7785725
Diabetes Mellitus
Type I
- ASSESSMENT
- 3 P's
- Polyuria
- Polyphagia
- Polydipsia
- Polyuria
- Weight Loss
- Weakness
- Fatigue
- Glycosuria
- 3 P's
- Risk Factors
- Genetics
- Environment
- Genetics
- Complications
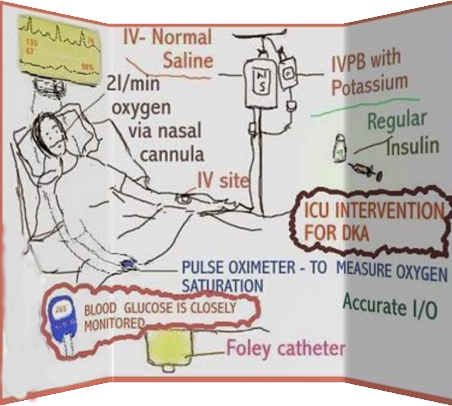
- Acute
- Diabetic
Ketaoacidosis
(DKA)
- Caused by profound
deficiency of insulin
- results in severe
metabolic, fluid and
electrolyte disturbances
- life-threatening
condition of
hyperglycaemia and
metabolic acidosis
- life-threatening
condition of
hyperglycaemia and
metabolic acidosis
- results in severe
metabolic, fluid and
electrolyte disturbances
- Caused by profound
deficiency of insulin
- Hypoglycemia
- low blood
glucose
- low blood
glucose
- Complications
Due to Diabetic
Control
- Somogyi Effect
- - rebound effect in which an overdose of
insulin causes hypoglycemia due to release
of counterregulatory hormones -
hypoglycaemic episode tends to occur during
the night (during hours of sleep) or at a time
when it is not recognized
- low blood glucose
- low blood glucose
- - rebound effect in which an overdose of
insulin causes hypoglycemia due to release
of counterregulatory hormones -
hypoglycaemic episode tends to occur during
the night (during hours of sleep) or at a time
when it is not recognized
- Dawn Phenomenon
- - characterized by a hyperglycaemic episode due to
release of counterregulatory hormones (increased
levels of fasting blood glucose, or insulin
requirements, or both without antecedent
hypoglycaemia) - tends to occur during the
predawn hours (5 AM - 9 AM) or when the
individual wakes up - possible factors for
occurrence: - growth hormone/cortisol possible
factors
- - characterized by a hyperglycaemic episode due to
release of counterregulatory hormones (increased
levels of fasting blood glucose, or insulin
requirements, or both without antecedent
hypoglycaemia) - tends to occur during the
predawn hours (5 AM - 9 AM) or when the
individual wakes up - possible factors for
occurrence: - growth hormone/cortisol possible
factors
- Somogyi Effect
- Diabetic
Ketaoacidosis
(DKA)
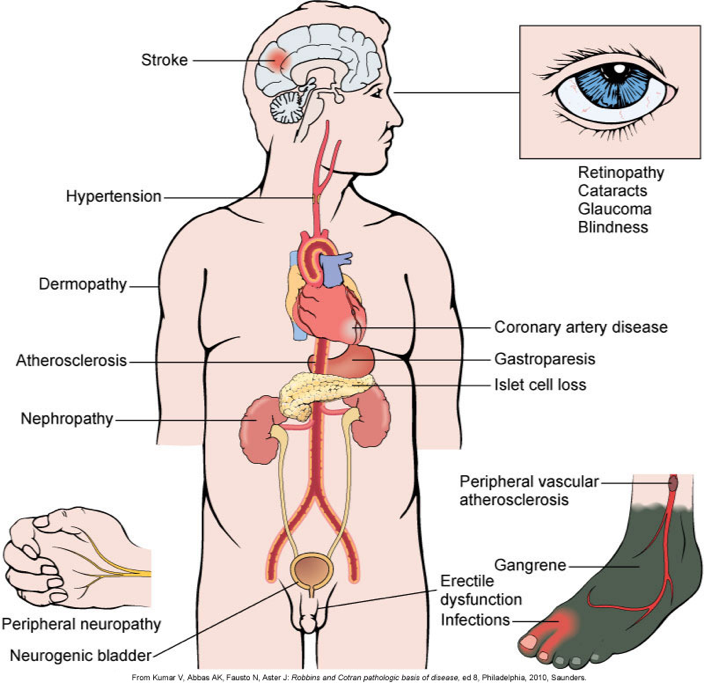
- Chronic
- Immune
System
- impaired healing; chronic skin
infections; periodontal disease;
urinary tract infections; lung
infections and et cetera
- impaired healing; chronic skin
infections; periodontal disease;
urinary tract infections; lung
infections and et cetera
- Ingtegumentary
Complications
- Microvascular
Angiopathy
- Macrovascular
Angiopathy
- Ingtegumentary
Complications
- Immune
System
- Acute
- Nursing Assessments
- Symptom analysis, fluid status, I&O,
nutritional status, weight, energy level, GI
symptoms, neurological assessment,
history of recent infections or difficulty
healing
- Symptom analysis, fluid status, I&O,
nutritional status, weight, energy level, GI
symptoms, neurological assessment,
history of recent infections or difficulty
healing
- DIAGNOSIS
- Diagnostic Tests
- Urine Tests
- postive for presence of glucose, ketones and proteins
- postive for presence of glucose, ketones and proteins
- Fasting Plasma Glucose (FPG)
- ≥ 7 mmol/L
- ≥ 7 mmol/L
- Casual Blood Glucose Test
- ≥11 mmol/L plus classic symptoms
- ≥11 mmol/L plus classic symptoms
- Oral Glucose Tolerance Test (OGTT)
- ≥11.1 mmol/L when a glucose load of 75 g is used
- ≥11.1 mmol/L when a glucose load of 75 g is used
- Glycosylated Hemoglobin
(A1C)
- CDA ≤7.0% ; Normal range is <6.0%
- CDA ≤7.0% ; Normal range is <6.0%
- Fasting Plasma Glucose (FPG)
- Urine Tests
- Nursing
Diagnosis
- Diagnostic Tests
- PLANNING
- Overall
Goals
- Active patient participation
- Maintain normal glucose level (b/t 4.0-6.0mmol/L)
- Prevent or delay chronic complications
- Lifestyle adjustments with minimal stress
- Few/no episodes of acute hyperglycemic/hypoglycemia emergencies
- Active patient participation
- Overall
Goals
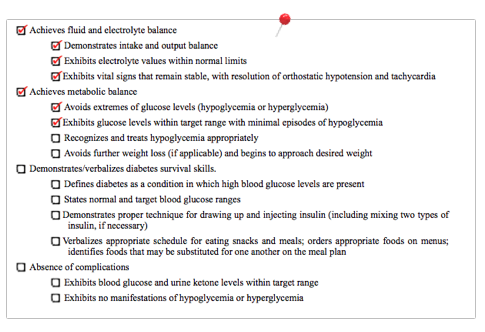
- EVALUATION
- Expected patient outcomes may include the following:
- Expected patient outcomes may include the following:
- IMPLEMENTATION
- Acute
interventaion
- Hypoglycemia
- Patient Alert To Swallow
- 15 to 20 g of a simple
carbohydrate or 175 mL of
fruit juice or Regular soft
drink
- 15 to 20 g of a simple
carbohydrate or 175 mL of
fruit juice or Regular soft
drink
- Patient Not Alert To Swallow
- Administer 1 mg of glucagon
IM or subcutaneously
- Administer 1 mg of glucagon
IM or subcutaneously
- Patient Alert To Swallow
- DKA
- Administer continuous low-dose
short acting insulin infusion after
initial dose of insulin
- Monitor: BG hourly,
electrolytes every
2hours after start of IV
therapy, hourly fluid
input and output
- Administer continuous low-dose
short acting insulin infusion after
initial dose of insulin
- Stress of illness and surgery
- Frequent monitor BG level, ketone
testing if glucose >14 mmol/L,
continue with insulin therapy,
regular meal plan - increase intake
of non-caloric fluids
- Frequent monitor BG level, ketone
testing if glucose >14 mmol/L,
continue with insulin therapy,
regular meal plan - increase intake
of non-caloric fluids
- Hypoglycemia
- chronic
intervention
- Smoking Cessation
- Lifestyle changes
- control blood lipids, HTN, BG
- control blood lipids, HTN, BG
- Drug therapy
- antiplatelet agents (ex. aspirin or
clopidogrel
- antiplatelet agents (ex. aspirin or
clopidogrel
- Smoking Cessation
- General treatments
- Drug
therapy
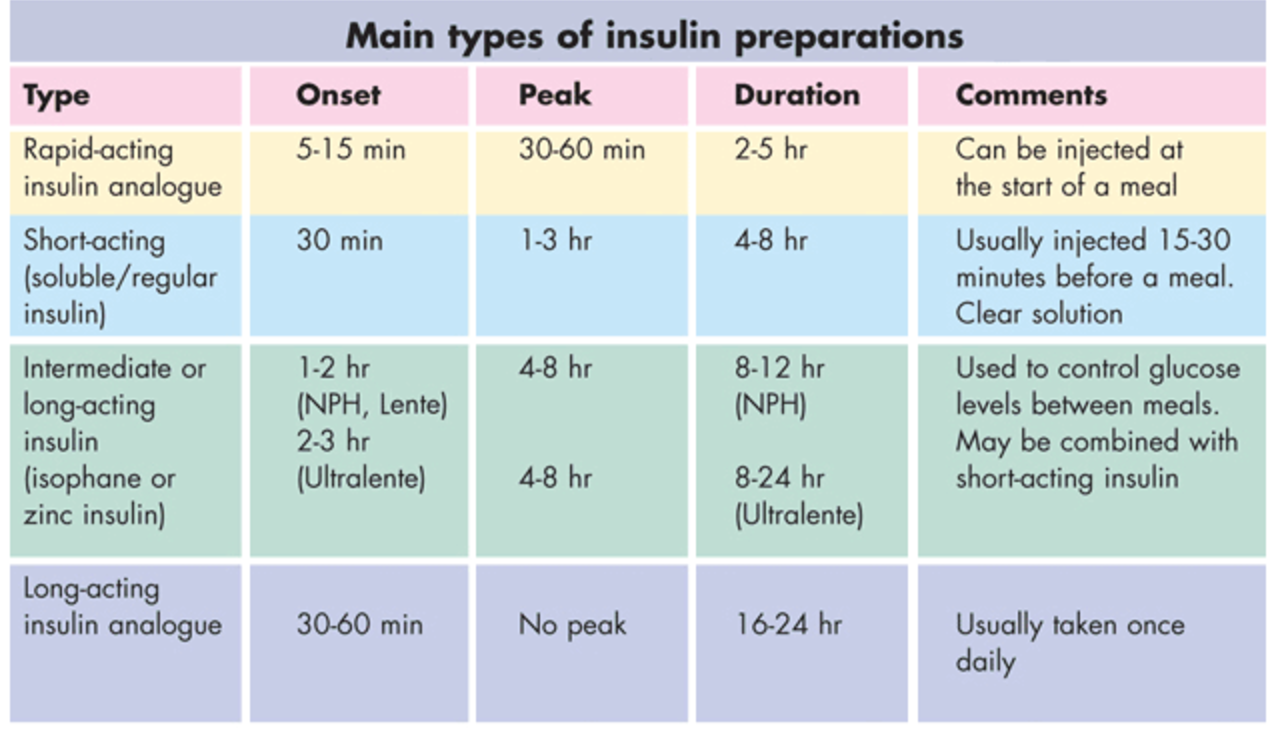
- Insulin Injections
- Bolus
- Lispro, Aspart, Glulisine
- Lispro, Aspart, Glulisine
- Basal
- NPH
- glargine
- NPH
- Choice of insulin depends on many factors: Age , Duration of DM ,Family
lifestyle, Socioeconomic factors ,Family, patient, & physician preferences
- at bed time or in the
morning, CAN NOT be mixed
with other insulin or solution
- Bolus
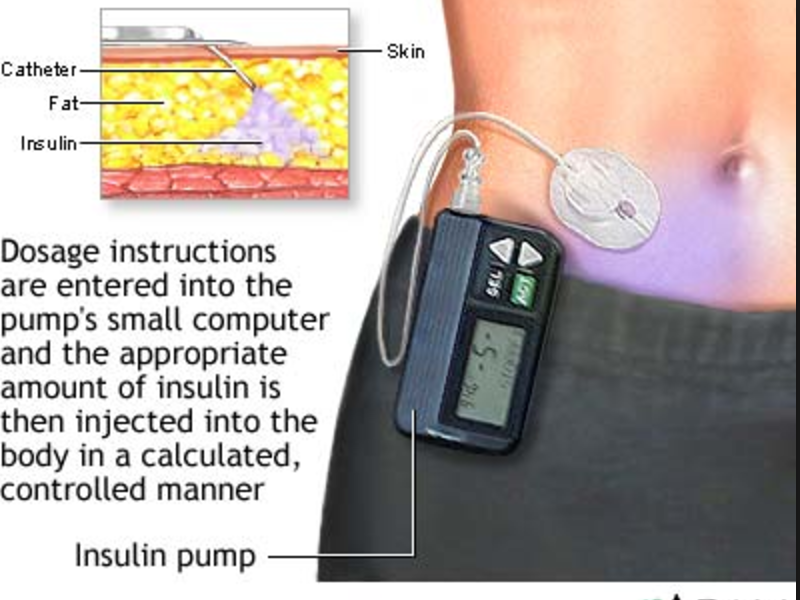
- Insulin pump
- continuous subcutanous infusion
- continuous glucose monitor
- continuous subcutanous infusion
- Insulin Injections
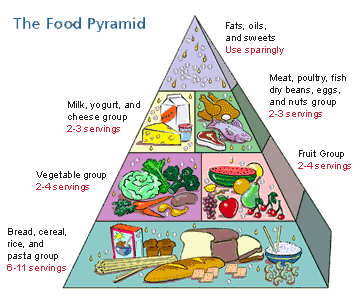
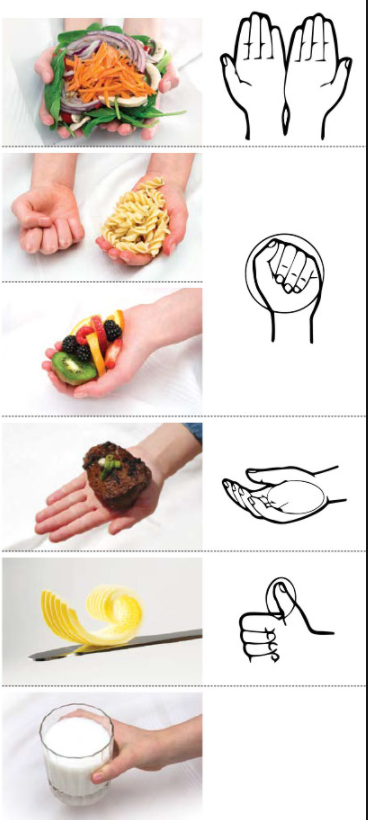
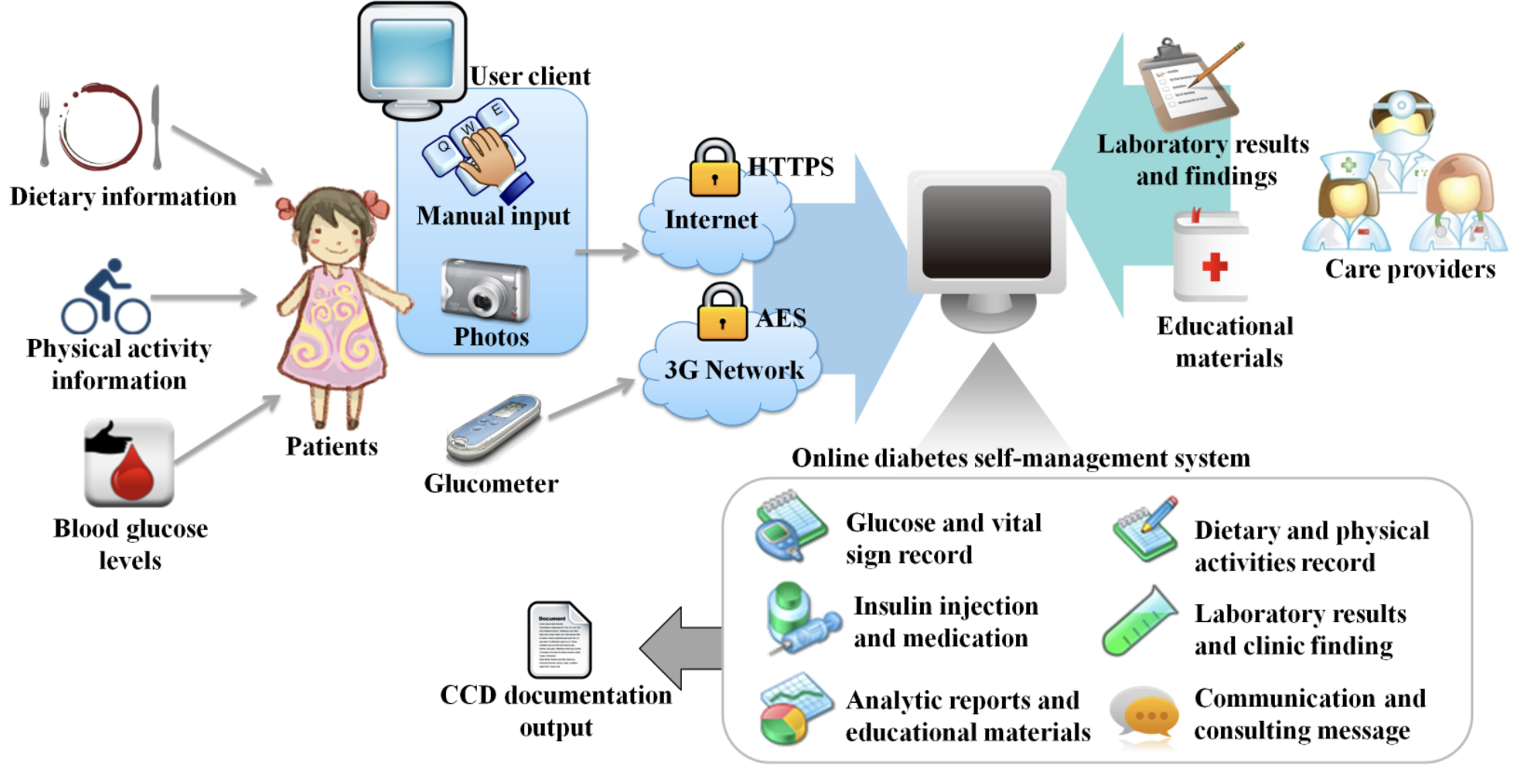
- Nutrition
- Canadian diabetes association [CDA] - provides
variety of nutrition teaching tools
- Alcohol
- no benefit at all, high in calories
- *Promote hypertriglyceridemia, sever hygolycemia
- no benefit at all, high in calories
- reduce saturated fats & trans fats to
<7% of energy intake
- foods rich in
polyunsaturated
omega 3 fatty acids
and plant oils
- foods rich in
polyunsaturated
omega 3 fatty acids
and plant oils
- Proteins: Limit to 15% of total energy intake
- carbs counting
- <10% daily energy
should come from
sugar
- <10% daily energy
should come from
sugar
- counselling from a Registered dietitian
- Children/adolescents: normal growth
& development should be considered
- Alcohol
- balance is
essential
- Canadian diabetes association [CDA] - provides
variety of nutrition teaching tools
- Exercise
- Essential part of management
- insulin receptor sites,
glucose level, carbs snacks
(every 30min during
exercise to prevent
hypolgycemia), weight loss
- insulin receptor sites,
glucose level, carbs snacks
(every 30min during
exercise to prevent
hypolgycemia), weight loss
- after meal, personalized
plan, start slowly with
gradual progression
- Essential part of management
- Drug
therapy
- Health Promotion
- Family & patient
education
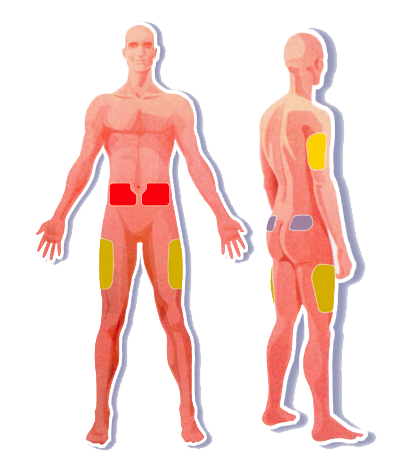
- Teach insulin administration
- subcutaneous injection.
self administration
abdomen is preferred site.
Abdoment >
arm>thigh>buttock
- Rotate injections
- do not inject in site to be
exercised
- do not inject in site to be
exercised
- Rotate injections
- subcutaneous injection.
self administration
abdomen is preferred site.
Abdoment >
arm>thigh>buttock
- Teach signs and symptoms of
hypoglycaemia &
hyperglycaemia
- Teach self-monitoring of glucose
- Teach proper diabetic foot care,
need for proper shoe fit and
wound care
- Teach what to do for sick days:
maintain/increase insulin when common
sickness occurs such as a cold and monitor
glucose more often than usual + maintain
appropriate fluid intake
- Teach insulin administration
- Screening
- To Test/Screen for Diabetes
- Testing/Screening for diabetes should be considered for
the following: - individuals 45 years of age and older -
obese - 1st-degree relative w/ diabetes - members of a
high-risk group - have hypertension or hyperlipidemia -
met the criteria (IFG, IGT, elevated AIC) for increased
risked of diabetes on previous testing
- Testing/Screening for diabetes should be considered for
the following: - individuals 45 years of age and older -
obese - 1st-degree relative w/ diabetes - members of a
high-risk group - have hypertension or hyperlipidemia -
met the criteria (IFG, IGT, elevated AIC) for increased
risked of diabetes on previous testing
- For Those Already
Diagnosed with
Diabetes
- dyslipidemia at diagnosis.
- dilated eye examinations
- microalbuminuria in urine; serum creatinine
- dyslipidemia at diagnosis.
- To Test/Screen for Diabetes
- Family & patient
education
- Acute
interventaion
- DEFINITION
- the destruction of pancreatic
beta cells that leads to insulin
dependence
- Etiology & Pathophysiology
- Type 1A -- Immune Mediated
Diabetes (aka "Juvenile-onset")
- thought to be a result from the interaction of:
(1) genetic predisposition -- HLA (human
leukocyte antigens) (2) environmental trigger
(3) T-cell mediated hypersensitivity reaction
against beta cell antigens
- thought to be a result from the interaction of:
(1) genetic predisposition -- HLA (human
leukocyte antigens) (2) environmental trigger
(3) T-cell mediated hypersensitivity reaction
against beta cell antigens
- Type1B -- Idiopathic Diabetes
- beta cell destruction in which no
evidence of autoimmunity is
present - strongly inherited
- beta cell destruction in which no
evidence of autoimmunity is
present - strongly inherited
- Hyperglycaemia
- excess of glucose in the
bloodstream,
- Microvascular
Angiopathy
- - results from thickening of vessel membranes in
capillaries and arterioles due to chronic
hyperglycaemia
- - results from thickening of vessel membranes in
capillaries and arterioles due to chronic
hyperglycaemia
- Microvascular
Angiopathy
- - diseases of large and medium-sized blood
vessels promoted by altered lipid metabolism
- - diseases of large and medium-sized blood
vessels promoted by altered lipid metabolism
- Microvascular
Angiopathy
- excess of glucose in the
bloodstream,
- Hyperglycaemia
- Type 1A -- Immune Mediated
Diabetes (aka "Juvenile-onset")
- Risk Factors
- Autoimmune
- Viral
- Autoimmune
- Clinical Manifestations
- Etiology & Pathophysiology
- the destruction of pancreatic
beta cells that leads to insulin
dependence
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.