8071475
Beschreibung
Mindmap von Eugene Lee, aktualisiert more than 1 year ago
|
|
Erstellt von Eugene Lee
vor fast 8 Jahre
|
|
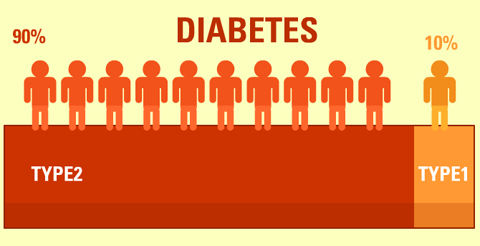
Diabetes Mellitus Type 2
- Symptoms and Diagnosis
- Symptoms and Presentation
- Acute
- Nausea
- Vomiting
- Abdominal
Pain
- Dehydration
- Hyperosmolar Nonketotic State
- Infection
- Prolonged Wound Healing
- Nausea
- Subacute
- Fatigue
- Polydipsia
- Polyuria
- Weight
Loss
- Polyphagia
- Fatigue
- Asymptomatic
- Can eventually
lead to
presentation of
symptoms
- Can eventually
lead to
presentation of
symptoms
- Acute
- Diagnostic Tests
- Hemoglobin A1C
Test
- Normal: <5.7%
Pre-diabetes: 5.7%-6.4%
Diabetes: >6.5%
- Normal: <5.7%
Pre-diabetes: 5.7%-6.4%
Diabetes: >6.5%
- Fasting Plasma Glucose Level
- Normal: <100mg/dl
Pre-diabetes: 100-125mg/dl
Diabetes: >126mg/dl
- Normal: <100mg/dl
Pre-diabetes: 100-125mg/dl
Diabetes: >126mg/dl
- Random/Casual Plasma Glucose Measurement
- Normal: <115mg/dl
Pre-diabetes: N/A
Diabetes: >200mg/dl
- Normal: <115mg/dl
Pre-diabetes: N/A
Diabetes: >200mg/dl
- Two-hour OGTT Level
- Normal: <140mg/dl
Pre-diabetes: 140-199mg/dl
Diabetes: >200mg/dl
- Normal: <140mg/dl
Pre-diabetes: 140-199mg/dl
Diabetes: >200mg/dl
- Hemoglobin A1C
Test
- Symptoms and Presentation
- Treatment
- Mild
Presentation
- Lifestyle modifications
- Diet
- Carbohydrates (Less than
10% of calorie intake)
- Fats (Less than 7%
of calorie intake)
- Proteins (Limited to
15% of calorie intake)
- Carbohydrates (Less than
10% of calorie intake)
- Exercise
- 30 minutes a day, 5
days a week
- Increases insulin receptor
sites, lowers blood sugar
- Increases insulin receptor
sites, lowers blood sugar
- 30 minutes a day, 5
days a week
- Diet
- Lifestyle modifications
- Moderate to Severe
Presentation
- Medication in conjunction with
lifestyle modifications
- Drugs
- First-line
Medication
- Biguanides
- Increases insulin sensitivity, therefore increasing
glucose transport into tissues
- Decreases glucagon, therefore
reducing glucose production
- Can decrease A1C levels by
1%
- If blood glucose hasn't improved, add another
medication
- Thiazolidinediones
- Increases insulin transport and sensitivity
on cell receptors
- Improves insulin use at tissues
- Increases insulin transport and sensitivity
on cell receptors
- Sulfonylureas
- Inhibits potassium channels on beta cells
- Influx of calcium in beta
cells
- Releases
insulin
- Releases
insulin
- Influx of calcium in beta
cells
- If blood glucose still hasn't improved, add insulin to treatment
- Insulin
- Issues with insulin therapy
- Hypoglycemia
- Could be caused
by overdose of
insulin
- Could be caused
by overdose of
insulin
- Allergic Reaction
- Lipodystrophy
- Can result in areas of insulin if injection
site is unchanged
- Can result in areas of insulin if injection
site is unchanged
- Somogyi Effect
- Rebound effect from too
much insulin causing
hypohlycemia
- Rebound effect from too
much insulin causing
hypohlycemia
- Dawn Phenomenon
- Hyperglycemia when waking in the morning due to
hormones that counter insulin during this time
- Hyperglycemia when waking in the morning due to
hormones that counter insulin during this time
- Hypoglycemia
- Issues with insulin therapy
- Insulin
- Inhibits potassium channels on beta cells
- Meglitinides
- Increases insulin production
from beta cells in pancreas
- Increases insulin production
from beta cells in pancreas
- Alpha-Glucosidase
Inhibitors
- Slows carbohydrate
absorption
- Slows carbohydrate
absorption
- Thiazolidinediones
- Increases insulin sensitivity, therefore increasing
glucose transport into tissues
- Biguanides
- First-line
Medication
- Drugs
- Medication in conjunction with
lifestyle modifications
- Mild
Presentation
- Nursing Care
- Assessment
- Patient's ability to perform ADL/iADL
- Community Dwelling
Patients
- Assisted Living
Facilities
- Hospitalized Inpatients
- Nursing Facility
(Long-term)
- Community Dwelling
Patients
- Mentally incompetent patients
- Confused, cognitively dysfunctional, or delirious
- Depression
- Confused, cognitively dysfunctional, or delirious
- Past health history
- Viral infections
- Respiratory Syncytial Virus (RSV)
causes a change in the pathways that
regulate insulin levels
- Respiratory Syncytial Virus (RSV)
causes a change in the pathways that
regulate insulin levels
- Hypertension in diabetic patients
- Beta-blockers are not ideal
medications for diabetic
patients with HTN
- Beta-blockers not ideal because they have
been shown to ↑ TG, ↓ HDL cholesterol,
heighten insulin resistance, induce
systemic weight gain, and mask
hypoglycemia.
- Beta-blockers not ideal because they have
been shown to ↑ TG, ↓ HDL cholesterol,
heighten insulin resistance, induce
systemic weight gain, and mask
hypoglycemia.
- Beta-blockers are not ideal
medications for diabetic
patients with HTN
- Recent surgery
- eg. CABG surgery alters body glucose
homeostasis and increases stress
causing HHS
- eg. CABG surgery alters body glucose
homeostasis and increases stress
causing HHS
- Viral infections
- Identify daily
basal rate and
bolus doses
- Obese individuals are more likely
to develop T2D than overweight or
normal BMI individuals
- Check for family history of diabetes
- Patient's ability to perform ADL/iADL
- Planning
- Actively engage patient to participate in
lowering blood glucose levels
- Prevent or delay T2D complications
- Prevent or eliminate acute hyperglycemic
emergencies or hypoglycemia
- Maintain appropriate blood glucose
levels according to patient profile
- Adjust lifestyle management with minimal stress
- Actively engage patient to participate in
lowering blood glucose levels
- Implementation
- Patient
Education
- Travelling with
diabetes
- Must continue medications as regular
- Must continue medications as regular
- Self-Management
- Consider mentally incompetent
individuals. May require self-management
assistance
- Offer regular diet and preferred food items
- Offer food substitutions if meal intake is
<75%
- Increase blood glucose monitoring during
acute mental status or behaviour changes
- Depression
- Assess and treat depression
- Encourage physical
activity as possible
- Encourage socialization, especially during meals
- Assess and treat depression
- Offer regular diet and preferred food items
- Consider physically incompetent individuals
ranging from the ability to perform ADLs
independently to ADL-dependent
individuals, to successfully apply
self-management skills
- For hospitalized patients who require
temporary self-management assistance
- Monitor BG levels as required based on patient
complexity and avoid relying on A1C levels due to
recent acute illness
- Monitor BG levels as required based on patient
complexity and avoid relying on A1C levels due to
recent acute illness
- For rehab patients who require
partial self-management assistance
- Nursing staff monitor BG levels based on the
patient complexity of T2D and risks of
hypoglycemia. Use caution when
interpreting A1C levels as many conditions
interfere with A1C levels.
- After discharge, patients need to be able to perform
self-care skills and informed about
self-adminstration skills for home management
- After discharge, patients need to be able to perform
self-care skills and informed about
self-adminstration skills for home management
- Nursing staff monitor BG levels based on the
patient complexity of T2D and risks of
hypoglycemia. Use caution when
interpreting A1C levels as many conditions
interfere with A1C levels.
- For chronically ill patients who require full
or partial self-management assistance
- Continuous nursing staff education
to provide T2D management
- Continuous nursing staff education
to provide T2D management
- For community-dwelling patients who require no
self-management assistance (are fully independent)
- Educate the patient in preventing Type 2 diabetes
complications and maintaining BG levels within
normal ranges
- Educate the patient in preventing Type 2 diabetes
complications and maintaining BG levels within
normal ranges
- For hospitalized patients who require
temporary self-management assistance
- Consider mentally incompetent
individuals. May require self-management
assistance
- Plate Method
- Travelling with
diabetes
- Prevent or delay T2D and its
complications
- Encourage physical activity to
minimize the T2D effects of
overweight and obese individuals
- For overweight adults 45 YO and up, provide
routine screening to monitor prognosis
- Encourage physical activity to
minimize the T2D effects of
overweight and obese individuals
- For a Diagnosed T2 Diabetic
- Inform patients of the risks of
poor blood glucose control
- Advise healthy eating habits and nutrition levels and
help develop appropriate plate portions and meal
plans following Canada's Food Guide
- Continue oral agents and
insulin therapy as prescribed
- Track daily basal rates and
bolus doses to review
progression
- Monitor BG levels according
to patient complexity of
regimen
- Monitor BG levels according
to patient complexity of
regimen
- Track daily basal rates and
bolus doses to review
progression
- Continue oral agents and
insulin therapy as prescribed
- Advise healthy eating habits and nutrition levels and
help develop appropriate plate portions and meal
plans following Canada's Food Guide
- Inform patients of the risks of
poor blood glucose control
- Emotional Care
- Patient
Education
- Evaluation
- Review diet progression and connect
with overall health benefits
- Follow-up with patient after
discharge and evaluate outcomes
of patient goals and treatments
- A study showed that when nursing staff are actively involved in
patient therapy after discharge, including initial individual
meeting with an RN, attending a group class meeting for 1 to 2 h
(with 4-10 participants) once per week for 4 weeks, and
telephone follow-up calls for 1 year, resulted in greater mean
change in A1C and total cholesterol and LDL cholesterol
- A study showed that when nursing staff are actively involved in
patient therapy after discharge, including initial individual
meeting with an RN, attending a group class meeting for 1 to 2 h
(with 4-10 participants) once per week for 4 weeks, and
telephone follow-up calls for 1 year, resulted in greater mean
change in A1C and total cholesterol and LDL cholesterol
- If diet has improved or if physical
activity has improved, the risks of
CVD would normally decrease
- Follow-up with patient after
discharge and evaluate outcomes
of patient goals and treatments
- Check if there are any issues with blood
glucose control. If it is poorly controlled, then...
- Check for the absence of
injuries
- Review diet progression and connect
with overall health benefits
- Assessment
- Collaborative Care
- Dietitian
- Works with the patient, RN and the
patient's health care team to develop a
meal plan, appropriate plating portion,
and guidelines to healthy eating habits -
get ready for the yummy fruits and
veggies!
- Works with the patient, RN and the
patient's health care team to develop a
meal plan, appropriate plating portion,
and guidelines to healthy eating habits -
get ready for the yummy fruits and
veggies!
- Chiropodist
- Foot care specialist
who is trained to
trim the toe nails of a
diabetic patient's
foot - I promise he
won't bite!
- Foot care specialist
who is trained to
trim the toe nails of a
diabetic patient's
foot - I promise he
won't bite!
- Diabetes Nurse Educator
- An RN with specialized training and education
in teaching self-management goals, skills, and
diabetic complications unique to each individual
- Arranges Diabetes Education Programs
for patients interested in receiving
support for diabetes management
- An RN with specialized training and education
in teaching self-management goals, skills, and
diabetic complications unique to each individual
- Pharmacist
- Provides more information
on medications and their
interactions
- Provides more information
on medications and their
interactions
- Optometrist
- Uses various vision
tests to check for
and determine
retinal blood vessel
damage
- Uses various vision
tests to check for
and determine
retinal blood vessel
damage
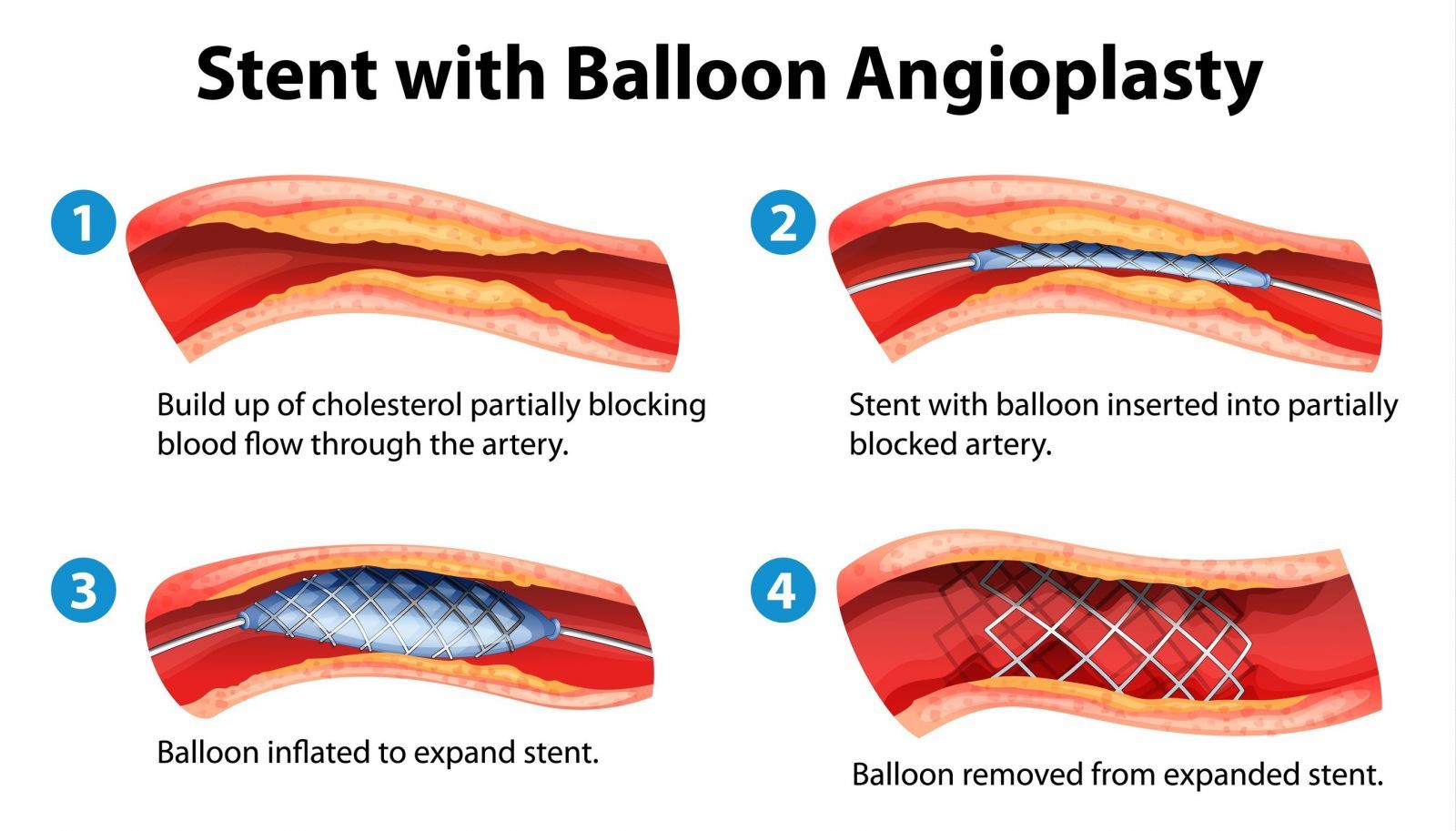
- Cardiologist and Cardiac
Rehabilitation
- Angioplasty or CABG procedures
performed to restore heart function
- Cardiac Rehab provides counseling and
training on exercise, education for
heart-healthy living and stress management
therapies
- Angioplasty or CABG procedures
performed to restore heart function
- Nephrologist
- Community Organizations
- Raises awareness and health promotion strategies to
prevent or delay T2D and associating complications
such as providing support and services leading to
improved self-management goals and skills
- Raises awareness and health promotion strategies to
prevent or delay T2D and associating complications
such as providing support and services leading to
improved self-management goals and skills
- Dietitian
- Pathophysiology
- Who could this affect?
- Over 35 years of age
- Risk increases with age
- Risk increases with age
- Family history
- 80%-90% of patients
are overweight
- Due to increase intake of food, insulin is
constantly being produced
- Insulin receptors on cells become desensitized to
insulin
- Insulin receptors on cells become desensitized to
insulin
- Due to increase intake of food, insulin is
constantly being produced
- Aboriginal
Hispanic
South Asian
Asian
African
- Has higher risk
- Has higher risk
- Over 35 years of age
- What is Diabetes Mellitus Type 2?
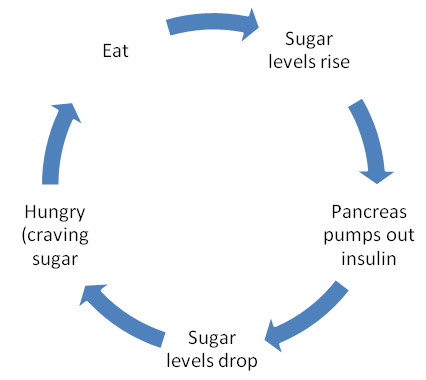
- The body normally goes through the following
cycle to maintain 4 to 6 mmol/L of glucose
- When you eat food, glucose begins building up in the blood
- Beta cells on Islets of Langerhans on
the pancreas secrete insulin
- Insulin "unlocks" receptors on cells
- This step in the cycle is the main
problem for patients with type 2
diabetes
- Insulin Resistance
- Insulin receptors on cells do not get
"unlocked" by insulin due to receptors
being unresponsive or loss of receptors
entirely
- Glucose begins to build up in the
bloodstream
- Results in hyperglycemia
and Type 2 Diabetes
- Results in hyperglycemia
and Type 2 Diabetes
- Analogy: When you put on glasses for the first time, you become very aware that they're on your nose and ears. But over
time, those sensations begin to dim until you forget that the glasses are even on your nose!
- Glucose begins to build up in the
bloodstream
- Insulin receptors on cells do not get
"unlocked" by insulin due to receptors
being unresponsive or loss of receptors
entirely
- Insulin Resistance
- Cells receive glucose to use for
energy
- Lowers blood glucose levels
as the glucose passes out of
the bloodstream
- Alpha cells on liver secrete
glucagon
- Abnormal glucose production
from liver could aid in
development of type 2
diabetes
- Promotes conversion of glycogen to
glucose
- Abnormal glucose production
from liver could aid in
development of type 2
diabetes
- Alpha cells on liver secrete
glucagon
- Lowers blood glucose levels
as the glucose passes out of
the bloodstream
- This step in the cycle is the main
problem for patients with type 2
diabetes
- Pancreas still makes insulin, but could
produce less because of fatigue
- Beta-cell mass loss
- Beta-cell mass loss
- Insulin "unlocks" receptors on cells
- Beta cells on Islets of Langerhans on
the pancreas secrete insulin
- Analogy: This is just one of the components of the homeostatic elements that our body goes through. It
very much works like a thermometer. It detects levels of glucose in the environment, and releases
elements to counteract them if they become to rampant.
- When you eat food, glucose begins building up in the blood
- The body normally goes through the following
cycle to maintain 4 to 6 mmol/L of glucose
- Who could this affect?
- Complications
- Hyperosmolar Hyperglycemic
Syndrome
- BG levels rise immensely and
leads to severe dehydration
and very dark urine
- BG levels rise immensely and
leads to severe dehydration
and very dark urine
- Hypoglycemia
- Happens when there's too much
glucose compared to insulin
- Tremors
Hunger
Excessive
Sweating
- Tremors
Hunger
Excessive
Sweating
- Happens when there's too much
glucose compared to insulin
- Macrovascular
Angiopathy
- increased risk of heart diseases such as CAD and ACS
which can lead to increased risk of mortality
- increased risk of heart diseases such as CAD and ACS
which can lead to increased risk of mortality
- Microvascular
Angiopathy
- Diabetic Retinopathy
- Retinal blood vessels are damaged and can cause
impaired vision and/or blindness
- Retinal blood vessels are damaged and can cause
impaired vision and/or blindness
- Diabetic Nephropathy
- Glomerular arterioles
damaged and increases
the risk of kidney disease
and excretion of proteins
in urine
- Glomerular arterioles
damaged and increases
the risk of kidney disease
and excretion of proteins
in urine
- Diabetic Retinopathy
- Diabetic Neuropathy
- Peripheral nerves damaged and
increases susceptibility to injuries
without being aware of it
- Peripheral nerves damaged and
increases susceptibility to injuries
without being aware of it
- Foot and lower extremity
- Gangrene
- Gangrene
- Skin complications
- Decreased blood circulation lead to
changes in collagen, changing
appearance
- Decreased blood circulation lead to
changes in collagen, changing
appearance
- Infection
- Hyperosmolar Hyperglycemic
Syndrome
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.