17726185
Beschreibung
Mindmap von Charles Naveen, aktualisiert more than 1 year ago
|
|
Erstellt von Charles Naveen
vor mehr als 5 Jahre
|
|
Hypovolemic shock
- Patients' background
- Mrs.Muna
- 45 years old
- Housewife
- Got into an accident
- 45 years old
- Mrs.Muna
- Physical examination
- Pale
- Dehydrated
- Disoriented
- Obese woman
- Abdomen and right lower limb bruised and wounded
- Multiple abrasions and ecchymosis of abdomen
- Multiple abrasions and ecchymosis of abdomen
- Vital signs
- Temperature 36.8 C
- Pulse rate 110 bpm
- BP of 56/38 mmHg
- Respiratory rate 25/min
- Temperature 36.8 C
- Marked tenderness in right hypochondrium. Mild tenderness all over
- Diminished bowel sounds
- Unable to move right leg
- A large ecchymotic area is seen on the right thigh with marked tendernes
- Pale
- Diagnostic/lab tests
- X-ray shows gas under diaphragm
- Diagnostic peritoneal lavage
- Presence of blood and intestinal contents in the peritoneal cavity.
- Presence of blood and intestinal contents in the peritoneal cavity.
- Portable X-ray shows fracture
of the right femur.
- Thoracic and cerebral injuries are excluded
- Thoracic and cerebral injuries are excluded
- X-ray shows gas under diaphragm
- Pre-operative preparations
- Put on I/V fluids through a central venous line
- Her CVP is recorded as 2mmHg
- Bladder catheterized
- 200 ml of amber colored urine is drained
- 200 ml of amber colored urine is drained
- Immediately transfused with two units of O-ve blood
- Put on I/V fluids through a central venous line
- Lab investigations
- Hb 6 g/dL,
- PCV 15%
- Blood group A –ve
- Urine microscopy shows
- (heme) granular casts (Muddy casts)
- Erythrocytes and cellular debris.
- Erythrocytes and cellular debris.
- (heme) granular casts (Muddy casts)
- Hb 6 g/dL,
- Surgery
- Laparotomy,
- lacerated liver
- perforated ileum with hemoperitoneum
- lacerated liver
- abdominal surgery and fixation of femur fracture lasted for about 6 hours.
- Laparotomy,
- Postoperative, Shifted to the surgical ICU
- given I/V fluids and monitored continuously for vital signs
- Urine output recorded as 10ml/hour in the first four hours
- Her urine output increases to 20 ml/hour in the next 24 hours
- Next day, her urine output declines to 10 ml/hour
- The output continues to decline despite I/V infusion of fluids
- The output continues to decline despite I/V infusion of fluids
- Next day, her urine output declines to 10 ml/hour
- Her urine output increases to 20 ml/hour in the next 24 hours
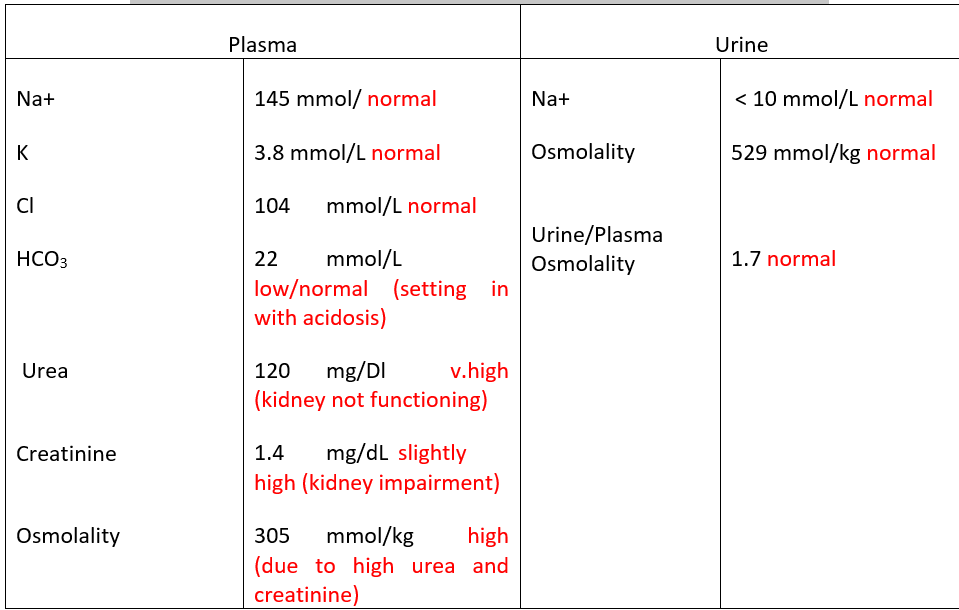
- Urine and blood samples sent for urgent laboratory investigations show
- Hemoglobin 2nd P0 day rises to 7 g/dL with a hematocrit of 25%.
- during transfusion she develops a transfusion reaction
- Transfusion is stopped and replaced by plasma expanders
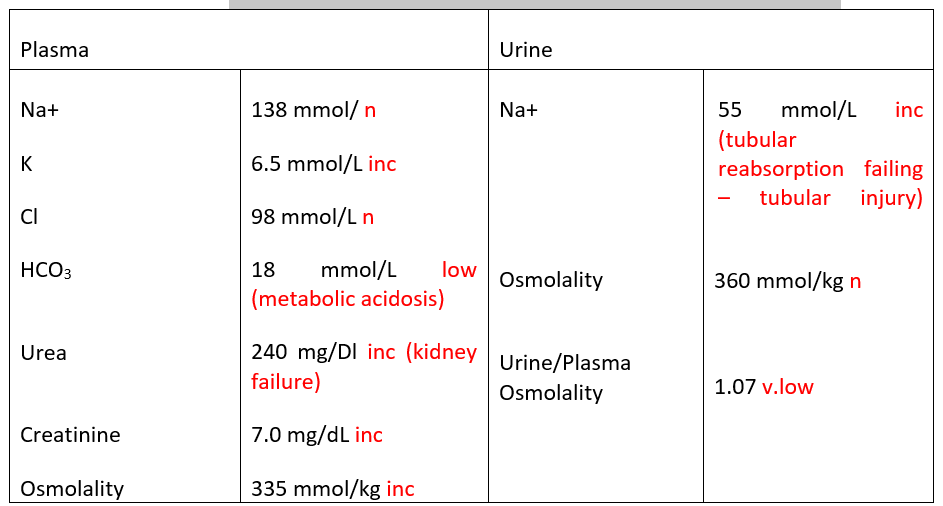
- Blood and urine specimens sent for urgent investigations show
- given I/V fluids and monitored continuously for vital signs
- Final diagnosis
- acute renal failure as a result of acute tubular necrosis
- plasma creatinine, urea and potassium show a rise leading to ECG changes
- plasma creatinine, urea and potassium show a rise leading to ECG changes
- Nephrologist advises urgent hemodialysis using an external
cannula.
- acute renal failure as a result of acute tubular necrosis
Medienanhänge
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.