12116342
Description
Flashcards by Laura Gennaro , updated more than 1 year ago
|
|
Created by Laura Gennaro
over 6 years ago
|
|
| Question | Answer |
| Upon exposure, contaminated pulp acts as a conduit between... | the oral cavity and alveolar bone |
| What is an important defense mechanism alerting to need for therapeutic intervention? | Pulpitis-related pain |
| Pulpitis: Main types of causative noxious stimuli | -Bacterial= caries -Mechanical= trauma, iatrogenic damage from dental procedures -Thermal= extensive cavity preparation, large uninsulated metal restoration |
| What is the crossover point from reversible to irreversible pulpitis? | Invasion of the pulp by bacteria |
| Reversible pulpitis | tissue capable of returning to a normal state of health if noxious stimuli removed |
| Irreversible pulpitis | dental pulpal tissue damaged beyond point of recovery |
| Reversible pulpitis details | -Tooth acutely painful to stimuli >>discomfort resolves within few seconds >>responds to electric pulp testing (EPT) at lower levels of current than control tooth -Mobility and sensitivity to percussion absent -Dentin sensitivity may produce similar symptoms -Cracked tooth and defective restoration often present if pain upon biting |
| Irreversible pulpitis details | -Tooth acutely painful to stimuli >>Discomfort continues for longer period of time >>Responds to electric pulp testing (EPT) at lower current than control tooth -Throbbing pressure in later stages -With increasing discomfort patient may be unable to identify offending tooth >>Pulpal pain may be referred between arches, but should not cross the midline |
| Pulpal necrosis | -Tooth fails to respond to EPT or thermal sensitivity testing -Symptoms vary from none to acute pain |
|
Chronic hyperplastic pulpitis (pulp polyp)
Image:
Image (binary/octet-stream)
|
-Unique, uncommon pattern of pulpal inflammation -Occurs with large exposures of pulp in which entire dentinal roof is missing -High level of chronic inflammation produces hyperplastic granulation tissue that extrudes from chamber |
| Is a biopsy necessary for the diagnosis of pulpitis? | No, there is a surprising lack of correlation between histopathologic findings and clinical symptoms |
| Primary dentin | formed before completion of crown |
| Secondary dentin |
formed after completion of crown
-dentin physiologically continues to be deposited along inner walls
-Leads to smaller pulp chambers/canals w/ age
-Significant traumatic injury may lead to early obliteration of pulp chamber/canal (calcific metamorphisis)
Image:
Image (binary/octet-stream)
|
| In what disease is early widespread formation of secondary dentin seen in association with? |
Progeria
Image:
Image (binary/octet-stream)
|
| Tertiary dentin |
laid down in response to focal injury
-triggered by injury of peripheral odontoblastic
-in response to caries, trauma, dental procedures
Image:
Image (binary/octet-stream)
|
| Dental Calcifications | Prevalence: approx. 20% of radiographs -Idiopathic, associated with aging -Increased prevalence in context of chronic pulpal irritation (attrition, caries, dental restorative procedures) -Noted in association w/ certain disease processes (uncommon) |
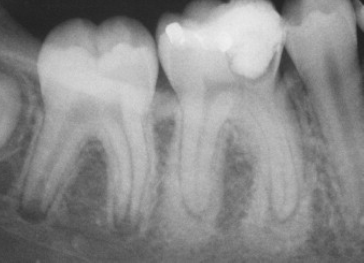
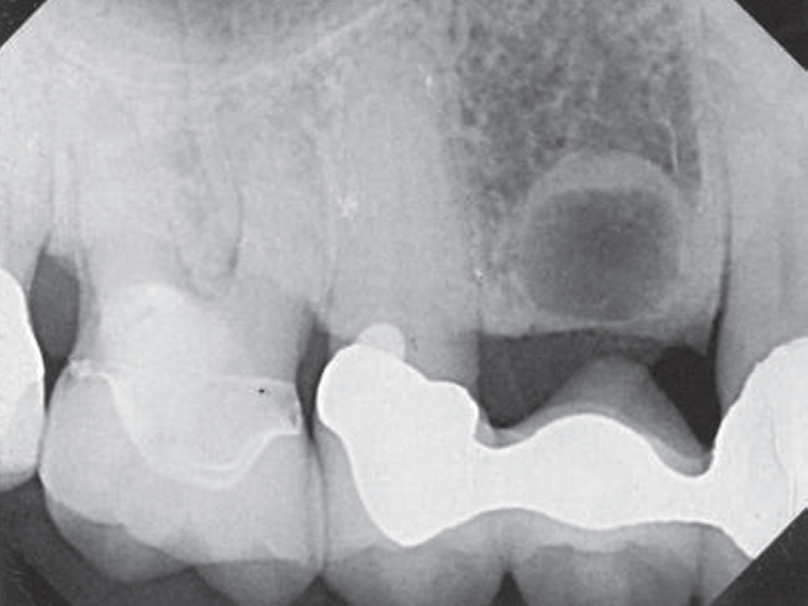
| Condensing Osteitis |
-localized areas of bone sclerosis associated w/ teeth exhibiting pulpitis
-uniform area of increased radiodensity adjacent to apex of tooth
-thickened PDL or apical inflammatory lesion often present
-no clinical expansion
Image:
Image (binary/octet-stream)
|
| What percent of condensing osteitis cases regress with extraction/treatment of the involved tooth? | ~85% |
| Bone scar |
residual area of condensing osteitis remaining after resolution of inflammatory focus
Image:
Image (binary/octet-stream)
|
| Idiopathic Osteosclerosis | -asymptomatic focus of increased bone production -tends to arise in 1st-2nd decade -Prevalence: 5-10% -Seen in various tooth & non-tooth bearing areas of the jaws -Associated dentition vital -needs to be distinguished from condensing osteitis |
| Acute Apical Periodontitis |
-early stage of infection in which neutrophils predominate
-widening of PDL space radiographically
-pain on biting/percussion
-constant dull, throbbing pain
Image:
Image (binary/octet-stream)
|
| Chronic Apical Periodontitis |
-neutrophils release prostaglandins which activate osteoclasts to resorb bone, leading to detectable periapical radiolucency, and chronic inflammatory cells dominate
-often asymptomatic
-pain and sensitivity in context of acute exacerbation
Image:
Image (binary/octet-stream)
|
| Acute Inflammation | -initial, rapid response to infection or tissue damage -exudation of fluid/plasma proteins -migration of PMNs (neutrophils) |
| Chonic inflammation | -response of prolonged duration to infection or tissue damage -characterized by varying combinations of: >>continued inflammation >>continued tissue injury >>attempted tissue repair (granulation tissue, angiogenesis, fibrosis) |
| G | wound healing tissue comprised of: -fibroblasts (deposit collagen) -endothelial cells (form capillaries; angiogenesis) -scattered leukocytes (mainly macrophages) |
| Fibrosis | -healing by connective tissue replacement (scarring) -represents end result of granulation tissue: >>fibroblasts in granulation tissue secrete collagen >>granulation tissue ultimately converts to fibrous tissue (called organization) |
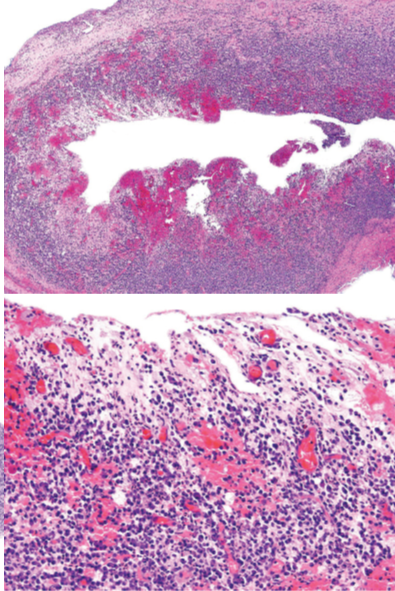
| Abscess | -specific pattern of ACUTE inflammation -represents a localized collection of purulent inflammatory tissue (pus) -most frequently due to infection with bacteria that are pyogenic |
| Pus | exudate rich in neutrophils, dead cell debris, microbes |
| Resolution of periapical pathology cannot occur as long as... | pulpal infection is active -rationale behind RCT/extraction |
| Periapical Pathology: Progression to chronic inflammation | -periapical granuloma -radicular/periapical cyst |
| Periapical granuloma | -a tumor-like mass of granulation tissue -inflammatory response can be associated w/ orifice of main canal or can be associated w/ a lateral canal that is infected -usually asymptomatic and associated w/ infected tooth (pain & sensitivity may occur w/ acute exacerbation) NOT a real granuloma |
| Radiographic appearance of Periapical Granuloma |
-radiolucency varies from small to >2cm in diameter
-apical lamina dura usually lost
-circumscribed or ill-defined
-cortical expansion, root resorption may rarely occur
Image:
Image (binary/octet-stream)
|
| Pathology of Periapical Granuloma |
-removed tissue consists chiefly of granulation tissue w/ admixture of acute/chronic inflammation & variable amounts of organizing fibrous tissue
Image:
Image (binary/octet-stream)
|
| Granuloma | -collection of activated macrophages, often w/ T-lymphocytes -represents attempt to contain an offending agent that is difficult to eradicate (foreign material that is relatively inert, persistent microbes) -limited number of diseases cause granulomatous inflammation |
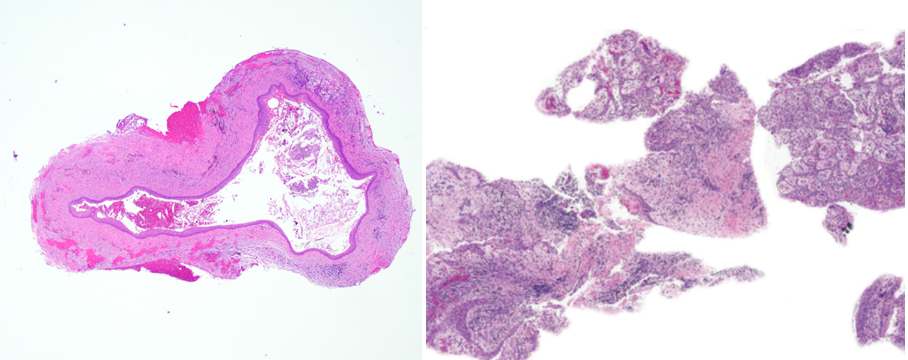
| Radicular (periapical) cyst |
-represents the exact same inflammatory response seen in periapical granuloma PLUS epithelium
-in the presence of surrounding inflammatory milieu, otherwise quiescent epithelium may be stimulated to proliferate
-proliferation may assume the morphology of a cyst or may proliferate haphazardly amongst the granulation tissue
Image:
Image (binary/octet-stream)
|
| Where does the epithelium in Radicular cysts come from? | Incomplete disintegration of HERS (Hertwig's Epithelial Root Sheath) yields clusters (rests) of quiescent epithelial cells in PDL space -Epithelial rests of Malassez |
| Residual Radicular Cyst |
consequence of tooth extraction without curettage
Image:
Image (binary/octet-stream)
|
| Periapical Fibrous Scar | -on occasion fibrous tissue (organized granulation tissue) is not remodeled into alveolar bone during healing -most commonly occurs when facial & lingual cortical plates destroyed by initial periapical insult -results in periapical radiolucency indistinguishable from periapical granuloma/radicular cyst |
| Management of Non-abscessed periapical radiolucencies | -often resolve following root canal therapy or extraction w/ curettage -persistent lesions may require apicoectomy (tissue should be submitted to pathology since expected resolution did not occur w/ RCT) -periapical fibrous scars= no treatment theoretically but difficult to diagnose preoperatively |
| Other things seen microscopically | -Endodontic materials -Pseudostratified ciliated epithelium (sinus mucosa due to oroantral communication; occasionally metaplastic change to cyst lining) -Rushton bodies -Hyaline ring granulomas |
| Rushton bodies | -peculiar structures seen in <10% of odontogenic cyts -represents amalgamation of keratin secretion and hemorrhage (from ruptured cysts) |
| Hyaline Ring Granulomas | -granulomatous inflammation around poorly-digestible, hyalinized, ring-shaped material -plant-based food penetrate tissues through extraction sockets or grossly carious dentition -incidental finding |
| Periapical abscess | -abscess at the apex of a non-vital tooth -may arise as initial periapical pathosis or from acute exacerbation of chronic periapical inflammation -may be symptomatic or asymptomatic |
| Symptomatic Periapical Abscess | caused by accumulation of purulent material within alveolus -tenderness/pain upon percussion and palpation -tissue swelling -constitutional signs/symptoms may be present |
| Asymptomatic Periapical Abscess | especially if abscess is able to drain -intraoral sinus tract w/ parulis -cutaneous sinus tract |
| Complications of abscess | -cellulitis (soft tissue) -osteomyelitis (bone) -sepsis (blood) (Risk of dissemination less for abscesses that drain freely) |
| Where do most dental abscesses perforate? Where do maxillary lateral incisors, palatal roots of maxillary molars, and mandibular 2nd-3rd molars frequently drain? | -perforate buccally because the bone is thinner -Drain palatally/lingually |
| Management of Periapical Abscess | -Drainage & elimination of focus of infection (treatment w/ NSAIDs pre-op & for post-op pain control) -Antibiotic coverage for well-localized and easily drained abscess in healthy patient unnecessary -Signs/symptoms diminish within 48hrs -Sinus tract resolves spontaneously after treatment of offending tooth |
|
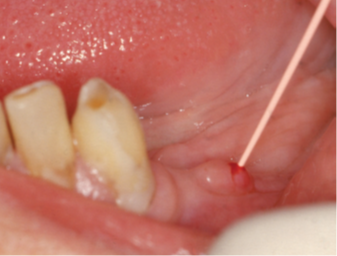
Parulis (gumboil)
Image:
Image (binary/octet-stream)
|
-small, exophytic mass of granulation tissue at opening of sinus tract into oral cavity -compressible & fluctuant -typically asymptomatic (abscess can drain) -patient may report foul/salty taste in saliva (from pus) -resolves w/ treatment of underlying periapical/periodontal disease |
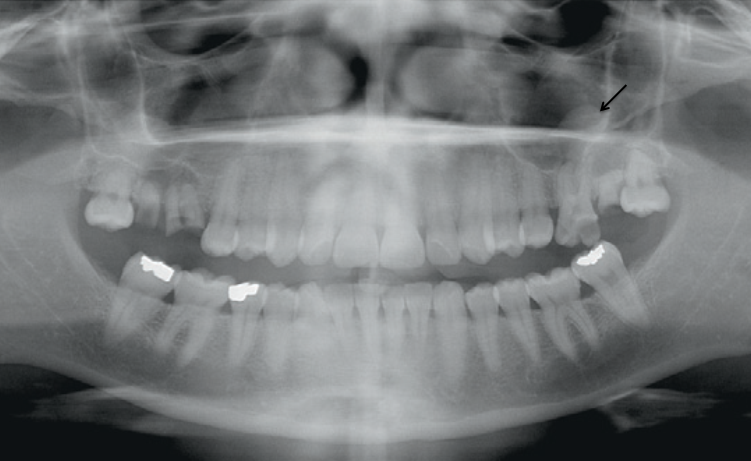
| Antral Pseudocyst | -focus of inflammation located within maxillary sinus -typically asymptomatic and discovered incidentally on radiographs -cause unknown but adjacent odontogenic infection contributory in some cases (treatment of offending tooth when applicable) -treatment otherwise unnecessary; surgical removal if symptomatic |
|
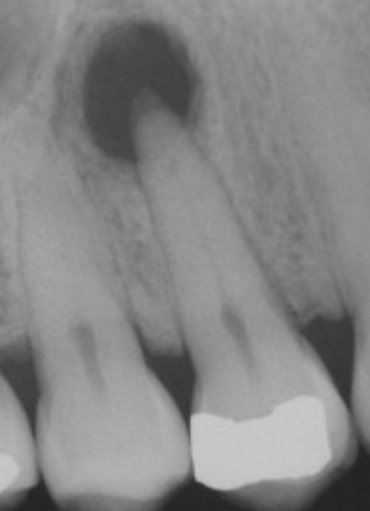
Radiographic features of Antral Pseudocyst
Image:
Image (binary/octet-stream)
|
-Spherical
-Dome-shaped
-Uniform radiodensity arising from floor of maxillary sinus
-Inflammatory exudate located immediately beneath mucosal sinus lining
-Cortical bone remains intact below lesion (would be displaced superiorly if disease was intraosseous)
Image:
Image (binary/octet-stream)
|
| Actinomycosis | -serious, chronic infectious bacterial infection caused primarily by genus Actinomyces |
| Top 3 clinical presentations of Actinomycosis | -Cervicofacial (55%) -Abdominal (20%) -Thoracic (15%) |
| Actinomyces | -members of endogenous flora of mucous membranes (oral cavity, colon, vagina, bronchi) -disruption of mucosal barrier integral pathogenicity of Actinomyces (tooth extraction, grossly carious tooth, mandibular fracture) |
| Periapical actinomycosis | -clinical presentation may or may not be more aggressive than routine periapical disease -sinus tract formation or perforation of buccal/lingual cortical plates -asymptomatic |
| Prognosis/Treatment | -Excellent prognosis with minimal antibiotic coverage -Removal of all tissue at time of apicoectomy/surgical excision prerequisite -Antibiotic coverage for 1 week at discretion of clinician |
| Osteomyelitis | -inflammation of bone and marrow spaces -virtually always secondary to infection: >>complication of open fractures, surgical procedures, diabetic infections of foot >>secondary to bacteremia stemming from minor skin infections or trivial mucosal injury |
| The vast majority of osteomyelitis cases are caused by... Most common types of osteomyelitis | -bacterial infection -Suppurative osteomyelitis (Acute, Chronic) -Tuberculous osteomyelitis -Proliferative periostitis |
|
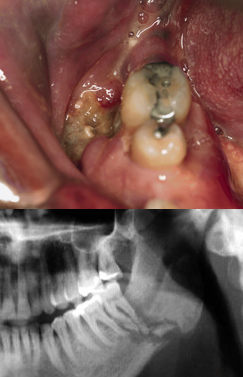
Osteomyelitis of gnathic bones
Image:
Image (binary/octet-stream)
|
-mandible affected more frequently (poor vascular supply) -75% male predilection Etiology: -Acute dental infection -Radiation treatment -Hypovascular bone conditions |
| Acute dental infection | -usually in context of predisposing condition (fracture, irradiation, diabetes mellitus, steroid therapy) -most dental infections do not cause osteomyelitits |
| Hypovascular bone conditions | -cemento-osseous dysplasia -paget disease of bone -osteopetrosis |
| Acute suppurative osteomyelitis of the gnathic bones |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.