16629351
Tuberculosis
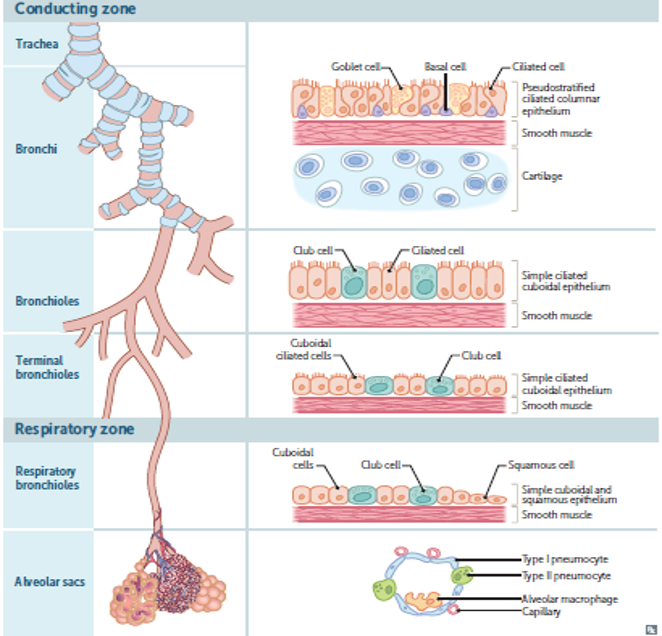
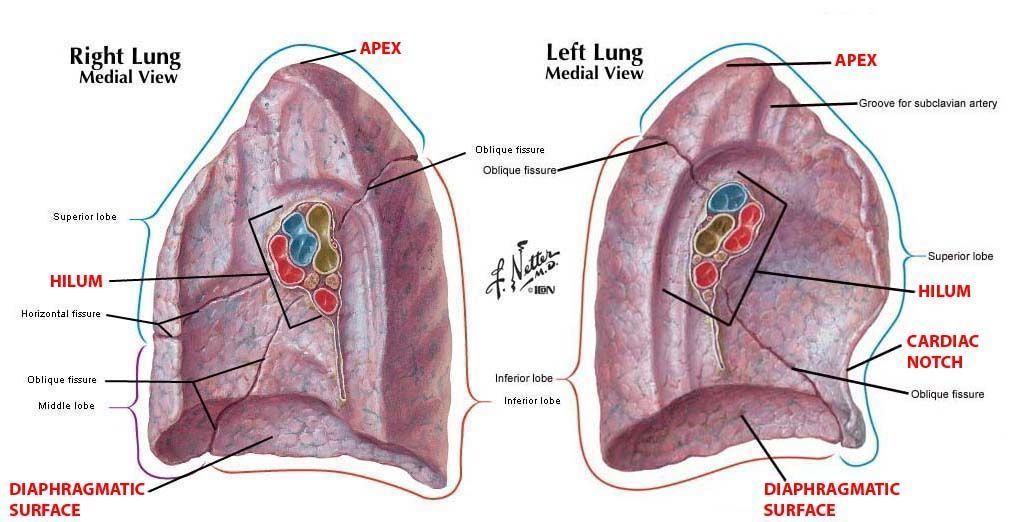
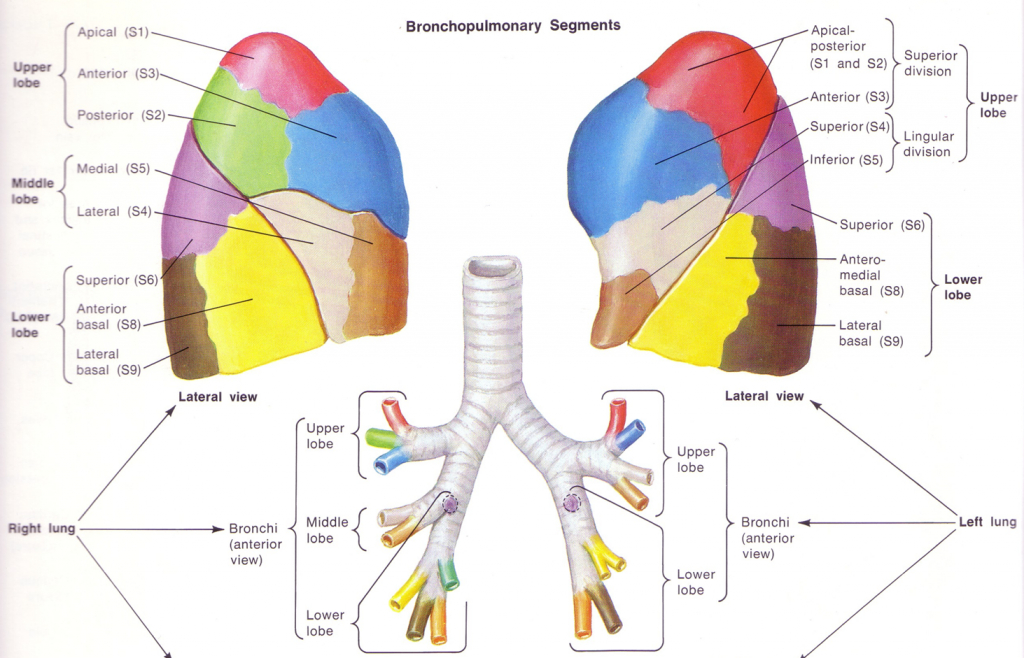
- Anatomy
of the
lungs
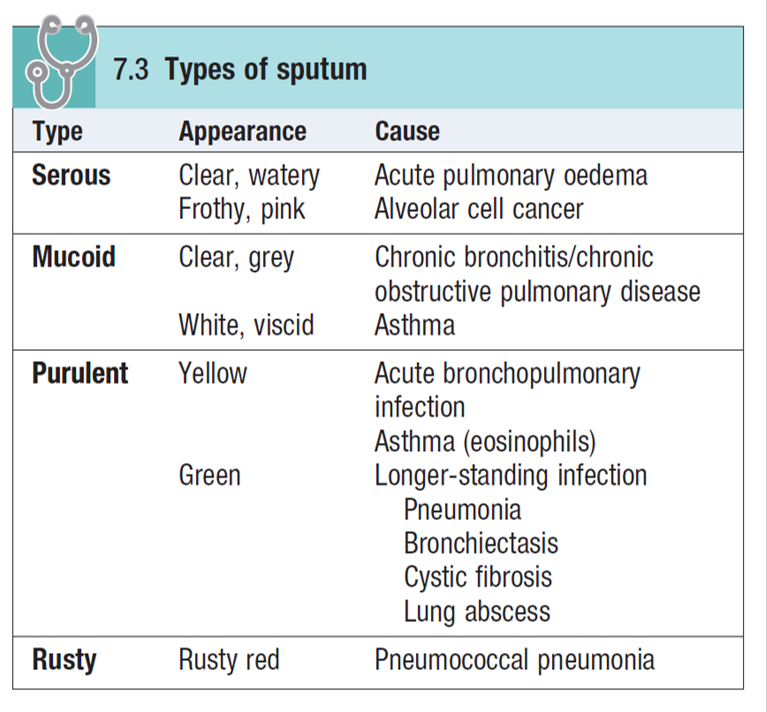
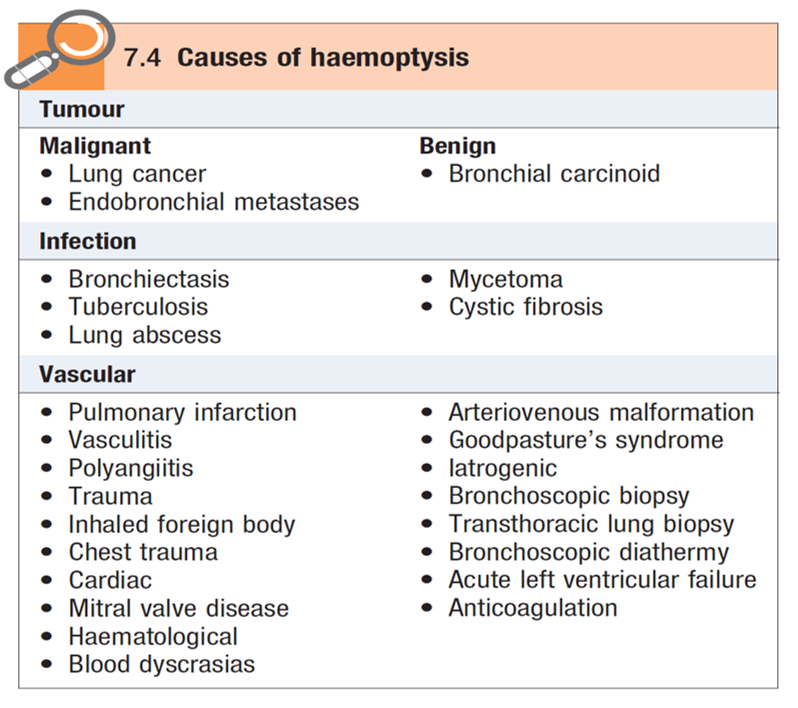
- Causes of Productive Cough
- Based on sputum color
- Based on sputum color
- Lower
Respiratory Tract
Infections
- Acute bronchitis
- adenovirus, coronavirus,
parainfluenza, influenza and
rhinovirus
- Only few cases are caused by bacterial infection
- Only few cases are caused by bacterial infection
- is self-limiting infection
- It manifests as cough that sometimes could come with sputum, wheezing, fever and shortness of
breath
- adenovirus, coronavirus,
parainfluenza, influenza and
rhinovirus
- Bronchiolitis
- self-limiting infection
- Respiratory syncytial virus
- Usually it infects children
- It manifests as cough, fever, runny nose, wheezing and crackles.
- self-limiting infection
- Influenza
- RNA virus
- 3 types
- Type A
- is the most common type of influenza virus
- infect both humans and animals
- is the most common type of influenza virus
- Type B
- infect humans only
- infect humans only
- Type C
- infect both human and pigs.
- infect both human and pigs.
- Type A
- Symptoms of influenza infection start 1 to 4
days after infection and it include fever,
headache, runny nose, sore throat, myalgia,
malaise and nonproductive cough.
- RNA virus
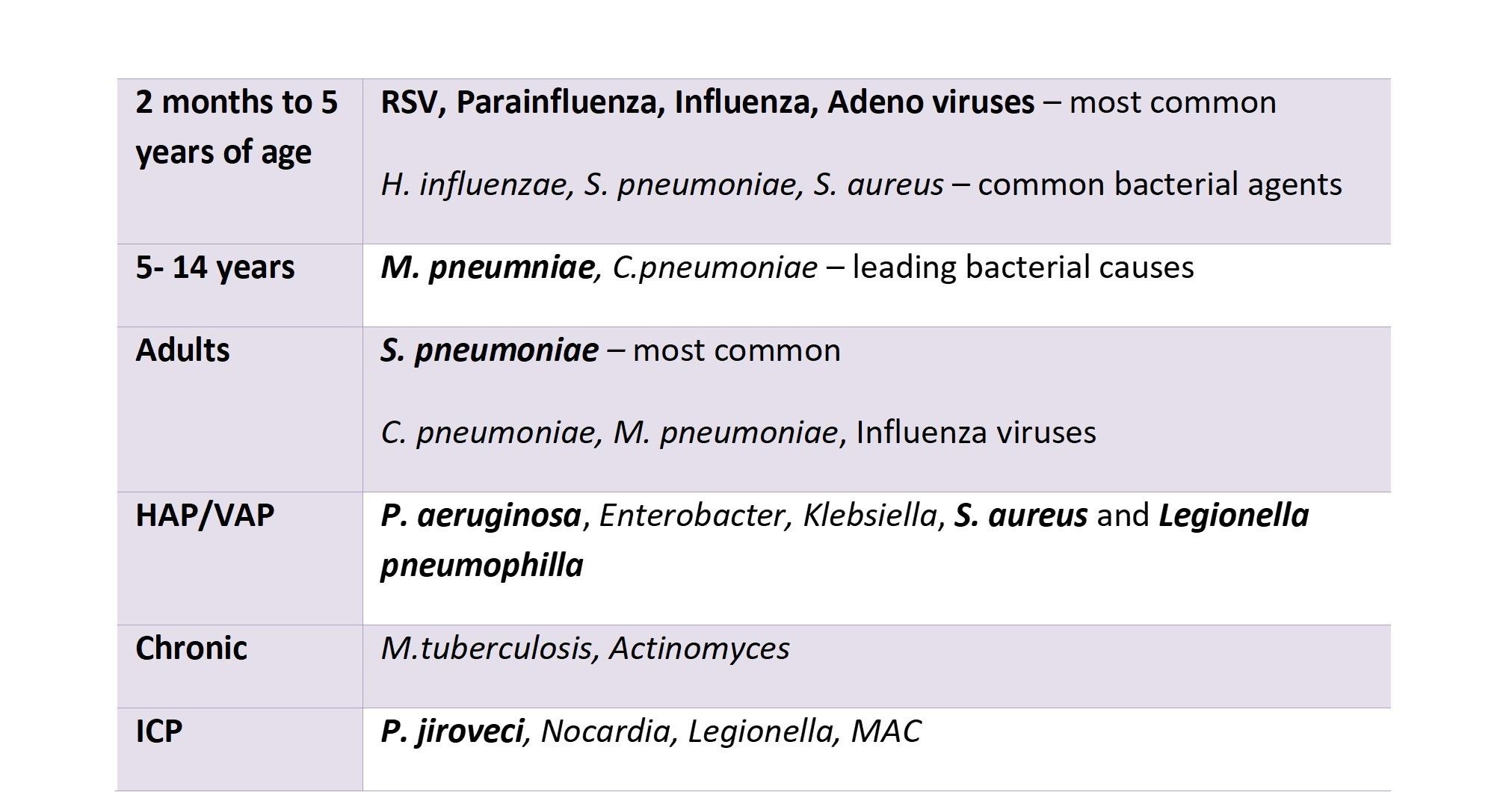
- Pneumonia
- Pneumonia manifests as dyspnea or
shortness of breath, chest pain, productive
cough ( bloody sputum or yellow green
sputum), fatigue, fever, tachypnea, decreased
breath sound and dullness to percussion.
- Caustive Agents
- Pneumonia manifests as dyspnea or
shortness of breath, chest pain, productive
cough ( bloody sputum or yellow green
sputum), fatigue, fever, tachypnea, decreased
breath sound and dullness to percussion.
- Acute bronchitis
- Classification of myobacterium
- Non- cultivable
- M,leprea
- M,leprea
- Typical
- M. tuberculosis
- M, bovis
- M. africanum
- M. tuberculosis
- Atypical
- Runyon
Group I
(Photochromogens)
- M. kansasii
- M. marinum
- M. kansasii
- Runyon
Group II
(Scotochromogens)
- M. szulgai
- M. xenopi
- M. scrofulaceum
- M. szulgai
- Runyon
Group III
(Nonchromogens)
- M. avium
- M. haemophilum
- M. ulcerans
- M. avium
- Runyon Group
IV (Rapid
Growers)
- M. abscessus
- M. chelonae
- M. fortuitum
- M. abscessus
- Runyon
Group I
(Photochromogens)
- Non- cultivable
- Epidemiology of TB
- infects 1/3 world
population – 2
billion people
- 95% cases are
in developing
world
- 8 million
new
cases/yr
- 3 million deaths/yr
- 3 million deaths/yr
- 80% of all TB cases
occurs in Sub
Sharan Africa and
South East Asia
- Globally, TB incidence is
falling at about 2% per
year. This needs to
accelerate to a 4–5%
annual decline to reach
the 2020 milestones of
the End TB Strategy.
- An estimated 54 million
lives were saved through TB
diagnosis and treatment
between 2000 and 2017.
- infects 1/3 world
population – 2
billion people
- Transmission
- Touch
- Ingestion
- Airborne
- Touch
- Risk factors
- Recently
infected with TB
- Those with medical
conditions that weaken
the immune system
- HIV infection (the virus that causes
AIDS)\ Substance abuse\ Silicosis\
Diabetes mellitus\ Severe kidney
disease\ Low body weight\ Organ
transplants\ Head and neck
cancer\ Medical treatments such as
corticosteroids or organ transplant\
Specialized treatment for
rheumatoid arthritis or Crohn’s
disease
- HIV infection (the virus that causes
AIDS)\ Substance abuse\ Silicosis\
Diabetes mellitus\ Severe kidney
disease\ Low body weight\ Organ
transplants\ Head and neck
cancer\ Medical treatments such as
corticosteroids or organ transplant\
Specialized treatment for
rheumatoid arthritis or Crohn’s
disease
- Recently
infected with TB
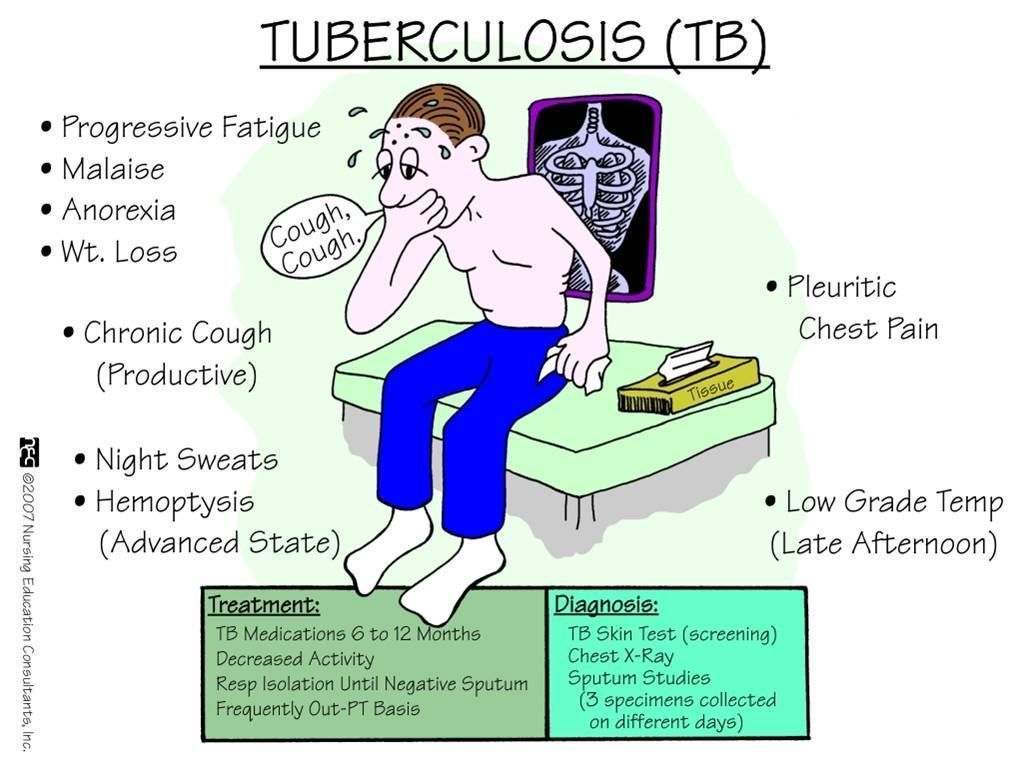
- Signs and symptoms
- Mechanism of Fever
- Pyrogen
- Macrophages and immune cells are activated
- IL-1, IL-6, IL-8, TNF-a, interferon gamma
- Laminae terminalis
- Pre-optic region
- Posterior hypothalamic region
- Activate phospholipase
- Induce the production of prostaglandins E2
- Prostaglandins E2 will change the
temperature set point
- Body will try to increase body Tempreture by
- Peripheral vasoconstriction
- Norepinephirne
increases
thermogenesis in
adipose tissue
- Shivering
- Peripheral vasoconstriction
- Body will try to increase body Tempreture by
- Prostaglandins E2 will change the
temperature set point
- Induce the production of prostaglandins E2
- Activate phospholipase
- Posterior hypothalamic region
- Pre-optic region
- Laminae terminalis
- IL-1, IL-6, IL-8, TNF-a, interferon gamma
- Macrophages and immune cells are activated
- Pyrogen
- Investigations of Tuberculosis
- collection of a specimen
- Early morning sputum in case of pulmonary TB and it
requires a minimum of two successive days sputum\
Bronchoalveolar lavage (BAL) \Gastric aspirate\ CSF \ Lymph
node biopsy or aspirates\ Other tissue biopsies
- Early morning sputum in case of pulmonary TB and it
requires a minimum of two successive days sputum\
Bronchoalveolar lavage (BAL) \Gastric aspirate\ CSF \ Lymph
node biopsy or aspirates\ Other tissue biopsies
- Microscopy
- Ziehl Neelsen Staining /
Acid Fast Staining
- Specificity of 98% / Low sensitivity < 50%
/Qualitative and quantitative
- Specificity of 98% / Low sensitivity < 50%
/Qualitative and quantitative
- Fluorescent staining
(Auramine-Rhodamine
Fluorochrome)
- Rapid and more sensitive / Expensive / Dye toxicity.
- Rapid and more sensitive / Expensive / Dye toxicity.
- Ziehl Neelsen Staining /
Acid Fast Staining
- Culture (The Gold Standard)
- Solid Media
- Agar based (Middlebrook 7H10) / Egg based
(Löwenstein-Jensen medium)
- Culture is incubated at 35 C, 5-10% CO2 and in
high humidity
- It takes 4-8 weeks / can be
reported negative after 8 weeks.
- Rough, tough and buff colonies.
- Agar based (Middlebrook 7H10) / Egg based
(Löwenstein-Jensen medium)
- Liquid Media
- BACTEC 460 /
Mycobacteria Growth
Indicator Tube (MGIT)
- Positive in 2-3 weeks
/ can be reported
negative after 6
weeks
- BACTEC 460 /
Mycobacteria Growth
Indicator Tube (MGIT)
- Radiometric
culture has faster
results (3-4 days)
- Solid Media
- Molecular Methods
- PCR
- Molecular Line
Probe Assays
(LPA)
- It is a DNA-based
diagnostic test that
identifies
multidrug-resistant
TB (MDR TB).
- It is a DNA-based
diagnostic test that
identifies
multidrug-resistant
TB (MDR TB).
- Xpert
MTB/RIF
Assays
- A new NAAT that quickly
identifies possible
multidrug-resistant TB (MDR
TB) (Rifampicin resistance).
- A new NAAT that quickly
identifies possible
multidrug-resistant TB (MDR
TB) (Rifampicin resistance).
- PCR
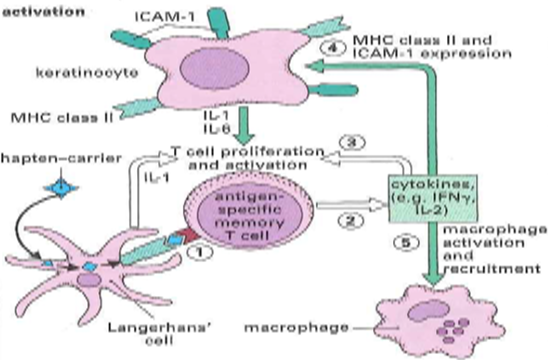
- Tuberculin Test
(Mantoux tuberculin
skin test (TST))
- Delayed
hypersensitivity
reaction type 4.
- Injecting tuberculin
intradermally, which contains
purified protein derivative from
mycobacteria tuberculosis (PPD
tuberculin).
- Induration
measured after
48-72 hours.
- It can be positive in case of active
TB (disease), people with latent
infections, and people who had
received BCG vaccination.
- Delayed
hypersensitivity
reaction type 4.
- Serology
- Interferon-Gamma
Release Assays
(IGRAs)
- Test that detects
IFN-g that is
released by WBC
when mixed with
antigens derived
from M.
tuberculosis.
- The results within 24 hours.
- BCG vaccination does not cause a false positive IGRA test result.
- Test that detects
IFN-g that is
released by WBC
when mixed with
antigens derived
from M.
tuberculosis.
- Interferon-Gamma
Release Assays
(IGRAs)
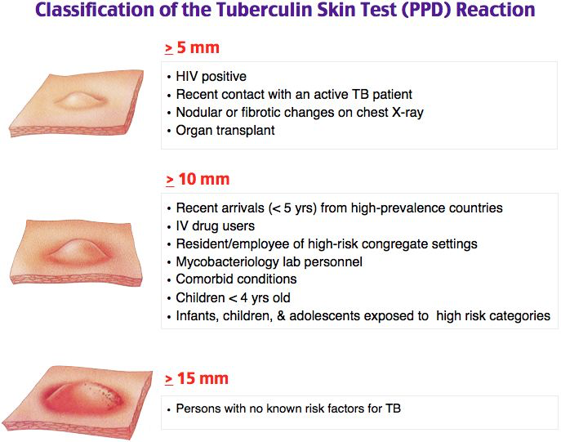
- Investigations of TB Contacts
- Contacts with skin test reaction of an induration
diameter of >5 mm or with any symptoms of TB
disease should go for further examination and TB
diagnostic tests, starting with a chest radiograph.
- Contacts with special vulnerability or susceptibility to TB disease
should undergo for further examination and diagnostic testing
regardless of whether they have a positive skin test result or are ill.
- Contacts with skin test reaction of an induration
diameter of >5 mm or with any symptoms of TB
disease should go for further examination and TB
diagnostic tests, starting with a chest radiograph.
- Evaluating
Response to
Treatment
- Clinical evaluation
- (Monthly / Adverse
reactions to
medications and to
assess adherence)
- (Monthly / Adverse
reactions to
medications and to
assess adherence)
- Bacteriological examination
- Positive cultures after 3 months
of treatment: Reevaluated for
drug-resistant disease and
failure to adhere to the regimen
- Positive cultures
after 4 months of
therapy: Failure of
the treatment and
managed
accordingly
- Positive cultures after 3 months
of treatment: Reevaluated for
drug-resistant disease and
failure to adhere to the regimen
- Chest radiograph
- Positive cultures at the
diagnosis: Repeat chest
radiograph after completing 2
months of therapy might be
useful (not essential), while
chest radiograph after
completing the course of the
therapy gives a baseline for
comparison with any future
films.
- Negative culture in the initial
diagnosis: Chest radiograph is
necessary after 2 months of
treatment, and desirable at
completion of treatment.
- Positive cultures at the
diagnosis: Repeat chest
radiograph after completing 2
months of therapy might be
useful (not essential), while
chest radiograph after
completing the course of the
therapy gives a baseline for
comparison with any future
films.
- Clinical evaluation
- collection of a specimen
- Tuberculosis
(TB) Treatment &
Management
- Approach
Considerations
- Isolate patients with
possible (TB) in a private
room with negative
pressure\ Medical staff must
wear high-efficiency
disposable masks\ Continue
isolation until sputum
smears are negative for 3
consecutive determinations
- Isolate patients with
possible (TB) in a private
room with negative
pressure\ Medical staff must
wear high-efficiency
disposable masks\ Continue
isolation until sputum
smears are negative for 3
consecutive determinations
- Drug therapy
- Patients who are receiving
pyrazinamide should undergo
baseline and periodic serum uric
acid assessments, and those who
are receiving long-term
ethambutol should undergo
baseline and periodic visual acuity
and red-green color perception
testing (Ishihara test) for color
blindness.
- After 2 months of therapy (for a fully
susceptible isolate), pyrazinamide
can be stopped. Isoniazid plus
rifampin are continued as daily or
intermittent therapy for 4 more
months. If isolated isoniazid
resistance is documented,
discontinue isoniazid and continue
treatment with rifampin,
pyrazinamide, and ethambutol for
the entire 6 months. Therapy must
be extended if the patient has
cavitary disease and remains
culture-positive after 2 months of
treatment.
- After 2 months of therapy (for a fully
susceptible isolate), pyrazinamide
can be stopped. Isoniazid plus
rifampin are continued as daily or
intermittent therapy for 4 more
months. If isolated isoniazid
resistance is documented,
discontinue isoniazid and continue
treatment with rifampin,
pyrazinamide, and ethambutol for
the entire 6 months. Therapy must
be extended if the patient has
cavitary disease and remains
culture-positive after 2 months of
treatment.
- Approach
Considerations
- Disease notification
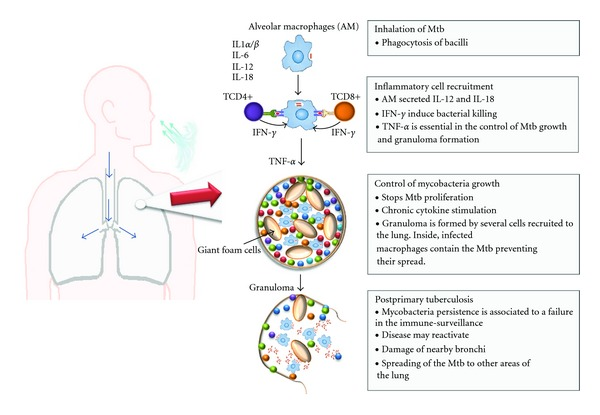
- Pathogenesis
- Primary tuberculosis
- granuloma - macrophages,
fibroblasts, lymphocytes, and
neutrophils
- tubercles can become calcified – Ghon
complex
- self-limiting
- Infants & very young have
a high mortality from
primary infections
- granuloma - macrophages,
fibroblasts, lymphocytes, and
neutrophils
- Secondary
Tuberculosis
- Tubercles can reactivate,
proliferate, and cause
additional infection and
damage in the lung
- Re-infection from
exogenous bacteria
- Reactivated disease
occurs in areas with high
oxygen tension and low
lymphatic drainage such
as the apices of the lungs
- Tubercles can reactivate,
proliferate, and cause
additional infection and
damage in the lung
- Disseminated
tuberculosis
- bacilli can disseminate
to the lymph nodes,
kidneys, bones, genital
tract, brain, etc
- prognosis is
poor and the
affected site
suffers severe
damage:
- renal necrosis and
scarring damage to
reproductive organs
degeneration of spine
meningitis
- renal necrosis and
scarring damage to
reproductive organs
degeneration of spine
meningitis
- bacilli can disseminate
to the lymph nodes,
kidneys, bones, genital
tract, brain, etc
- Latent TB
- Is a subclinical infection
with tubercle bacilli
without clinical,
bacteriological or
radiological signs of the
disease
- Is a subclinical infection
with tubercle bacilli
without clinical,
bacteriological or
radiological signs of the
disease
- Monitoring
- Patients diagnosed with active TB
should undergo sputum analysis
for Mycobacterium
tuberculosis weekly until sputum
conversion is documented.
Monitoring for toxicity includes
baseline and periodic liver enzymes,
complete blood cell (CBC) count,
and serum creatinine.
- Patients diagnosed with active TB
should undergo sputum analysis
for Mycobacterium
tuberculosis weekly until sputum
conversion is documented.
Monitoring for toxicity includes
baseline and periodic liver enzymes,
complete blood cell (CBC) count,
and serum creatinine.
- BCG vaccine
- contains a live but
very weakened form
of a bacteria
called Mycobacterium
bovis
- prevention of severe
forms of TB
(tuberculous meningitis
and miliary disease)
- Not given to
immunocompromised
people and pregnant
- Not given to
immunocompromised
people and pregnant
- prevention of severe
forms of TB
(tuberculous meningitis
and miliary disease)
- contains a live but
very weakened form
of a bacteria
called Mycobacterium
bovis
- Complications
- Prognosis
- If treated >
Excellent
prognosis.
- If not treated >
mortality rate > 50%.
- Extreme ages\ Hodgkin
lymphoma\ end-stage
renal disease \ chronic
lung disease\
malnutrition\ alcoholism
- Extreme ages\ Hodgkin
lymphoma\ end-stage
renal disease \ chronic
lung disease\
malnutrition\ alcoholism
- If treated >
Excellent
prognosis.
- Airborne
precautions
- N95 Respirator
- Powered Air-Purifying
Respirator (PAPR)
- Airborne Infection Isolation Room (AIIR)
- N95 Respirator
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.