6846408
Description
Mind Map by Samantha Salonga, updated more than 1 year ago
|
|
Created by Samantha Salonga
about 8 years ago
|
|
Hypertrophic
Cardiomyopathy
- SIGNS & SYMPTOMS
- Subjective
- Exertional chest pains
- Light-headedness
- Syncope
- Palpitations
- Dyspnea (Argulian,
Sherrid, & Messerli, 2016)
- Dyspnea (Argulian,
Sherrid, & Messerli, 2016)
- Palpitations
- Syncope
- Light-headedness
- Exertional chest pains
- Objective
- Additional heart sounds
- Murmur
- Prominent apical pulse
- Brisk/bifid carotid pulse
(Argulian, Sherrid, & Messerli,
2016)
- Brisk/bifid carotid pulse
(Argulian, Sherrid, & Messerli,
2016)
- Prominent apical pulse
- Murmur
- Assessments
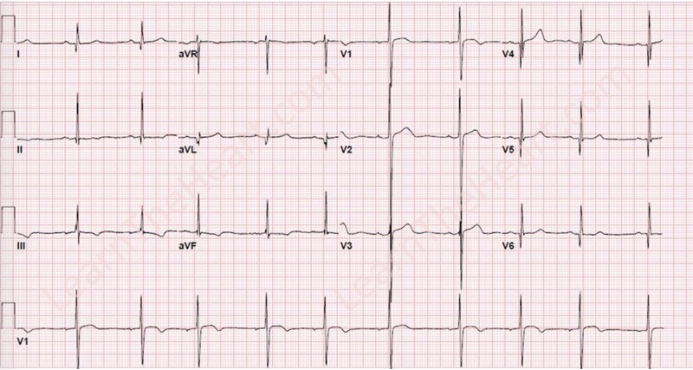
- Diagnostic Tests:
Electrocardiogram
- P wave abnormalities
- Repolarization changes
- Axis deviations (Argulian, Sherrid,
& Messerli, 2016)
- Axis deviations (Argulian, Sherrid,
& Messerli, 2016)
- T waves diffuse large and
inverted if cardiac apex
abnormally thick
- Large “dagger like” septal
Q-waves (Lome, 2016)
- Large “dagger like” septal
Q-waves (Lome, 2016)
- Repolarization changes
- P wave abnormalities
- Diagnostic Tests:
Electrocardiogram
- Additional heart sounds
- Subjective
- TREATMENTS
- Dependent on symptoms
- Arrhythmias (Argulian, et al., 2016)
- Anticoagulation
- Rhythm Control
- Cadioversion
- Antirhythmic agents
- Cadioversion
- Rhythm Control
- Anticoagulation
- Left Ventricular Outflow Obstruction
- Beta blockers: reduced inotropy
and longer ventricular filling times
reduce obstructive symptoms
(Argulian, et al., 2016).
- Disopyramide can be used in
combination with beta blockers
and should be considered before
any invasive therapies (Argulian,
et al., 2016).
- Surgery and catheter-based
treatment of outflow obstruction,
associated with low complications
and successful relief of obstruction
(Argulian, et al., 2016).
- Surgical Myectomy for young patients with low rsk
- Catheter-based care for older patient with higher risks
and comorbidities
- Surgical Myectomy for young patients with low rsk
- Surgery and catheter-based
treatment of outflow obstruction,
associated with low complications
and successful relief of obstruction
(Argulian, et al., 2016).
- Disopyramide can be used in
combination with beta blockers
and should be considered before
any invasive therapies (Argulian,
et al., 2016).
- Beta blockers: reduced inotropy
and longer ventricular filling times
reduce obstructive symptoms
(Argulian, et al., 2016).
- Non-obstructive (Argulian, et al., 2016)
- Beta Blockers
- Calcium Channel Blockers
- Beta Blockers
- Arrhythmias (Argulian, et al., 2016)
- Dependent on symptoms
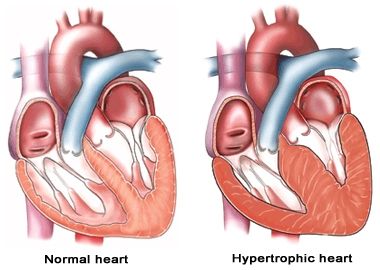
- PATHOPHYSIOLOGY
- First signs recognized in the pathophysiology of
hypertrophic cardiomyopathy are pathogenic
mutations in cardiac sarcomere
- Mitral valve apparatus abnormalities
- Diagnosis confirmed via genetic testing
- Abnormal loading conditions present causing left
ventricle to require more effort. (HTN, aortic
stenosis)
- Left ventricle hypertrophy can lead to obstruction
of the left ventricle outflow which can result in atrial
arrhythmias, embolic phenomena, and HF (Argulian,
Sherrid, & Messerli, 2016
- May lead to sudden cardiac death in young
healthy individuals (Jacoby, Depasquale, &
McKenna, 2013).
- May lead to sudden cardiac death in young
healthy individuals (Jacoby, Depasquale, &
McKenna, 2013).
- Left ventricle hypertrophy can lead to obstruction
of the left ventricle outflow which can result in atrial
arrhythmias, embolic phenomena, and HF (Argulian,
Sherrid, & Messerli, 2016
- Abnormal loading conditions present causing left
ventricle to require more effort. (HTN, aortic
stenosis)
- Diagnosis confirmed via genetic testing
- Mitral valve apparatus abnormalities
- First signs recognized in the pathophysiology of
hypertrophic cardiomyopathy are pathogenic
mutations in cardiac sarcomere
- NURSING IMPLICATIONS
- Must be able to interpret ECG reading (Palmer, 2013).
- Advocate for other tests if HCM is suspected
- Advocate for other tests if HCM is suspected
- Family
History
- ECG
- Multiple sudden deaths in the family
- Review postmortem reports if possible
- Advocate for family screening
- Review postmortem reports if possible
- Assessing Heart Sounds
- Harsh systolic crescendo >> decrescendo murmur at the left sternal border
- Diminished with squatting and increases when standing
- Diminished with squatting and increases when standing
- Harsh systolic crescendo >> decrescendo murmur at the left sternal border
- ECG
- Must be able to interpret ECG reading (Palmer, 2013).
- CAUSES
- Common inherited type of cardiomyopathy. (Jacoby, Depasquale, & McKenna, 2013)
- Described as thickening of left ventricle with no apparent cause. (Argulian, Sherrid, & Messerli,
2016)
- General experience is that late development or progression of hypertrophy is
uncommon, with most cases of hypertrophy developing during adolescence and early
adulthood (Argulian, et al., 2016).
- Disease is attributed to many sarcomere gene mutations (Argulian, et al., 2016)
- "Autosomal dominant disease is predominant, with most sporadic and alternate inheritance patterns
(X-linked, mitochondrial) representing phenocopies. Disease penetrance is incomplete and
expression is variable, making the familial nature of this disease occasionally challenging to
appreciate" Argulian, et al., 2016).
- "Autosomal dominant disease is predominant, with most sporadic and alternate inheritance patterns
(X-linked, mitochondrial) representing phenocopies. Disease penetrance is incomplete and
expression is variable, making the familial nature of this disease occasionally challenging to
appreciate" Argulian, et al., 2016).
- Disease is attributed to many sarcomere gene mutations (Argulian, et al., 2016)
- General experience is that late development or progression of hypertrophy is
uncommon, with most cases of hypertrophy developing during adolescence and early
adulthood (Argulian, et al., 2016).
- Described as thickening of left ventricle with no apparent cause. (Argulian, Sherrid, & Messerli,
2016)
- Common inherited type of cardiomyopathy. (Jacoby, Depasquale, & McKenna, 2013)
- LIFESTYLE CHANGES
- Decreased physical activity
- Children are forced to quit sports or greatly decrease participation
- May hinder future career plans
- Children are forced to quit sports or greatly decrease participation
- Social Changes
- Some children have fears of informing their peers of their
condition, because they might be treated differently
- Children may be separated from social groups
- Some children have fears of informing their peers of their
condition, because they might be treated differently
- Restricting alcohol
consumption (Bratt,
et al., 2012)
- Quit
smoking
- Losing weight (Wexler
et al., 2009)
- moderate excersice
- low-sodium diet
- low-sodium diet
- moderate excersice
- Decreased physical activity
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.