6407245
Description
Flashcards by Emma Allde, updated more than 1 year ago
|
|
Created by Emma Allde
about 8 years ago
|
|
| Question | Answer |
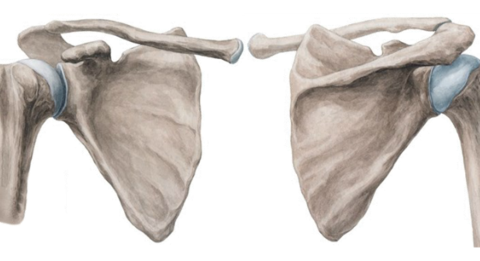
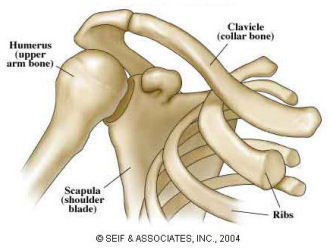
| What (2) bones make up the pectoral or shoulder girdle? | anterior clavicle and posterior scapula (L: key, shoulder) |
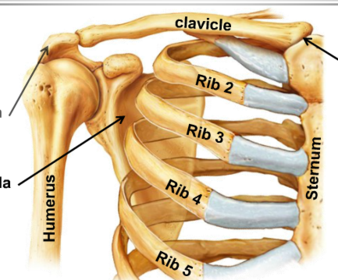
| What separates the shoulder girdles from each other anteriorly? | the sternum |
| What separates the shoulder girdles of either side posteriorly? | Nothing, there is a gap and they do not articulate with e/o or the spinal column |
| What is the only connection b/w the upper limb and axial skeleton? | pectoral/ shoulder girdle |
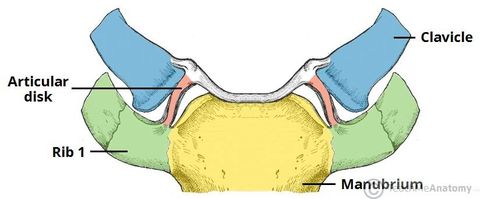
| What does the medial end of the clavicle articulate with? | the manubrium of the sternum |
| What is the joint b/w the clavicle and the sternum? | sternoclavicular joint |
| Posteriorly, the anterior surface of the scapula, along with its associated musculature, forms a connection with what? | the posterior aspects of the upper ribs |
| What is the false joint between the scapula and ribs called? | 'scapulo-thoracic' joint |
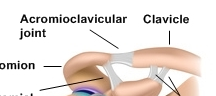
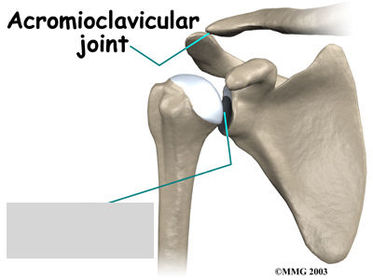
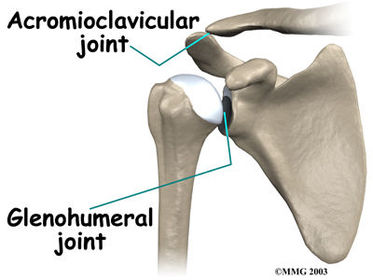
| What is the joint called at the articulation b/w the clavicle and scapula? | acromioclavicular joint |
| What is the function of pectoral girdle? | to brace the upper limb away from the trunk |
| What is the function of the scapula? | give a large surface area for muscular attachments |
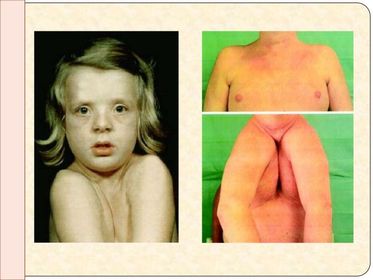
| In what genetic condition are some people born without a clavicle and are thus able to bring the upper limb across the front of the chest? | Cleidocranial dysostosis (or dysplasia) cleido = L. key dystotis = L. bad bone development |
| What is the inheritance pattern of cleidocranial dysotosis? | autosomal dominant |
| What other bone is also affected in cleidocranial dysotosis? | cranium |
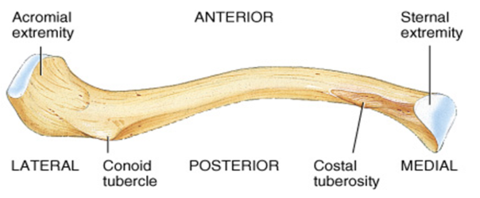
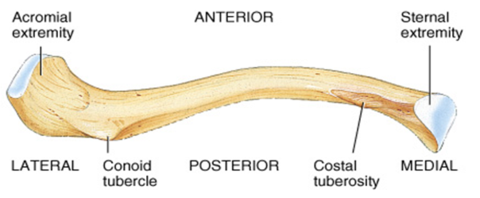
| What is the function of the clavicle? | to act as a brace |
| Describe the articular surface of the medial end of the clavicle: | expanded to form a large, oval facet |
| Describe the articular surface of the lateral end of the clavicle: | flattened in the horizontal plane, with a small posterolateral facet which articulates with the acromion process of the scapula |
| What makes the scapula the most frequently fractured bone in the body? | It serves to transmit forces from the upper limb to the axial skeleton |
| Describe the concave/ convex points of the scapula: | medial 2/3: convex towards the front lateral third: concave towards the front |
| What are (7) unique features of the clavicle: | (1) subcutaneous throughout (2) only horizontal long bone (3) first bone to ossify (4) only long bone to ossify in membrane (5) occasionally pierced by the middle supraclavicular nerve (6) no medullary cavity (7) only long bon to ossify from 2 primary centres |
| How are most clavicular fractures caused? (2) | fall or direct trauma |
| What makes are clavicular fractures potentially dangerous? | The fractured ends present a hazard to the vessels at the root of the neck (thoracic inlet) |
| What kind of bone is the scapula? | flat bone |
| Where, in relation to the ribs, is the scapula found? | 2nd - 7th rib |
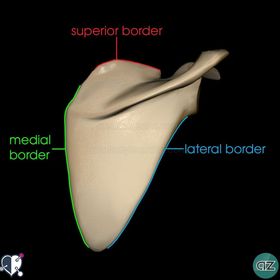
| How many margins does the scapula have? | |
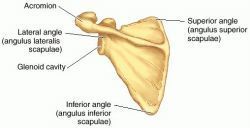
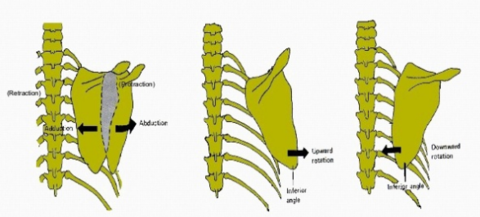
| How many angles does the scapula have? Where are they found? | 3: inferior, superior and lateral |
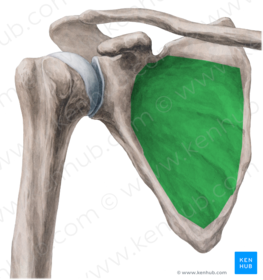
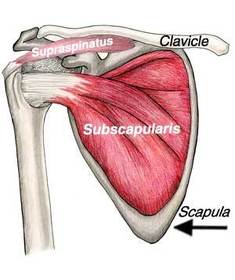
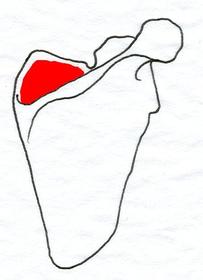
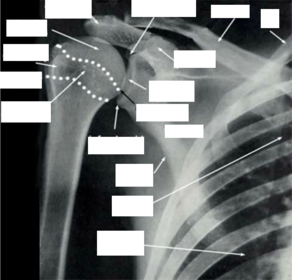
| Identify (anterior view) | subscapular fossa |
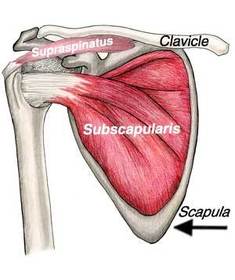
| What do the medial ridges of the anterior surface of the scapula serve as attachments for? | tendinous origins of the subscapularis muscle |
| What attachments does the lateral, anterior surface of the subscapular fossa serve as attachments for? | fibrous attachment of subscapularis muscle |
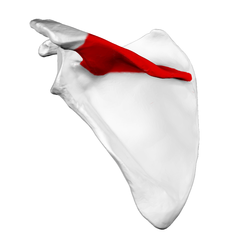
| Identify | supraspinous fossa |
| Identify | infraspinous fossa |
| Identify | spine of the scapula |
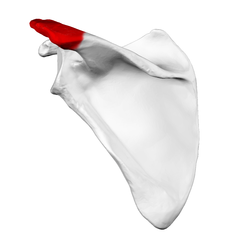
| The spine of the scapula projects shelf-like and posteriorly, angling upwards from the medial border to end in a free lateral process called what? | the acromion |
| What does the acromion articulate with? | the clavicle |
| What does the medial 2/3 of the supraspinous process serve as an attachment for? | supraspinatus msucle |
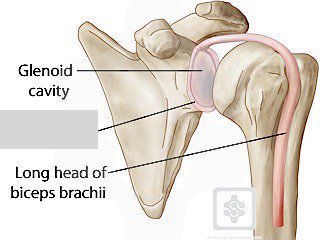
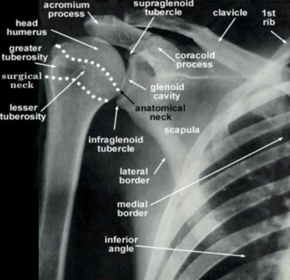
| The supero-lateral angle of the scapula forms a cavity/fossa with what part of what other bone? What is the cavity/fossa called? | head of the humerus glenoid fossa |
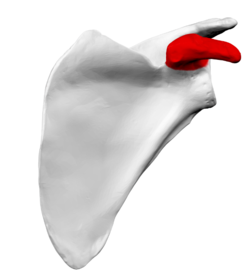
| What process arises from the superior margin of the scapula, projecting antero-laterally over the glenoid fossa? | coracoid process |
| What is found medial to the base of the coracoid process? | suprascapular notch |
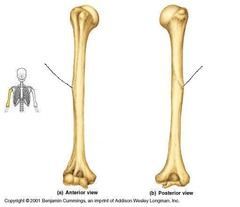
| What does the proximal end form of the humerus form an articular surface with and what is the joint called? | shoulder joint glenohumeral joint |
| What is the articular part of the humerus called? | the head |
| What is unique about this bone? | It has (2) heads: surgical and anatomical |
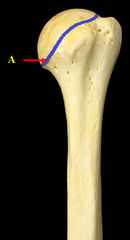
| Label | anatomical neck of the humerus |
| Label | surgical neck of the humerus |
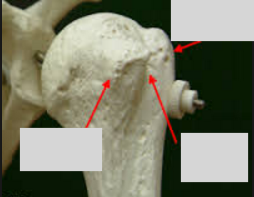
| What (3) features are found b/w the (2) necks of the humerus? | |
| Why is the bicipital (inter-tubercular) groove called as such? | b/c the long head of the biceps brachii sits in the groove, having just passed over the head and anatomical neck |
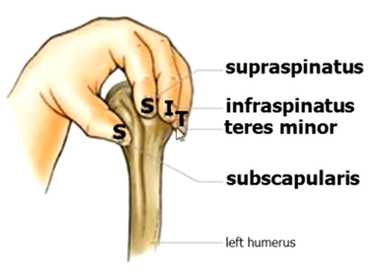
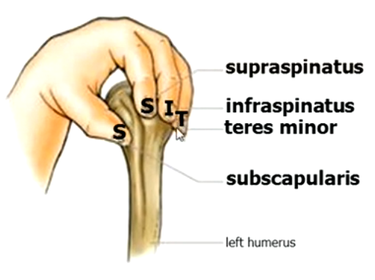
| How many facets does the greater tuberosity have? What are the muscle attachments? | 3 for the attachment of three separates muscles from the scapula supraspinatus, infraspinatus and teres minor |
| How many facets does the the lesser the tuberosity have? Where do the muscle attachments originate? | 1, from the scapular muscle (subscapularis) |
| Identify What is the muscle attachment? | Deltoid tuberosity tendon of the deltoid muscle |
| Identify What structures are found here? | Spiral groove Nerve (radial) and artery (profunda brachii) |
| Identify this joint and describe its movement | Sternoclavicular joint b/w the clavicle and sternum, the only shoulder to articulate with the axial skeleton very mobile, allowing movement of the shoulder |
| Identify this joint and describe its movement | Acromioclavicular joint b/w the clavicle and scapula Less mobile, only permits small gliding and rotation movements |
| Identify this "joint" and describe its movement | Scapulo-thoracic joint b/w the scapula and the rib-cage Movements here allow the upper limb to be moved around the trunk, and increase our range of hand positioning in space |
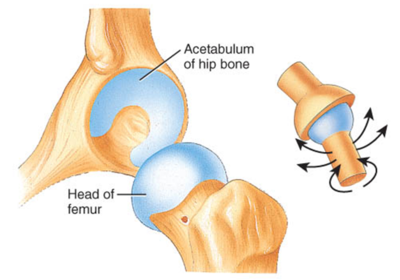
| Identify this joint and describe its movement | b/w the head of the humerus and glenoid cavity of scapula allows most movement of the shoulder |
| What kind of joint is the sternoclavicular joint? | synovial joint |
| What divides the sternoclavicular joint in two? | an articular disc |
| What are the (2) main components of the sternoclavicular joint? | the concave indention of the sternum and the sternal end of the clavicle |
| How is the incongruity of the sternoclavicular joint (specifically the articular facets) adjusted | a cartilage-like fibrous tissue |
| Describe the capsule found at the sternoclavicular joint | slack and thick |
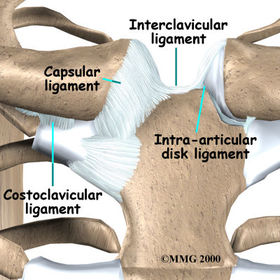
| What helps strengthen the sternoclavicular capsule? | anterior and posterior sternoclavicular ligaments |
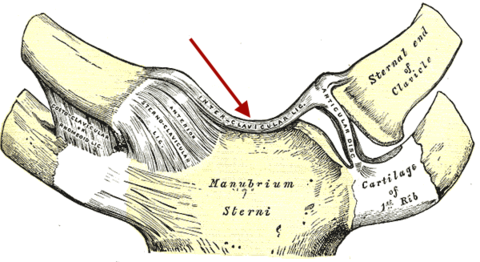
| Identify and define its purpose | The interclavicular ligament Connects the R. and L. clavicles |
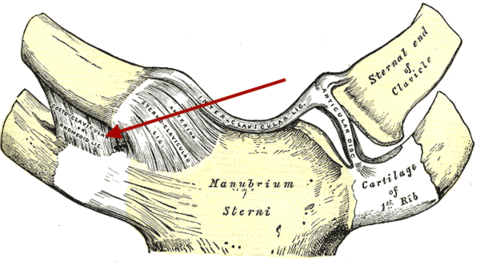
| Identify and define its purpose | Sternoclavicular ligament helps strengthen the sternoclavicular capsule Extends b/w the 1st rib and clavicle |
| What kind of joint is the sternoclavicular joint? | ball and socket joint |
| How many degrees of freedom does the sternoclavicular joint have? | 3 |
| The sternoclavicular joint is capable of movements in superior-inferior (up and down) plane up to __° and in the anterior-posterior (front and back) plane up to __° | 60, 20 |
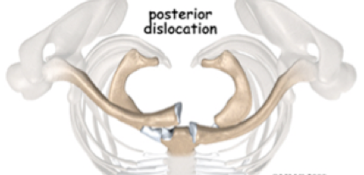
| What is the danger of posterior sternoclavicular dislocations? | Whilst rare, the clavicle may compress of lacerate a lung, a great vessels, the trachea or oesophagus |
| What is the most common cause of posterior sternoclavicular dislocations? | MVA, sports or a fall, with a force to the shoulder usually via an externally, laterally placed blow along the axis of the clavicle |
| In which direction does the clavicle move is a posterior dislocation? | anteriorly/ superiorly due to the attachment of its ligament |
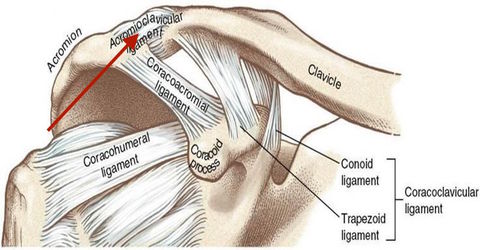
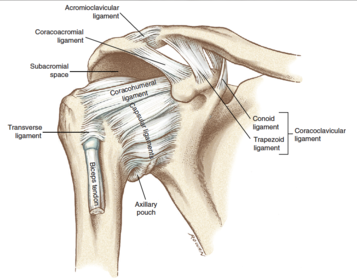
| Define ligament and define its purpose | Acromioclavicular ligament helps strengthen the capsule at the acriomioclavicular joint (ACJ) |
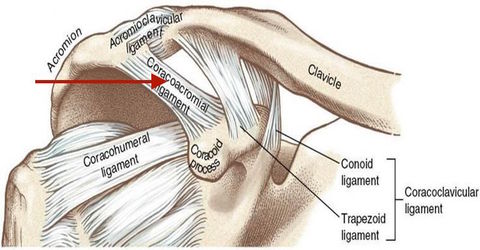
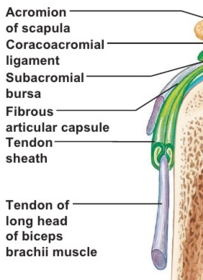
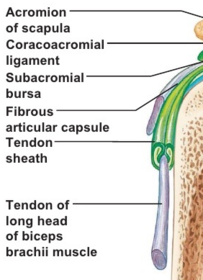
| Define ligament and label | Coracoacromial ligament along with the tendon of the long head of biceps protects the top of the joint |
| How can the coracoacromial ligament be divided further? | Antero-lateral: trapezoid ligament Postero-medial: conoid ligament |
| Is there a disc at the acromioclavicular joint? | Yes, but it can be absent as the capsule here is very lax but small |
| What kind of joint is the acromioclavicular joint? | synovial gliding joint |
| What kind of joint is the glenohumeral joint? | Ball-and-socket |
| As the shoulder (glenohumeral) joint lacks strong ligaments, how is action maintained? | by enveloping muscle making it a "muscle-dependent" joint |
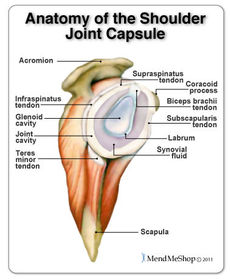
| How is the synovial membrane of the capsule of the glenohumeral joint attached? | via the glenoid lip |
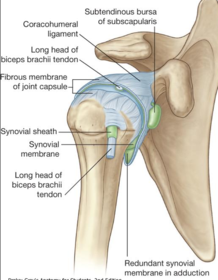
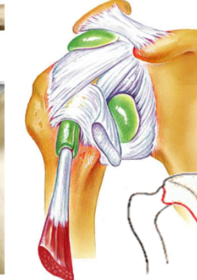
| What structure evaginates and surrounds the synovial membrane of the glenohumeral joint like a tubular sheath? | The long head of biceps brachii tendon |
| Identify this structure When it it found? | axillary recess when the articular capsule is slack and when the arm hangs down |
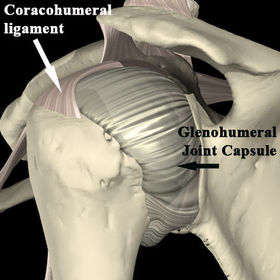
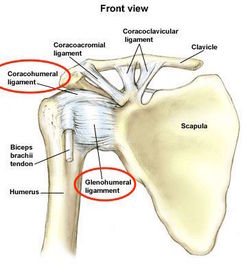
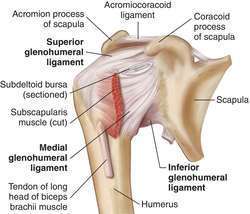
| What (4) structures support the upper part of the glenohumeral capsule? | mainly the coracohumeral ligament also (3) weak glenohumeral ligaments |
| Define and know the importance of this structure | glenoid labrum it serves to the deepen the glenohumeral socket |
| What are synovial bursae and where are they found in the shoulder? | a fluid-filled sac or sac-like cavity, especially one countering friction at a joint acromial process (subacromial bursae), deltoid and subscapular bursae |
| Which is the only bursae in direct communication with the joint cavity? | subscapular bursae |
| What does the capsule of the glenohumeral joint attach to? | proximally to the glenoid labrum and laterally to the anatomical neck of the humerus |
| Why does the capsule at the glenohumeral joint need to be week? esp. when? | to permit free movement esp. at the inferior aspect of the joint where the capsule is tightened upon full abduction of the joint |
| What structure(s) thicken the superior and anterior parts of the capsule? | the glenohumeral ligaments |
| There is a gap b/w the glenohumeral ligaments anteriorly, where the synovium membrane is able to escape from the confines of the capsule to form what? | the subscapularis bursa |
| What tendon arises from inside the joint (from the supragenoid tubercle), making it intra-capsular? | the long head of biceps brachii |
| Is the long head of biceps brachii intra-synovial too? | No, it sites outside the synovial lining of the joint, making it extra-synovial |
| What is the long head of biceps brachii surrounded by to help protect it as the joint moves? | a sheath of synovium |
| What structure emerges from the synovial sheath into the biciptial groove, outside the joint, making it exposed and prone to inflammation (teno-synovitis)? | the synovial sheath |
| What structures provide vertical stability to the humeral head? | the glenohumeral capsule and the coracohumeral ligament |
| What structures provide anterior stability to the humeral head? | the anterior capsulo-ligamentous complex (but the contribution is limited) |
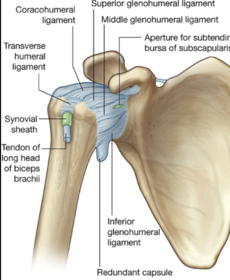
| What ligaments are simply thickenings of the capsule? | the superior, middle and inferior glenohumeral ligaments |
| What kind of structure is found b/w the superior and middle glenohumeral ligaments? | a foramen |
| What does the small foramen b/w the superior and middle glenohumeral ligaments allow? | a bursa to protrude anteriorly |
| What does the bursa b/w the superior and middle glenohumeral ligaments allow? | movements if the tendon is in front of the joint (subscapularis tendon) |
| Which of the glenohumeral ligaments is the largest and strongest of the three? | the inferior glenohumeral ligament |
| Where is the inferior glenohumeral ligament found? What function does it provide? | b/w the subscapularis and teres minor tendons it reinforces the inferior glenohumeral capsule |
| What is the significance of the inferior glenohumeral ligament? | beyond 90 degrees abduction, the subcapularis tendon no longer provides anterior (forward) stability of the humeral head, so the anterior stability must be provided by the axillary pouch of the inferior glenohumeral ligament |
| Define and label | transverse humeral ligament passes b/w the humeral tubercles, attaching superior to the epiphyseal line It converts the intertubercular groove into a canal into a canal and acts as a retinaculum for the long tendon of the biceps |
| Where is the glenohumeral joint weakest? | inferiorly |
| Which scan is the test of choice for diagnosing soft tissue injuries and is often used for assessing ongoing pain which fails to respond to traditional treatment options such as rest, physiotherapy and medication | MRI |
| What imaging types are excellent for detecting bone injuries? | x-ray and CT |
| What imaging is best for diagnosing soft tissue injuries such as tears of the rotators cuff or inflammation? | MRI |
| What kind of abnormality is shown? | y view anterior shoulder dislocation |
| What kind of abnormality is shown? | y view posterior shoulder dislocation |
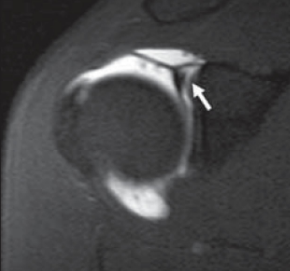
| What kind of abnormality is shown? | Glenoid labrum tear |
| What kind of abnormality is shown? | SLAP lesion Superior labrum from anterior to posterior lesion/ tear |
| Label and define | A Bankart lesion Injury of the anterior (inferior) glenoid labrum of the shoulder due to anterior shoulder dislocation. When this happens, a pocket at the front of the glenoid forms that allows the humeral head to dislocate into it. |
| Shoulder dislocations are brought on by a force applied when the limb is in a position of _______ and _______ rotation, e.g. trying to protect yourself in a fall from a weight when your hands are in front of your head. | abduction, external |
| The shoulder joint is weakest ______, and hence is more easily diplaced in this direction | inferiorly |
| The most common form of dislocation is called ______, and the limb is placed ____-______ | anterior, antero-inferiorly |
| Anterior dislocations stresses the _____ capsule, and the _____ part of the glenoid labrum. If the glenoid labrum is torn, it is referred to as a _______ _____. | anterior, anterior, Bankart lesion |
| Shoulder joint deformity, an abnormally long arm, humeral head position in the axilla and pain and dysfunction are symptoms of what? | a shoulder dislocation |
| What is the most physically obvious sign of shoulder dislocation? | The normal rounded contour of the shoulder is lost the greater tubercle is usually the most palpable |
| What structures become palpable in a shoulder dislocation? | the acromion |
| Movements of the dislocated shoulder are limited and painful, and hence the limb remains in a partially ____ and ____ rotated position This is because the ____ rotators of the joint (________,______) are stretched and also maintained in this position | abducted, laterally lateral (infraspinatous and teres minor) |
| Most posterior dislocations are caused by what? | a direct blow to the front of shoulder, or the violent twisting of the upper arm twisting (e.g. via direct trauma or an epileptic attack) |
| A shoulder can be partially dislocated (in the head of the upper arm is partially out of the shoulder socket) or completely dislocated (the head of the upper arm is completely out of the socket. A partial dislocation is know as: | subluxation |
| a dislocation can result in fracture of the ______ | humerus NB: nerve damage, damage to an artery or muscle is also possible |
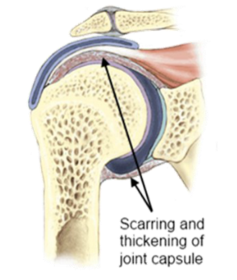
| What term is used to describe a loss of range of motion in the shoulder? | Frozen shoulder or "Adhesive Capsulitis" |
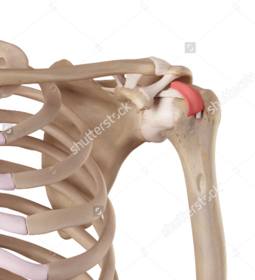
| What are the characteristics of a frozen shoulder? | inflammation, associated pain, limited movement of the glenohumeral joint |
| Frozen shoulder is most common in what age range? | 40-60 |
| How many people in the UK are affected by frozen shoulder annually? | 1 million |
| What is the ratio of frozen shoulder female:male? | 2:I for unknown reasons |
| What are the four main types of shoulder stiffness? What is the most common of the four? | Idiopathic, Diabetic, Post-traumatic and Post--surgical Idiopathic is the most common |
| What is the leading hypothesis as to why people with endocrine problems such as diabetics are more prone to shoulder stiffness? | It is not entirely understood, but the main hypothesis suggests that it is linked to increased vascularity of the capsule |
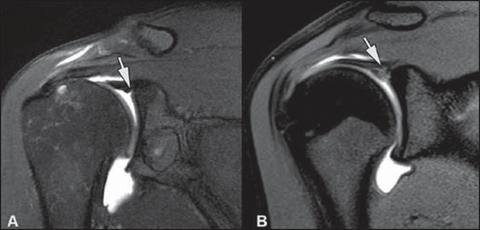
| What is shown in the image and how does it relate to stiff shoulder? | Synovitis Typically seen in stiff or frozen shoulder. Can be accompanied with scarring and adhesions that limit motion. Possible both inside and outside the joint. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.