5336941
Descrição
Mapa Mental por Samantha Fredman, atualizado more than 1 year ago
|
|
Criado por Samantha Fredman
mais de 8 anos atrás
|
|
Principles of fractures and dislocations
- Stress fracture
- normal bone
- repetitive stress
- normal bone
- Pathological fracture
- abnormal bone
- metastatic disease
- benign lesion
- metastatic disease
- vs
- physiological stress
- abnormal bone
- Force
- Direct
- break at point of impact (POI)
- + soft tissue damage
- + soft tissue damage
- break at point of impact (POI)
- Indirect
- break away from POI
- +/- soft tissue damage
- +/- soft tissue damage
- break away from POI
- Direct
- Mechanism of Injury
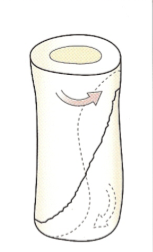
- Spiral
- TORSION
- rotational force applied to a lever
- humerus
- femur
- humerus
- rotational force applied to a lever
- TORSION
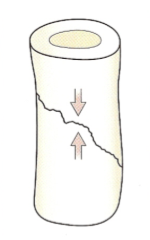
- Short Oblique
- COMPRESSION
- greenstick
- children due to thickenss of periosteum
- children due to thickenss of periosteum
- greenstick
- COMPRESSION
- Butterfly
- BENDING
- Car accident
- Comminution
- e.g. vertebral comminution
common when subject to
- e.g. vertebral comminution
common when subject to
- Car accident
- BENDING
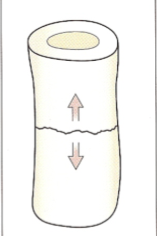
- Transverse
- TENSION
- TENSION
- Spiral
- How to describe a fracture
- open or closed?
- open- antibiotics + cleaning of bone ends
- open- antibiotics + cleaning of bone ends
- bone(s)?
- location?
- location?
- simple or comminuted?
- complete or incomplete?
- involvement of joint?
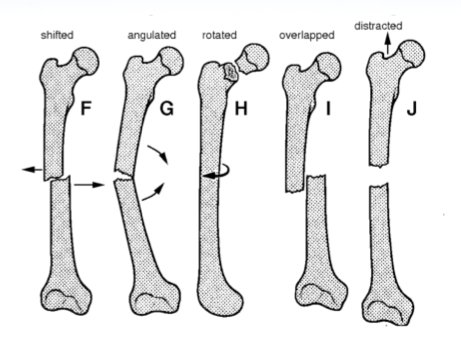
- displaced or non displaced?
- displacement
- translation
- describe with reference to distal
fragment (50%, 100%, or complete (off
ended
- describe with reference to distal
fragment (50%, 100%, or complete (off
ended
- alignment
- angulation
- angulation
- rotation
- twist
- twist
- length
- distraction
- separation
- overlap
- distraction
- translation
- displacement
- traumatic, stress or pathological?
- open or closed?
- HEALING
- INDIRECT
- In tubular bone in the absence of
rigid fixaiton
- 1. Haemotoma formation
- 2. Inflammation and Cellular
proliferation
- 3.Callus
- response to movement at the
fracture site
- stabilise
- response to movement at the
fracture site
- 4. Consolidation
- 5. Remodelling
- 1. Haemotoma formation
- In tubular bone in the absence of
rigid fixaiton
- DIRECT
- fracture
immobilised
- example
- Fixed with metal plate
- impacted cancellous
bone fracture
- Fixed with metal plate
- fracture healing occurs directly between fragments WITHOUT
CALLUS
- example
- fracture
immobilised
- HOW LONG?
- dependant
on
age,
nutrition,
general
health,
blood
supply,
type
of
fracture,
fracture
stability
- dependant
on
age,
nutrition,
general
health,
blood
supply,
type
of
fracture,
fracture
stability
- promoted by physiological loading of bone (DONT IMMOBILISE)
- INDIRECT
- CLINICAL FEATURES
- LOOK
- swelling
- bruising
- deformity
- skin intact?
- swelling
- FEEL
- bony tenderness
- crepitus
- grating
bone
against
bone
- grating
bone
against
bone
- pulses
- associated injuries
- tense compartment= compartment syndrome
- tense compartment= compartment syndrome
- bony tenderness
- MOVE
- maybe not if patient awake and conscious
- x-ray might be more appropriate
- x-ray might be more appropriate
- maybe not if patient awake and conscious
- NEUROVASCULAR EXAM
- all nerves and vessels traversing the compartment
- at presentaiton AND after any intervention
- at presentaiton AND after any intervention
- all nerves and vessels traversing the compartment
- LOOK
- IMAGING
- X-RAY
- rule of 2's
- views, joints, limbs, injuries, occassions
- views, joints, limbs, injuries, occassions
- rule of 2's
- ADVANCED IMAGING
- Technitium Bone Scan
- may be "cold" if performed within 48-72 hours of
injury
- may be "cold" if performed within 48-72 hours of
injury
- CT
- complex or interarticular fractures
- used to define bony anatomy
- complex or interarticular fractures
- MRI
- assessment of associate structures
- spinal cord, nerve root, ligament injuries
- spinal cord, nerve root, ligament injuries
- soft tissue anatomy definition
- assessment of associate structures
- Technitium Bone Scan
- X-RAY
- TREATMENT
- REDUCTION
- aim for adequate apposition and
normal alignment
- closed
- + anasthesia
- distal limb pulled in line with bone
- fragments disengage and are
repositioned
- alignment adjusted in each plane
- use
- most fractures in children
- for fractures that are stable after reduction
- can be fixated
- can be fixated
- Unstable fractures can be reduced prior to internal fixation
- most fractures in children
- + anasthesia
- open
- operative reduction under direct vision
- operative reduction under direct vision
- aim for adequate apposition and
normal alignment
- FRACTURE IMMOBILISATION
- casting/ FIXATION
- continuous traction
- typically children
- typically children
- cast splintage
- funcitonal bracing
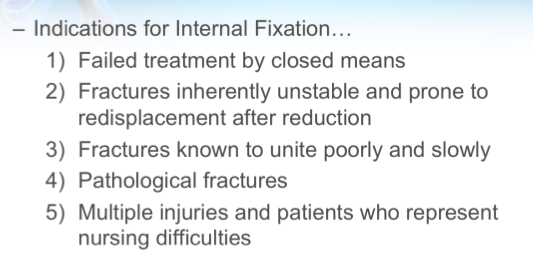
- internal fixation
- wires
- plates and screws
- intermedullary nails
- wires
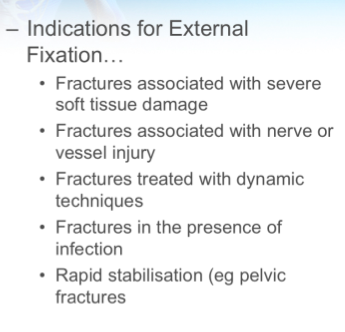
- external fixation
- internal vs External
- casting/ FIXATION
- REHAB
- REDUCTION
- COMPLICATIONS
- EARLY
- vascular injury
- nerve injury
- shoulder- axillary
- humerus- radial
- humerus supracondylar-
radial or median
- hip- sciatic
- knee- fibular
- shoulder- axillary
- compartment syndrome
- 5 P's
- pain out of
proportion to
injury and
pain on
passive
stretch most
important
- pain out of
proportion to
injury and
pain on
passive
stretch most
important
- 5 P's
- fracture blisters
- infection
- vascular injury
- LATE
- delayed union/ nonunion
- Injury factors
- treatment factors
- Pt factors e.g. smoking, NSAIDs, drinking
- Hypertrophic non-union: florid periosteal new bone formation,
wants to heal- biology of healing okay just needs stability
- Atrophic non-union- no signs of healing, needs improved biology
- Injury factors
- malunion
- avascular necrosis
- Femoral head, scaphoid, talus
- Femoral head, scaphoid, talus
- growth disturbance
- joint impairment
- pain syndromes
- delayed union/ nonunion
- EARLY
Anexos de mídia
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quer criar seus próprios Mapas Mentais gratuitos com a GoConqr? Saiba mais.