21668086
Description
Mind Map by Michal Silver, updated more than 1 year ago
More
Stroke
- Pathology
- Treatment
- Prevention
- Non-modifiable
- Age (>55), male,
African-American, family
history
- Age (>55), male,
African-American, family
history
- Modifiable
- Lifestyle
- Incorporate exercise, decrease
sodium intake, decrease alcohol
consumption, smoking cessation
- Incorporate exercise, decrease
sodium intake, decrease alcohol
consumption, smoking cessation
- heart conditions (atrial
fibrillation), conditions of
coagulability, hypertension,
diabetes, obesity
- Lifestyle
- Non-modifiable
- Drug Therapy
- TIA
- antiplatelet medications; ASA (aspirin)
- statins; lsimvastatin (zocor), ovastatin
- antiplatelet medications; ASA (aspirin)
- TIA with AF
- apixaban (Eliquis),
rivaroxaban (Xarelto),
dabigatran (Pradaxa)
- apixaban (Eliquis),
rivaroxaban (Xarelto),
dabigatran (Pradaxa)
- Ischemic
- recombinant tissue
plasminogen activator (tPA),
tPA can place pt at risk of
hemorrhage
- recombinant tissue
plasminogen activator (tPA),
tPA can place pt at risk of
hemorrhage
- Hemorrhagic
- antihypertensives, seizure prevention
- antihypertensives, seizure prevention
- Hemorrhagic (SAH)
- Ca channel blockers;
nimodipine (Nimotop)
- vasodilators; IV
milrinone
- Ca channel blockers;
nimodipine (Nimotop)
- TIA
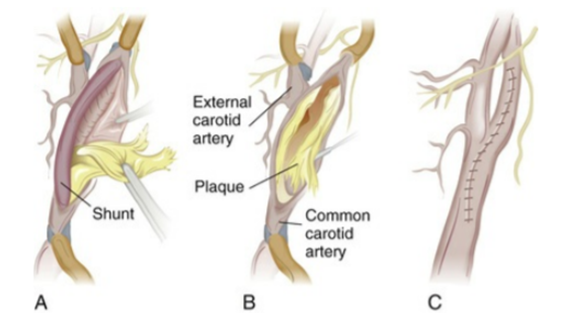
- Surgical
- TIA
- carotid endarterectomy,
extracranial-to-intracranial artery
bypass, transluminal angioplasty
- carotid endarterectomy,
extracranial-to-intracranial artery
bypass, transluminal angioplasty
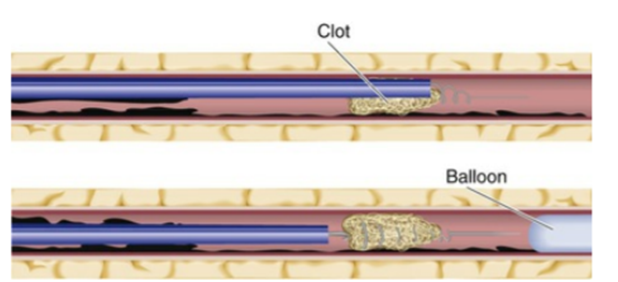
- Ischemic
- endovascular treatment (via
catheter and wire)
- endovascular treatment (via
catheter and wire)
- Hemorrhagic
- Guglielmi detachable coil
- Guglielmi detachable coil
- TIA
- Acute Care
- Prevent increased ICP
- CSF drainage
- osmotic agents; mannitol (Osmitrol)
- surgical; bone flap removal
- seizures; phenytoin (Dilantin),
levetiracetam (Keppra),
- core body temperature;
acetaminophen
- CSF drainage
- assessment and diagnostics within 4.5
hours of admission, airway, breathing,
circulation, pt will receive (tPA) within an
hour if ischemic, supplemental oxygen (if
needed), monitor for neurological deficits,
hydralazine, labetolol (if BP >220/120),
supplemental IV fluids (monitor electrolytes
to avoid hyperglycemia)
- Prevent increased ICP
- Rehabilitation
- once patient is stable
- once patient is stable
- Prevention
- Diagnostic Studies
- Other: CSF analysis,
Coagulation studies,
CBC, Electrolytes,
blood glucose, Hb A1C,
Lipid profile, renal and
hepatic studies
- Diagnosis
of Stroke:
CT scan,
CT
angiography,
MRA, MRI
- Cardiac Assessment:
Cardiac markers
[Troponin,
Creatine-kinase-MB, Chest
radiograph,
Echocardiography,
Electrocardiogram]
- Cerebral Blood Flow:
carotid angiography,
carotid duplex scanning,
cerebral angiography,
digital subtraction
angiography, transcranial
Doppler ultrasonography
- Other: CSF analysis,
Coagulation studies,
CBC, Electrolytes,
blood glucose, Hb A1C,
Lipid profile, renal and
hepatic studies
- Nursing Management
- Nursing Diagnoses
- risk for aspiration, impaired
physical mobility, impaired
verbal communication, unilateral
neglect, impaired swallowing,
impaired urinary eliminatio,
situational low self-esteem,
decreased intracranial
adaptive capacity
- risk for aspiration, impaired
physical mobility, impaired
verbal communication, unilateral
neglect, impaired swallowing,
impaired urinary eliminatio,
situational low self-esteem,
decreased intracranial
adaptive capacity
- Nursing
Assessment
- Primary
Assesment:
- Subjective
Data: Past
health
history,
medications,
symptoms
- Objective Data:
General,
respiratory,
cardiovascular,
Gastro-intestinal,
Urinary,
Neruological,
Diagnostic Test
- Subjective
Data: Past
health
history,
medications,
symptoms
- Secondary
Assessment
- Comprehensive
Neurological Exam -
Level of
consciousness
-cognition -motor
abilities -cranial
nerve function
-sensation
-proprioception
-cerebellar function
-deep tendon
reflexes
- Comprehensive
Neurological Exam -
Level of
consciousness
-cognition -motor
abilities -cranial
nerve function
-sensation
-proprioception
-cerebellar function
-deep tendon
reflexes
- Primary
Assesment:
- Planning
- Patient, Nurse &
Family Establish Goals:
- Maintain stable/improved LOC,
attain maximum physical
functioning, attain maximum
self-care abilities and skills,
maintain stable body functions,
maximize communication
abilities, maintain adequate
nutrition, avoid complications
of stroke, maintain effective
personal and family coping
skills
- Maintain stable/improved LOC,
attain maximum physical
functioning, attain maximum
self-care abilities and skills,
maintain stable body functions,
maximize communication
abilities, maintain adequate
nutrition, avoid complications
of stroke, maintain effective
personal and family coping
skills
- Patient, Nurse &
Family Establish Goals:
- Implementation
- Health Promotion, Acute
Intervention,
- Manage HTN with
antihypertensives, control of
blood glucose in diabetes
cases, treat AF with
anticoagulants, smoking
cessation,
- Neurological
- Monitor signs of
stroke extension,
use of The
Canadian
Neurological Scale
for monitoring,
changes in LOC,
monitor ICP and
cranial perfusion
pressure
- Monitor signs of
stroke extension,
use of The
Canadian
Neurological Scale
for monitoring,
changes in LOC,
monitor ICP and
cranial perfusion
pressure
- Respiratory
- Decreased muscle
strength, risk of
atelectasis and
pneumonia,
dysphagia leading
to aspiration
pneumonia or
airway obstruction,
may require enteral
feeding and/or
artificial airway
- Decreased muscle
strength, risk of
atelectasis and
pneumonia,
dysphagia leading
to aspiration
pneumonia or
airway obstruction,
may require enteral
feeding and/or
artificial airway
- Cardiovascular
- Manage secondary
cardiac diseases, Fluid
retention leading to
increased ICP (monitor
IV fluids, fluid intake and
output), Monitor cardiac
rhythms, vitals,
pulmonary congestion,,
orthostatic hypertension,
deep-vein thrombosis
(ROM exercises,
compression devices,
low-molecular-weight
heparin)
- Manage secondary
cardiac diseases, Fluid
retention leading to
increased ICP (monitor
IV fluids, fluid intake and
output), Monitor cardiac
rhythms, vitals,
pulmonary congestion,,
orthostatic hypertension,
deep-vein thrombosis
(ROM exercises,
compression devices,
low-molecular-weight
heparin)
- Musculo-Skeletal
- Prevent muscular atrophy and joint
contractures, ROM exercises, positioning,
joints positioned higher than proximal joint
(prevent edema), use of slings and
splints on extremities
- Prevent muscular atrophy and joint
contractures, ROM exercises, positioning,
joints positioned higher than proximal joint
(prevent edema), use of slings and
splints on extremities
- Integumentary
- Manage loss of
sensation, repositioning
(20 minutes per side),
cushions, skin hygiene,
mobility
- Manage loss of
sensation, repositioning
(20 minutes per side),
cushions, skin hygiene,
mobility
- Nutrition care
outlined by SLP or
OT, test of gag
reflex, chewing, and
swallowing
- GI/Urinary
- Manage constipation
with stool
softeners/fibre,
laxatives,
suppositories, monitor
fluid intake,
- prevent incontinence,
limit use of catheter,
adequate fluid intake,
scheduled toileting
- Manage constipation
with stool
softeners/fibre,
laxatives,
suppositories, monitor
fluid intake,
- Patient may
experience
aphasia, a nurse
should speak in
simple sentences,
use calm tone, and
hand gestures or
assistive devices
- Homonymous
hemianopia/neglect
syndrome may effect
patients ability to
interact with the
environment
- Health Promotion, Acute
Intervention,
- Evaluation
- Ambulatory & Home Care
- Interdisciplinary and
family-centered
- Eating, toileting, and walking, prevention of
additional muscle loss, muscle spasticity
and regaining voluntary control, balance
training, posture control, use of walkers,
wheelchairs, or splints
- Monitor patients weight and activity
level, signs of malnutrition/dehydration,
use of assistive devices. Regular
bowel elimination, possibly with the
use of stool softener/suppository.
Assess for urinary retention,
reduction in the need for
incontinence products
- Sensory-perceptual deficits require
a clear environment and increased
use of paralyzed side
- Affect and coping should be monitored
look for signs of maladjustment, Patient
should begin reintegrating into community
- Interdisciplinary and
family-centered
- Ambulatory & Home Care
- Nursing Diagnoses
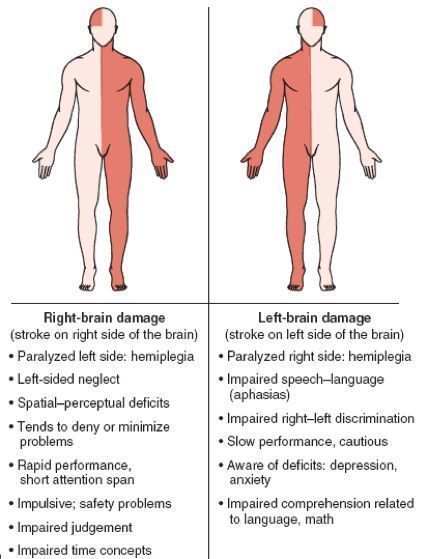
- Clinical Manifestations
- Motor Function
- Communication:
aphasia &
dysarthria
- Mood and Affect:
exaggerated or
unpredictable
emotional responses,
frustration and/or
depression
- Spatial-Perceptual: Alterations
- Elimination
Urination & BM:
Frequency,
urgency,
incontinence &
constipation
- Patient &
Caregiver
Teaching Guide
- Motor Function
- Complications
- Acute
- Subarachnoid Hemorrhage
- Rebleeding
- Rebleeding
- Cerebral aneurysm
- Death
- Death
- Dysphagia
- Risk for aspiration
- Airway obstruction
- Risk for aspiration
- Immobility
- DVT
- Skin breakdown
- Shoulder-hand syndrome
- DVT
- Lack of innervation
- Loss of sensation
- Loss of sensation
- Hydrocephalus
- Intracerebral hemmorhage
- Bleeding into ventricles
- Bleeding into ventricles
- Intracerebral hemmorhage
- Neurological
- Hypoxia and hypercarbia
- Secondary neuronal damage
- Brain damage
- Brain damage
- Secondary neuronal damage
- Dehydration
- Brain damage
- Brain damage
- Overhydration
- Increase in cerebral edema
- Compromise perfusion
- Brain damage
- Brain damage
- Compromise perfusion
- Increase in cerebral edema
- Hyperthermia
- Increase in brain metabolism
- Increase in brain metabolism
- Brain herniation
- Increased ICP
- Death
- Seizures
- Death
- Increased ICP
- Hypoxia and hypercarbia
- Subarachnoid Hemorrhage
- Post Stroke
- Lack of Innervation
- Muscle atrophy
- Muscle atrophy
- Hypertension
- Diabetes
- Hyperglycemia
- Lack of Innervation
- Comorbidities
- Manage them in acute phase
- Diabetes
- Hypertension
- Heart Disease
- Diabetes
- Manage them in acute phase
- Prognosis
- Treatments
- Thrombolytic Drugs
- Intracranial Hemorrhage
- Intracranial Hemorrhage
- Death
- Intracranial Hemorrhage
- Excess heparin
- Hemorrhage
- Hemorrhage
- Thrombolytic Drugs
- Acute
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.