the capsule -Attaches to lower border of zygoma to posterior border of neck and ramus of mandible -Tightens the head in retrusion (closing + pulling jaw backwards) |
| Describe the sphenomandibular ligament | -Accessory ligament -Remains constant in length and tension -Prevents inferior dislocation of the joint -Originates from the sphenoid spine to attach to the mandible |
| Describe the stylomandibular ligament | -Accessory ligament -Extends from apex of the styloid process to the posterior border of the ramus of the mandible near its angle -Tickening of parotid gland fascia -Separates parotid gland from submandibular gland |
| Describe the stabilisation of the TMJ | -More stable when jaw is closed since mandibular condyle are in contact with mandibular fossa -Teetch are in occlussal contact when jaw is closed (ie. zig-zag) -Least stable when jaw is open -Liable to spontaneous dislocation in people who lack teeth |
| What happen during opening movements of the TMJ? | -Condyles are pulled forwards (protrusion)- a gliding movement. The lateral pterygoid muscles are involved -Chin is pulled down and back, a hinge movement. This involves the digastric muscles |
| What happen during closing movements of the TMJ? | -Retraction of the mandible by the posterior fibres of the temporalis muscles (pull mandible backwards) -Elevation of the mandible by the rest of the temporalis muscles, masseter muscles and medial pterygoid muscles |
| What anatomical factors are present to add stability to the TMJ? | Post glenoid tubercle: limits posterior displacement Articular tubercle: limits passive anterior displacement Sphenomanibular/stylomandibular ligament: inferior dislocation |
| What are some disorders of the TMJ? | -Knacking -Bruxism Temporomandibular pain dysfunction disorders -Mal-occlusal syndromes (teeth do not align properly) |
| What are the general features of fibrous joints? Examples? | -Don't allow movement/locomotion -Any movement is not normal/pathological Syndesmosis (sheet of fibrous tissue uniting bones eg. interosseus membrane between ulna/radius) and gomphosis (joint between tooth and socket) |
| Diagram of a fibrous joint? | |
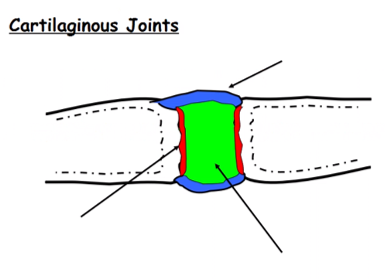
| Describe a cartilaginous joint | Primary cartilaginous joint: united by hyaline cartilage. Usually a temporary joint during growth Secondary cartilaginous joint: articular surface covered in hyaline cartilage. Bones are united by strong fibrocartilage and strong joints allow slight movement |
| Blue- fibrous capsule Green- fibrocartilage (movement between bone ends) Red- hyaline cartilage | |
| What are synovial joints? What specialised features do they contain? | -Provides free movements Features: -articular discs (fibrocartilage pads) which act as shock absorbers -fibrocartilage ring (labrum) which deepens joints esp ball and socket joints -tendons |
| 6 common features of synovial joints | -Bone ends covered in articular (hyaline) cartilage -Connective tissue capsule -Joint cavity -Inner surface is lined with synovial membrane -Reinforced by ligaments -Wide range of movements |
| Describe the specialisation of the hip joint as a synovial joint | -Head of femur is deep into the socket -Ligament is inside the joint capsule -The hip is rarely dislocated (compared to the shoulder) but movement is limited |
| What covers the surface of the tibia in the knee joint? | 2 Menisci (form a C shape on either side) with 2 articular cartilages in the centre This prevents wear/tear as there is no bone/bone grinding |
| Describe the glenoid labrum Purpose of it? | A fibrocartilaginous 'lip' around the glenoid cavity of the scapula Acts to deepen the cavity for better articulation |
| What is the rotator cuff? Contents? | A specialised muscle group which fixes the head of the humerus into the glenoid cavity. It increases stability to a joint that is prone is dislocation. Supraspinatus, infraspinatus, teres minor, subscapularis |
| Describe the dislocation of the shoulder joint Consequences? | -Humeral head rarely moves upwards during dislocation due to presence of coracoid process -Dislocation occurs inferiorly and the head lies in a subcoracoid position (under coracoid process) -Tears joint capsule and can damage to axillary nerve (since it wraps around the head of the humerus) -Damage to the axillary nerve can result in loss of sensation to skin of regimental badge area (deltoid muscle) |
| What happens in a pulled elbow? | -Radial head is subluxed -Radial head is held in place by a annular ligament -Ligament is softer in children so is more prone to dislocation (eg. when child is lifted up by the arm) |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.