5736773
Description
Flashcards by Amelia Claire, updated more than 1 year ago
|
|
Created by Amelia Claire
over 8 years ago
|
|
| Question | Answer |
| respiratory system | |
| Primary Functions of Respiratory System | Gas Exchange surface area moves air to and rom lungs protects respiratory surfaces from the outside environment produces sounds olfactory sense participation |
| Conducting Portion of Respiratory System | UPPER SYSTEM Nose & Pharynx LOWER SYSTEM Larynx Trachea Bronchi Terminal Bronchioles |
| Respiratory Portion of the Respiratory System | part of the LOWER SYSTEM Smaller respiratory bronicholes Alveoli This is where gas exchange occurs |
| Functions of the Nose | Warming, moistening, filtering air Olfaction Modifying speech vibrations Air enters the respiratory system through nostrils into nasal vestibule, hair = defence, filtration. |
| Pharynx / Throat | Nasopharynx (superior), tonsils & eustachian tube (equalises pressure in eardrum) Oropharynx (middle) Laryngopharynx (inferior) Hyoid bone to entrance of larynx and oesophagus |
| Respiratory Epithelium | Psuedostratified columnar epithelium, mucous cells (goblet cells) and glands in lamina propria cilia on epithelial cells moves mucus up toward the mouth = mucociliary escalator part of defence system also macrophages and neutrophils |
| irritants cause hyper production of mucus | Lung cancer, COPD, emphysema Bacterial Infections Cystic Fibrosis |
| Lung Lobes | Right = 3 Lobes Horizontal and oblique fissures Left = 2 Lobes Cardiac notch and oblique fissures |
| Trachea anterior to oesophagus | c shaped cartilage provides support, prevents trachea from collapsing allows food to pass through oesophagus |
| trachea extends to: | mediastinum here it breaches off to the right and left pulmonary bronchi |
| bronchial tree | 23 generations getting progressively smaller |
| Primary Bronchus | branches to form secondary bronchi (lobar bronchi) one secondary bronchus goes to each lobe |
| Secondary Bronchi | branches to form tertiary (segmental) bronchi each segmental bronchus supplies air to a single bronchopulmonary segment each time they divide they have less cartilage with the smallest having no cartilage |
| Bronchioles | dynamic airways; no cartilage have smooth muscle innervated by ANS and stimulated by circulating adrenaline |
| Parasympathetic system impact on Bronchioles | Constriction |
| Sympathetic Nervous System and Adrenaline's impact on bronchioles | dilation |
| Parasympathetic Nervous System affect on ARTERIOLES | Dilation |
| Sympathetic and Adrenaline impact on ARTERIOLES | constriction |
| bronchioles are sensitive to local chemicals | specifically CO2 and O2 |
| Bronchioles are dynamic | they have the capacity to change in diameter (CO2 is a dilator, sympathetic ns and adrenaline are also dilators) (parasympathetic NS is a constrictor) |
| bronchopulmonary lobule | each lobule begins from a terminal bronchiole and contains lymphatics arterioles capillaries venules |
| terminal bronchiole subdivides; | into several respiratory bronchioles beginning the respiratory zone. they branch into alveolar ducts, each leading to an alveolar sac, consisting of alveoli |
| Alveolar Type 1 Cells (predominant) | simple squamous epithelial cells long cytoplasmic extensions form alveoli walls site of gas exchange surrounded by capillaries |
| Alveolar type 2 Cells (interspersed) | cuboidal microvilli produce pulmonary surfactant; consists of lipids and proteins to reduce surface tension. |
| Alveolar Macrophages (move around) | phagocytosis, remove pathogens, dust, debris |
| Gas Exchange | |
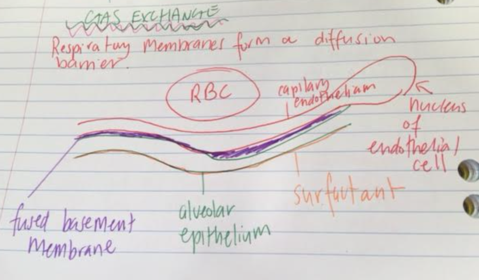
| Diffusion Barrier | 3 Parts to the Membrane Squamous epithelial lining of alveolus Endothelial cells lining adjacent capillary fused basal laminae between alveolar and endothelial cells |
| Fick's Law of Diffusion R inverse to A ΔP / d or R = D(constant)A ΔP/d | The rate of diffusion (R) Gas or molecule across an atom is: 1. Proportional to the area of the membrane (A) 2. Inversely proportional to the thickness of the membrane (d) 3. Proportional to the difference in concentration ( ΔC) or partial pressure (ΔP) |
| diffusion = | D(constant) x Area x Partial Pressure / thickness of membrane |
| blood supply to respiratory surface | each lung lob receives an arteriole and a venule (own blood supply) Respiratory exchange surfaces receive blood from arteries of the pulmonary circuit -- a capillary network surrounds each alveolus as part of the membrane; blood form alveolar capillaries passes through venues and veins and returns to L atrium. |
| Pleural Membranes / Pleural Sac | mediastinum separates thoracic cavity into two distinct compartments; pleural membranes encase each lung. contains lubricating fluids secreted by membranes, and enables them to be cohesive but smooth |
| parietal pleura | outer layer attached to wall of thoracic cavity |
| visceral pleura | inner layer covering surface of the lung |
| 3 processes of respiration | pulmonary (breathing) external (circulation of gases) internal (cellular respiration) |
| Pulmonary Ventilation (breathing) | physical movement of air in and out of respiratory tract; air moves from an area of HIGHER pressure to LOWER pressure |
| external respiration | 1. pulmonary ventilation 2. gas diffusion at lungs and tissues 3. transport of gases |
| Pulmonary Ventilation | Air moves from an area of high pressure to low pressure The volume of thoracic cavity changes with expansion or contraction of the diaphragm or rib cage, resulting in change in pressure. |
| Boyle's Law | Pressure is INVERSELY proportional to Volume |
| Pressure differentials created by changes in lung volume | Atmospheric Pressure (Patm) = 760mmHg Intrapulmonary Pressure (PpI) at rest = 760mmHg = 0 difference Intrapleural Pressure = 756mmHg |
| Inhalation | Active Process - Contraction of the diaphragm and external intercostal muscles expands the thoracic cavity, ↑ volume => ↓ in intrapulmonary pressure relative to atmospheric pressure Air flows down pressure gradient into lungs |
| Exhalation | Passive Process relaxation of muscles, elastic recoil of chest wall and lungs due to recoil of elastic fibres, inward pull of surface tension of alveolar fluid. Volume ↓ pressure ↑ air flows out of lungs |
| Muscles involved in deep breathing | Inhalation: Sternocleidomastoid (elvates sternum) Scalene (elevates first 2 ribs) Pectoralis Minor (elevates 3-5 ribs) Exhalation: Abdominals and internal intercostals |
| Intrapleural Pressure | 756mmHg - lower than Patm and PpI due to elastic lung constantly pulling on visceral membrane; the pressure is sub atmospheric as the pleural sac is completely enclosed. The pulling by the lung depressurises the intrapleural cavity, |
| tranpulmonary pressure gradient | acts across the lung wall; sucks the lung outward and adhered to thoracic cavity |
| intraplueral fluid | the cohesive forces of fluid filled intraplueral fluid resits separation of the membranes' water molecules are best friends and like to stick together; this means that the lung does not recoil and collapse. |
| Factors Affecting Pulmonary Ventilation | lung compliance elastance surface tension of alveolar fluid airway resistance |
| Factors Affecting Pulmonary Ventilation: Lung Compliance | Effort / force required to stretch or distend lungs (ΔV/ΔP) most work is to overcome resistance of elastic recoil and the stiff thoracic cavity Less compliant requires more work and ↑ pressure to produce given degree of inflation |
| Factors Affecting Pulmonary Ventilation: Elastance | inverse to compliance; how readily the kings will rebound after being stretched. This is due to elastic fibres in alveolar tissue and interstitial spaces Due to surface tension at air-liquid interface (surfactant) |
| Factors Affecting Pulmonary Ventilation: surface tension of alveolar fluid | surfactant reduces the surface tension and increase lung compliance and DECREASES elastance |
| Airway Resistance | Airflow is inversely proportional to airway resistance determinant of resistance is radius inverse proportionality Resistance proportional 1/r4 |
| Factors Affecting Pulmonary Ventilation: Pathology - COPD, Emphysema, chronic bronchitis Cause by inflammatory response by lung; | macrophages and neutrophils attempt to manage irritants (smoke, toxins, etc), produce excess PROTEASES that break down protein, use lay antiproteases will prevent damage but Chronic response damages alveoli and digests it - fewer alveoli, less surface area, loss of elasticity, floppy lungs, air trapped. |
| obstructive diseases | difficult to expire emphysema asthma bronchitis |
| Restrictive Diseases | difficult to inspire Respiratory Distress Syndrome Lung fibrosis |
| Lung Volume | Residual ~ 1200ml (always in lungs) tidal volume ~ 500ml (normal breathing) Inspiratory reserve + ~ 3100 ml (max) |
| vital capacity | total amount of air you can move in maximal inspiration and maximal expiration |
| Alveolar Ventilation (takes part in gas exchange) | 150ml anatomical dead space respiratory rate x tidal volume breathing efficiency affected by rate and volume |
| gas exchange | occurs between alveolar air and blood; passive diffusion - occurs down partial pressure gradients |
| Fick's Law | Diffusion proportional to surface area, concentration gradient, partial pressure and permeability. Inversely proportional to distance. |
| Dalton's Law | each gas in a mixture exerts its own pressure (the partial pressure) proportional to its concentration in the mixture and independent of other gases present. total pressure x fractional concentration in mixture = partial pressure |
| henry's law | quantity of the gas that dissolves in liquid is proportional to its partial pressure and the solubility coefficient -> increasing pressure drives a gas into solution until equilibrium established when gas pressure decreases, dissolved molecules leave solution until a new equilibrium is established (=gas and liquid molecules of the gas) |
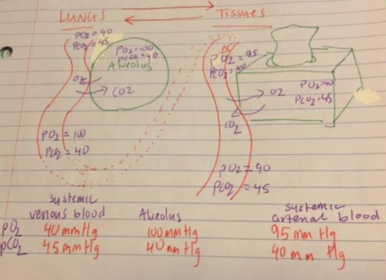
| composition of air | N2 =79% => 760mmHg x .79 = 600mmHg pp O2 = 21% => 760mmHg x .21 = 160mmHg |
| pulmonary gas exchange | Alveolar PO2 100mmHg Atmospheric PO2 160 mmHg |
| gas exchange | |
| transport of oxygen | most O2 is transported by haemoglobin Hb+O2 <=> HbO2 Deoxyhaemoglobin <=> oxyhaemoglobin haemoglobin must bind reversibly to O2 so it can load in lungs and unload in tissues |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.