7232391
Description
Flashcards by Andrew Street, updated more than 1 year ago
|
|
Created by Andrew Street
over 8 years ago
|
|
| Question | Answer |
| Give a DDx fo RUQ P. | * Acute cholecystitis * Duodenal ulcer * Hepatitis * Congestive hepatomegaly * Pyelonephritis Appendicitis * Pneumonia OHOCM p609. |
| Bile contains c......, b..... p..... (from broken down Hb), and p..... If the concentrations vary, different stones may form. | Bile contains *cholesterol, bile pigments* (from broken down Hb), and *phospholipids* If the concentrations vary, different stones may form. OHOCM p636. |
| What are the different types of stones that may form and some risk factors? | * Pigment stones: (<10%) Small, friable & irregular. Causes: haemolysis. * Cholesterol stones: Large, often solitary. Causes: ♀, age, obesity (Admirand’s triangle: ↑risk of stone if ↓lecithin, ↓bile salts, ↑cholesterol). * Mixed stones: Faceted (calcium salts, pigment, & cholesterol). OHOCM p636. |
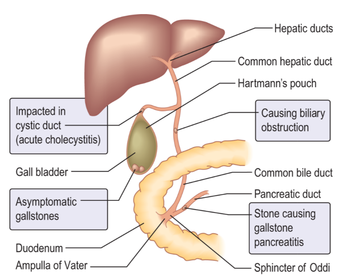
| Describe the anatomical positions required for stones to cause acute cholecystitis, biliary obstruction, gallstone pancreatitis, and asymptomatic gallstones. | |
| What are some complications of gallstones? | In the gallbladder & cystic duct: • Biliary colic • Acute and chronic cholecystitis • Mucocoele • Empyema • Carcinoma • Mirizzi’s syndrome (stone in the GB presses on the bile duct causing jaundice) In the bile ducts: • Obstructive jaundice • Cholangitis • Pancreatitis In the gut: • Gallstone ileus OHOCM p637. |
| What is biliary colic? | Symptomatic gallstones temporarily obstructing the cystic duct or common bile duct. K & C p352. |
| S & Sx of biliary colic. | * P may be severe but constant with a 'crescendo' characteristic * P may be epigastric, RUQ +/- radiation to R shoulder * Sx often follow heavy meal * N & V frequent K & C p352. |
| What is acute cholecystitis and what complications may it cause? | * Obstruction to gall bladder emptying (95% of cases due to a gall bladder stone) * Leads to progressive distension - may compromise vascular supply * Also an inflammatory response secondary to retained bile (unlike biliary colic) * Infxn may follow * Rarely it can become distended by pus (empyema), become gangrenous, & perforate leading to peritonitis K & C p352. |
| S & Sx of acute cholecystitis. | * Initial features similar to biliary colic * Over hours progresses to severe RUQ P due to inflammation irritating the peritoneum * Muscle guarding & rigidity * Murphy's sign +ve * RUQ mass may be palpable (phlegmon - inflamed adherent bowel & omentum) K & C p352 & OHOCM p636. |
| Describe the Ix used to confirm a Dx of gallstones. | * BD's - often show ^WCC & inflammatory markers (eg CRP), ^serum bilirubin * LFT's - ^ALP, ^GGT * USS - most useful Ix * If Dx uncertain after USS HIDA cholescintigraphy * MRCP may be used for stones in CBD * Ix for exclusion of DDx - CXR, urinalysis, ECG OHOCM p636. |
| Rx & Mx of acute cholecystitis. | Initially conservative: * NBM * IVI * ABx according to local protocol After initial Rx laproscopic cholecystectomy - used to be after 6-12/52 now being done early to avoid complications. If GB perforation then open Sx. OHOCM p636 & 637. |
| What is ERC/P? | Endoscopic retrograde cholangiography/pancreatography. Usually used to visualise & remove stones seen via other Ix's from the CBD. |
| What is cholangitis, what are the S & Sx, & Rx? | Infxn of the bile duct. S & Sx: * RUQ P * Jaundice * Rigors (Charcot's triad) Rx with ABx - eg cefuroxime 1.5g/8h IV & metronidazole 500mg/8h IV/PR OHOCM p636. |
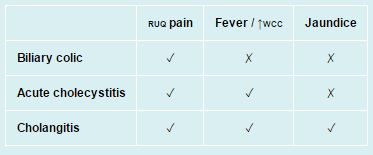
| Compare & contrast the S & Sx of RUQ P, fever/^WCC, & jaundice in biliary colic, acute cholecystitis, & cholangitis. |
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.