5995269
Description
Flashcards by Andrew Street, updated more than 1 year ago
|
|
Created by Andrew Street
over 8 years ago
|
|
| Question | Answer |
| 1560 List risk factors for HIV infxn. | * Needle sharing with IV drug use * Unprotected receptive anal intercourse * Unprotected receptive penile-vaginal sexual intercourse * Percutaneous needle stick injury * High maternal viral load (mother to child transmission - aka vertical transmission). See http://bestpractice.bmj.com/best-practice/monograph/555/diagnosis/history-and-examination.html |
| 1561 How are the majority of HIV infxns transmitted (which fluids)? | * Semen * Cervical secretions * Blood. KAC p172. |
| 1561 Distinguish between HIV positivity (how is this done?) and AIDS. | HIV = measurable infection (recommended 1st line assay tests for HIV AB's & p24 antigen). European definition of AIDS is based on Dx of specific clinical conditions whereas in the US this is combined with CD4 counts <200. KAC p175. |
| 1562 Who should be offered HIV testing? | Universal HIV testing is recommended in all the following settings: GUM & sexual health clinics / antenatal services / TOP services / drug dependency services / services for those with Dx TB, HBV, HCV, lymphoma. HIV testing should be routinely offered & recommended to: pt's with a DDx of HIV / Dx of an STI / partners with those HIV +ve / all MSM & any partners / IVDU / those who report sexual contact abroad or in UK with those from a country of high prevelance. HIV testing should also be routinely performed in the following groups: BD donors / dialysis pt's / organ transplant donors & recipients / members of staff with needlestick injuries. See http://patient.info/doctor/hiv-counselling |
| 1564 Describe the key elements included in counselling a patient for HIV testing. | * The benefits of testing to the individual * Clear details of how the results will be given * Why it's particularly recommended in some groups Issues raised by the patient about the test and HIV infection. Such issues often include: * Risk and lifestyle * Benefits of knowing HIV status and treatment possibilities * What tests are available and which is recommended * The window period for testing * Seroconversion * The difference between HIV and AIDS * Confidentiality. Certain pt's may need more time & explanation eg english 2nd language, young people, MH and learning difficulties. See http://patient.info/doctor/hiv-counselling |
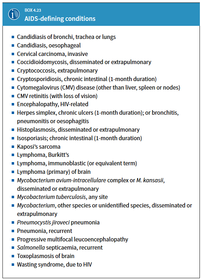
| 1565 List common opportunistic infxns from which pt's with AIDS may suffer. | |
| 1566 Describe the use of CD4 count in the Mx of HIV infection. | The absolute CD4 count and its percentage of total lymphocytes falls as HIV progresses. These figures bear a relationship to the risk of the occurrence of HIV-related pathology, with patients with counts below 200 cells at greatest risk. Rapidly falling CD4 counts and those below 350 are an indication for HAART. CD4 counts are performed at approximately 3-monthly intervals unless values are approaching critical levels for intervention, in which case they are performed more frequently. KAC p178. |
| 1566 Describe the use of viral load in the Mx of HIV infection. | The rate of viral clearance is relatively constant in any individual and thus the level of viraemia is a reflection of the rate of virus replication. By about 6 months after seroconversion to HIV, the viral set-point for an individual is established and there is a correlation between HIV RNA levels and long-term prognosis, independent of the CD4 count. Those patients with a viral load consistently >100 000 copies/mL have a 10 times higher risk of progression to AIDS over the ensuing 5 years than those consistently below 10 000 copies/mL. HIV RNA is the standard marker of treatment efficacy (see below). Both duration and magnitude of virus suppression are pointers to clinical outcome. None of the available therapies appears to be able to suppress viral replication indefinitely and a rising viral load, in a patient where compliance is assured, indicates drug failure. Baseline measurements are followed by repeat estimations at intervals of 3–4 months, ideally in conjunction with CD4 counts to allow both pieces of evidence to be used together in decision-making.. KAC p179. |
| 1567 What are the six main classes of antiretrovirals and which are the most commonly used to initiate Rx? | * Nucleoside & nucleotide reverse transcriptase inhibitors * Non-nucleoside reverese transcriptase inhibitors * Integrase inhibitors * Protease inhibitors * CCR5 inhibitors *Fusion inhibitors. Rx should be individually tailored. However usually initiated with three drugs - 2 x NRTI's + 1 x NNRTI (most common in UK with naive pt's) or protease inhibitor. KAC p181-83. |
| 1568 Describe the structure and life cycle of the human Immunodeficiency virus. | See note (HIV Structure and Life Cycle) https://www.goconqr.com/en/notes/5995816/edit |
| 1569 Explain to a patient the importance of adherence to antiretroviral medication and how patients can be supported to achieve it. | Poor adherence can lead to drug resistance. Levels of adherence <95% have been associated with poor virological and immunological responses. KAC p185. Use co-formulations and minimize daily doses to improve adherence. |
| 1570 What are the three common law justifications for breaching confidentiality? | 1 The pt has given consent 2 It's in the pt's best interest but it's impracticable or unreasonable to seek consent 3 It's in the public interest. KAC p6. |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.