11952890
Beschreibung
Karteikarten von Laura Gennaro , aktualisiert more than 1 year ago
|
|
Erstellt von Laura Gennaro
vor fast 7 Jahre
|
|
| Frage | Antworten |
| Idiopathic Osteosclerosis (Enostosis, dense bone island) | -Asymptomatic focus of increased bone production -Considered a variation of normal -Tend to arise in 1st-2nd decade -May remain static or enlarge until skeletal maturity -Seen in tooth, or non-tooth bearing areas of the jaws -Associated dentition vital -Diagnosed clinically/radiographically w/ sequential radiographs as needed -Root resorption seen rarely |
| Reported prevelance of idiopathic osteosclerosis | 5-10% |
| Condensing/sclerosing osteitis | -Identical radiographic appearance to idiopathic osteosclerosis -Seen exclusively at apex of non-vital tooth -represents reactive bone formation in response to pulpal/periapical inflammation |
| Cherubism | painless, self-limiting disorder characterized by: -symmetric, bilateral expansion of the mandible (& maxilla) -bone is replaced by fibro-osseous tissue w/ giant cells -swollen, rounded cheeks -interference of normal tooth eruption; impacted teeth -gnathic expansion causes downward stretching of the skin, exposing the white sclera beneath the iris -jaw enlargement continues throughout childhood; stabilizes during puberty and changes regress by early adulthood as normal bone remodeling occurs |
| Hypophosphatasia | -rare metabolic bone disease characterized by ALPL mutations -alkaline phosphatase levels in serum and bone low -low enzyme levels results in impaired bone mineralization -variable disease severity >>perinatal lethal >>infantile (50% die) >>adult (mild phenotype) >>odontophosphatasia |
| Odontophosphatasia | -premature exfoliation of incisors only sign of disease -most mild presentation of disease |
| Clinical features of hypophosphatasia | -osteomalacia (bone pain/tenderness; fractures) -Periodontal disease -Premature exfoliation of dentition (cementum does not form, PDL non-functional) |
|
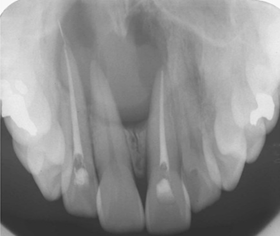
Nasopalatine duct cyst (incisive canal cyst)
Image:
Image (binary/octet-stream)
|
-Most common non-odontogenic cyst of the gnathic bones -most common in 4th-5th decade -Symmetric radiolucency between vital maxillary central incisors >>may appear heart-shaped due to superimposition of the Ant. nasal spine >>may cause root divergence |
| Paired incisive canals open into a single incisive foramen & transmit... | -nasopalatine nerve (innervates palatal mucosa of incisors) -terminal end of greater palatine artery (supplies nasal cavity) -degenerated remnants of nasopalatine duct |
| Nasopalatine duct cyst arieses from... | -epithelial rests of degenerated nasopalatine duct |
| Nasaopalatine duct cyst differential diagnosis | -radicular cyst/granuloma -keratocystic odontogenic tumor -large incisive foramen |
| Nasopalatine duct cyst management | -conservative surgical removal -recurrence rare |
| Cyst of the incisive papilla | -soft tissue counterpart of nasopalatine duct cyst (very rare, no radiograph abnormalities) -Arises from remnants of nasopalatine duct located within the incisive papilla -conservative removal, recurrence rare |
| Surgical ciliated cyst | -uncommon consequence of surgical entry into maxillary sinus -sinus epithelium iatrogenically implanted in bone by surgeon (pseudostratified ciliated respiratory epithelium) -posterior maxilla most common site -conservative removal (recurrence rare) |
|
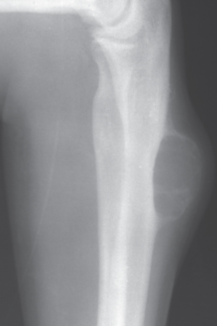
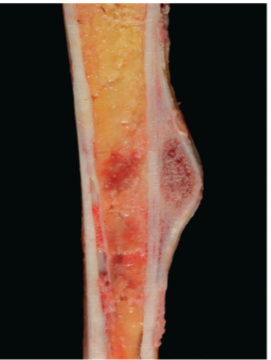
Simple bone cyst (traumatic bone cyst, idiopathic bone cavity)
Image:
Image (binary/octet-stream)
|
-Hollow cavity within bone -Etiology unknown -Treated by vigorous curettage of cavity walls (induces bleeding, wound healing) -20% recurrence rate |
| Epidemiology of Simple bone cysts | -Metaphysis of humerus or femur most common location -2:1 male predilection -Most common in 1st-2nd decade |
| Gnathic Simple Bone Cyst | -75% occur in posterior mandible, typically unilocular -asymptomatic, associated teeth are vital -Scalloping between roots characteristic but not universal -Rarely bilateral |
| Differential diagnosis of Gnathic simple bone cyst | -Keratocystic odontogenic tumor (both have tendency to scallop around roots of teeth) |
| Central Giant Cell Granuloma (CGCG) | -Likely neoplastic lesion exclusive to gnathic bones -associated w/ PDL of teeth -75% of cases are unilocular/multilocular radiolucency of the mandible (anterior or body most common) -Most common in 1st-3rd decades -Female predilection |
| Aggressive CGCGs characterized by... | -pain -paresthesia -size >5cm -root resorption -rapid growth -cortical perforation -recurrence |
| Management & Prognosis of CGCG | -surgical excision w/ vigorous curettage -variable recurrence rate (depending on biologic potential of lesion) |
| Recurrent CGCG lesions | -En bloc resection -intralesional injection (steroid, denosumab, IFN-alpha) |
|
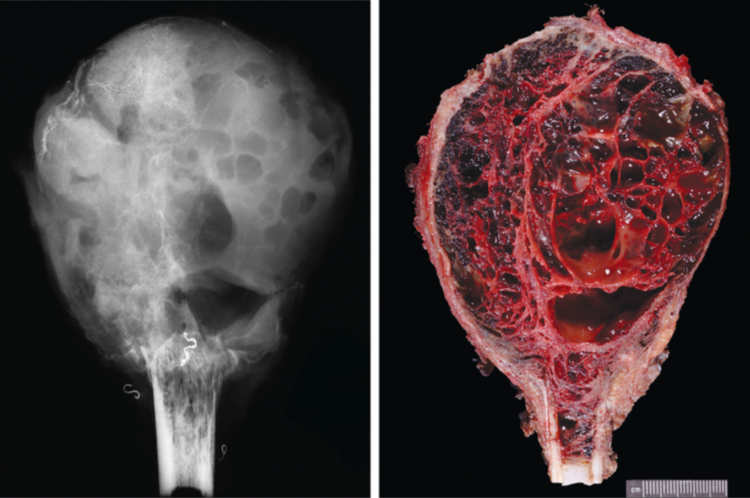
Aneurysmal bone cyst
Image:
Image (binary/octet-stream)
|
-benign neoplasm characterized by recurrent USP6 abnormalities
-Aneurysmal= referring to blowout distension of contour of affected bone
-Cyst= consists primarily of blood-filled (cyst-like) cavities
Image:
Image (binary/octet-stream)
|
| Epidemiology of Aneurysmal Bone Cyst (ABC) | -80% occur in 1st-2nd decade -20% occur in craniofacial bones -Approx. 50% of ABCs occur secondary to a pre-existing lesion (osteoblatoma, CGCGs, fibrous dysplasia, osteosarcoma in craniofacial bones) |
|
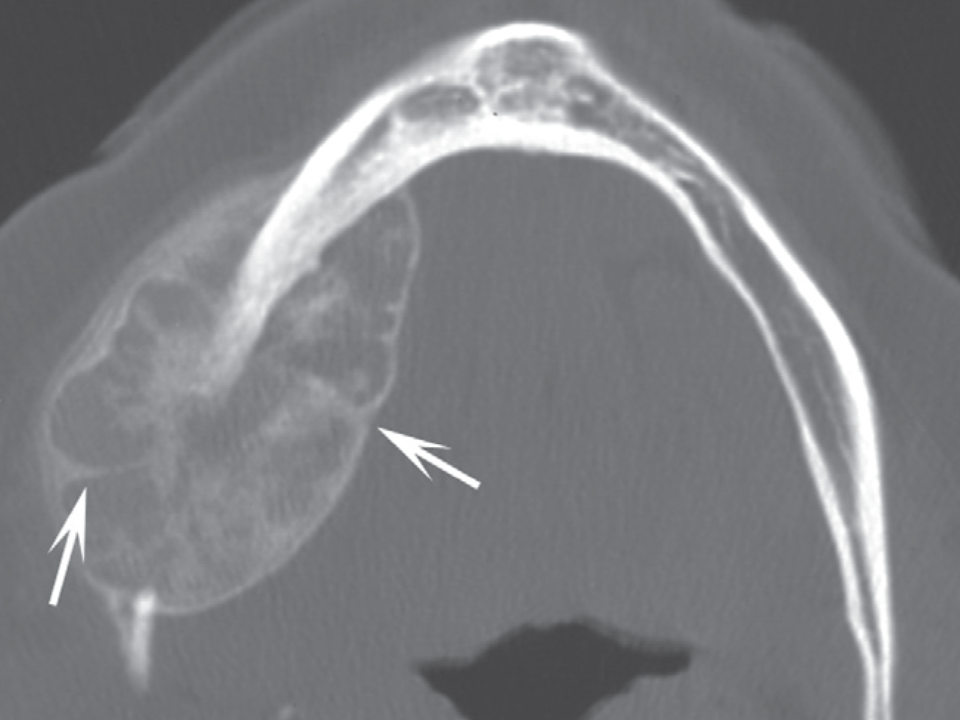
Gnathic ABC
Image:
Image (binary/octet-stream)
|
-most commonly occur in posterior mandible -multilocular, eccentric radiolucency with paper-thin shell of subperiostea bone -rapid growth, tooth displacement, root resorption common -patient may complain of pain, tenderness -finger in balloon sign |
| ABC clinical differential diagnosis Management & Prognosis | -CGCG -Aggressive curettage w/ bone grafting (high recurrence rate (20-70%)) -En bloc resection (most effective treatment; may require significant reconstruction) |
| Hematopoietic bone marrow defect | -focus of hyperplastic hematopoietic marrow -considered a variation of normal -no reported cases outside of gnathic bones -no treatment required -biopsy usually necessary for diagnosis -Post. mandible most common site -well-demarcated or diffuse radiolucency -may or may not be corticated -asymptomatic |
| Myospherulosis | -increasingly uncommon iatrogenically caused condition -gauze impregnated w/ petrolatum/antibiotics placed following: >>dental extractions >>surgical procedures involving paranasal sinuses >>subcutaneous intramuscular injections |
| Cause of Myospherulosis Presentation Treatment | -lipids in petrolatum or linolatum based antibiotic ointments undergo non-degradable emulsification w/ RBCs -Non-descript radiolucency; usually in the area of a previously extracted tooth -Curettage curative |
| Osteonecrosis (avascular necrosis) | -infarction of bone & marrow -associated w/ a variety of conditions: >>fracture >>corticosteroid administration (femoral head common site) >>antiresorptive therapy (bisphosphonates, denosumab; jawbones common site) >>infection, radiation >>sickle cell crisis |
| Medication related osteonecrosis of teh jaws (MRONJ) | -uncommon but serious side effect of certain medications >>bisphosphonates (majority of cases) >>denosumab >>antiangiogenic cancer therapies (rarely) -rarely extragnathic bones involved -mechanism of action incompletely understood |
| What are bisphosphonates? | Inhibitors of osteoclastic bone resorption -attach to hydroxyapatite crystals in bone -ingested by osteoclasts during bone resorption -osteoclasts rendered non-functional -half-life in bone ~10yr |
| When are bisphosphonates administered? | -Cancer therapy (multiple myeloma, metastatic cancer to bone [breast, prostate, lung]; inc. quality of life by decreasing skeletal events) -Osteoporosis/osteopenia (reduced risk of osteoporotic bone fracture) -Any condition w/ excessive bone resorption (osteogenesis imperfecta, Paget disease) |
| IV bisphosphonates every 3-4 weeks for bone metastases (zoledronate/zometa; pamidronate/aredia) | 0.5-1% develop osteonecrosis |
| IV bisphosphonates once yearly for osteoporosis (zoledronate/reclast) | 0.02-0.04% develop osteonecrosis |
| Oral bisphosphonates taken daily/weekly/monthly for osteoporosis (alendronate/fosamax; risedronate/actonel; ibandronate/bonvia) | 0.1-0.2% develop osteonecrosis |
| What is denosumab? | inhibitor of osteoclastic bone resorption -binds RANK ligand so it cannot bind RANK (binding is necessary to continue maturation) -osteoclasts cannot develop from precursor cells -does not bind bone -half-life ~6months |
| When is denosumab administered? | -Osteoporosis/osteopenia (reduce risk of osteoporotic bone fracture) -Cancer therapy (metastatic cancer to bone; increase quality of life by decreasing skeletal-related events) |
| Subcutaneous administration of denosumab every 6months for osteoporosis (Prolia) | 0.5-1% develop osteonecrosis |
| Subcutaneous administration of denosumab every 4 weeks for bone metastases (Xgeva) | 0.02-0.04% develop osteonecrosis |
| MRONJ Risk Factors: site | 73% Mandible 22.5% Maxilla 4.5% Both jaws |
| MRONJ Risk Factors: Duration of dose | -IV= 9-30 months median onset -PO= 4yr median onset |
| MRONJ Risk Factors: Age | -no children have developed ONJ |
| MRONJ: Other risk factors | -Dentoalveolar surgery? -Pre-existing inflammatory dental disease? |
| Diagnosis of MRONJ | 3 diagnostic criteria must be met: 1) Current or previous treatment with anti-resorptive/anti-angiogenic agents 2) Exposed bone or bone that can be probed (intraorally or extraorally) through a fistula (Present for at least 8 weeks) 3No history of radiation therapy to jaws or metastatic disease to jaws |
| Stage 0 MRONJ | No clinical evidence of necrotic bone Non-specific clinical/radiographic symptoms: -Dull/aching bone or sinus pain -Odontalgia, loosening of teeth -Alveolar bone loss, changes in trabecular pattern of bone -Intraoral fistula (does not probe to bone) |
| S | -Exposed necrotic bone or fistula that probes to bone -No evidence of infection -Asymptomatic |
| Stage 2 MRONJ | -Exposed necrotic bone or fistula that probes to bone -Evidence of infection (swelling, erythema) -Typically symptomatic |
| Stage 3 MRONJ | -Exposed necrotic bone or fistula that probes to bone -Evidence of infection (swelling, erythema) -One of the following: >>Extensive exposed bone >>Pathologic fracture >>Extra-oral fistula >>Oro-antral/oro-nasal communication |
| Treatment of MRONJ | -Conservative management of caries, periodontal disease -Close monitoring for progression to higher stage -Mobile bony sequestra should always be removed to facilitate soft tissue healing, when possible -Chlorhexidine 0.12% (antimicrobial mouth rinse) -Oral antibiotics (penicillin best) and/or pain control -Surgical resection, debridement |
| MRONJ & dental considerations | Prior to beginning therapy with anti-resorptives -Optimize dental health If dental work needed during therapy -Wait until 2 months after bisphosphonate administration (lowest levels in serum) -Bisphosphonate ‘drug holiday’ suggested but efficacy unproven If patient has exposed bone -Instruct to gently brush area with toothbrush (so plaque doesn’t build up) |
| Osteoradionecrosis | -Exposed, irradiated bone in the absence of residual or recurrent tumor -Complication of radiotherapy= vascular obliteration leads to tissue hypoxia |
| Osteoradionecrosis of the jaws | -Occurs in 5-7% of locally radiated patients -Mandible involved in >90% of cases (Exposed to high doses of radiation in majority of radiated patients (oropharyngeal cancer, oral cancer) Maxillary osteoradionecrosis rare) |
| Majority of Osteoradionecrosis of the Jaws occur... | -At radiation doses >60Gy -Following dentoalveolar surgery -4-36months after completion of radiation therapy |
| Management of Osteoradionecrosis of the jaws | Complex -Conservative debridement, antibiotics -Resection -Hyperbaric oxygen |
| Prevention represents best course of action (Osteoradionecrosis) | -Extraction of unrestorable teeth -Extraction of teeth w/ advanced periodontitis -Elimination of oral foci of infection -Excellent oral hygiene |
| Spontaneous sequestration (osteonecrosis) | -Occurs nearly exclusively along the mylohyoid ridge (<1cm in diameter) -Etiology unknown -Patient management: >>gently brush area (avoids plaque build-up) >>once mobile, can be removed |
| Other causes of osteonecrosis | -Mechanical trauma -Chemical trauma -Infection -Secondary to disease states causing hypovascular bone |
| Fibrous dysplasia | -anomaly of bone-forming mesenchymal tissue -characterized by inability of bone-forming tissue to produce mature lamellar bone >>Maturation arrested at level of woven bone >>abnormal bone produced in increased amounts |
| Fibrous dysplasia manifestation | -usually during 1st-3rd decades -asymptomatic bony swelling or deformity -mild/moderate pain occasionally -growth typically arrests by early 20s (foci go away entirely on their own once growth is arrested due to normal remodeling) |
| Fibrous dysplasia variable phenotypic expressions Monostotic FD (85-90%) | -one bone involved -craniofacial bones, ribs, femur commonly involved |
| Fibrous dysplasia variable phenotypic expressions Polyostotic FD (10-15%) | -Multiple bones affected -craniofacial involvement in ~50% of cases -Mazabraud syndrome: polyostotic FD w/ soft tissue myxomas |
| Fibrous dysplasia variable phenotypic expressions McCune-Albright Syndrome (<5%) | -Polyostotic FD -Irregular Cafe-au-lait skin pigmentation (coast of Maine borders) -precocious puberty |
| Extent of disease (FD) correlates w | onset of disease-causing GNAS mutation -always post-zygotic (never inherited) -Earlier occuring mutations in osteoblast precursors during embryologic development results in greater proportion of functional osteoblasts w/ GNAS mutation (greater amounts of abnormal bone production) |
| Radiographic appearance of FD |
-normal bone trabeculation characteristically replaced by 'ground glass' appearing bone
-borders often poorly discernable and blend into normal bone
Image:
Image (binary/octet-stream)
|
| Craniofacial fibrous dysplasia | refers to a solitary lesion affecting multiple contiguous craniofacial bones |
| Fibrous dysplasia Diagnosis & Management | -Diagnosed based on clinico-radiologic features (biopsy usually unnecessary) -Management depends on the presence of symptoms: >>Asymptomatic= observation w/ periodic radiographs >>Symptomatic= surgical recontouring (high rate of recurrence until natural cessation of growth of lesion) |
| Cemento-ossifying fibroma | -benign odontogenic neoplasm exclusive to tooth-bearing regions of gnathic bones -most common in 3rd-4th decades -60-70% occur in body of mandible -Typically treated by conservative removal -Rare patients may have hyperparathyroidism-jaw tumor syndrome |
| Cemento-ossifying fibroma Radiographic appearance |
-well-demarcated radiolucency w/ variable radiopacitites
-expansion, root resorption occasionally noted
Image:
Image (binary/octet-stream)
|
| Aggressive (juvenile) ossifying fibromas -Trabecular ossifying fibroma | -mean age range 8.5-12yr -Maxilla/mandible most common sites of occurence (rarely extragnathic craniofacial sites) -Progressive/rapid expansion of affected area |
| Aggressive (juvenile) ossifying fibromas -Psammomatoid ossifying fibroma | -Most common in 2nd-3rd decades -Extragnathic craniofacial sites most commonly involved (rarely gnathic bones) -Progressive/rapid expansion of affected area |
| Gigantiform cementoma |
-very rare
-multifocal development of ossifying fibroma-like lesions
-arises in childhood & progressively expand to cause facial deformity
-familial inheritance in some cases
Image:
Image (binary/octet-stream)
|
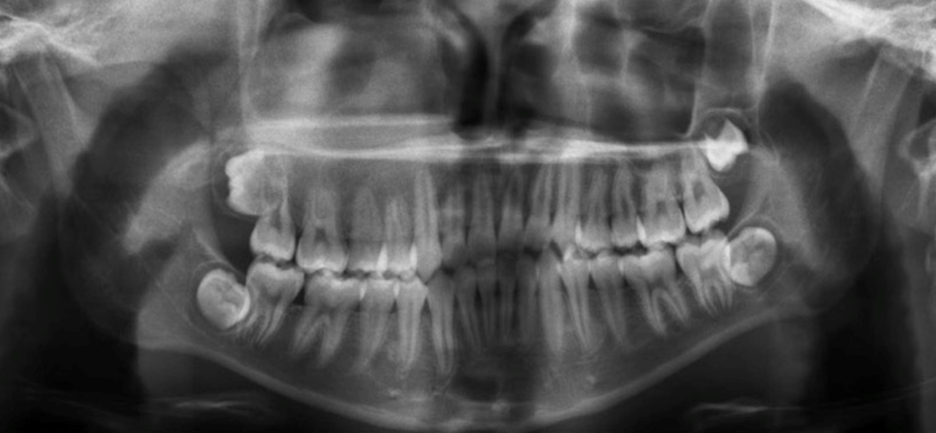
| Cemento-osseous dysplasia | -idiopathic bone condition in which bone is replaced by varying amounts of fibrous tissue and cemento-osseous tissue -unique to tooth-bearing regions of gnathic bones -Most common fibro-osseous lesion encountered -May persist following or develop in response to dental extraction |
| Cemento-osseous dysplasia Takes months/years to develop & radiographic appearance depends on maturity of lesion |
-Early= radiolucent (fibrous tissue)
-Intermediate= mixed radiolucent/radiopaque
-Late= radiopaque (cemnto-osseous tissue)
Image:
Image (binary/octet-stream)
|
| Cemento-osseous dysplasia most frequently occurs in... | African American females in 4th-5th decades -asymptomatic & discovered on routine radiographs -no bony expansion -associated dentition vital |
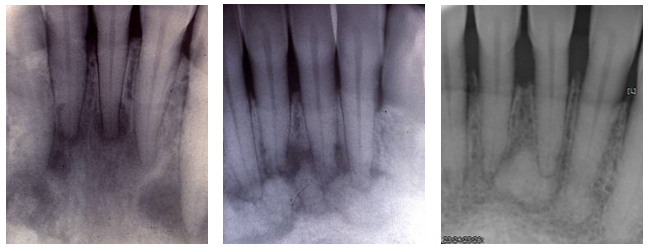
| Periapical COD |
-(most?) common presentation of COD
-affects apices of one or more vital mandibular anterior teeth
Image:
Image (binary/octet-stream)
|
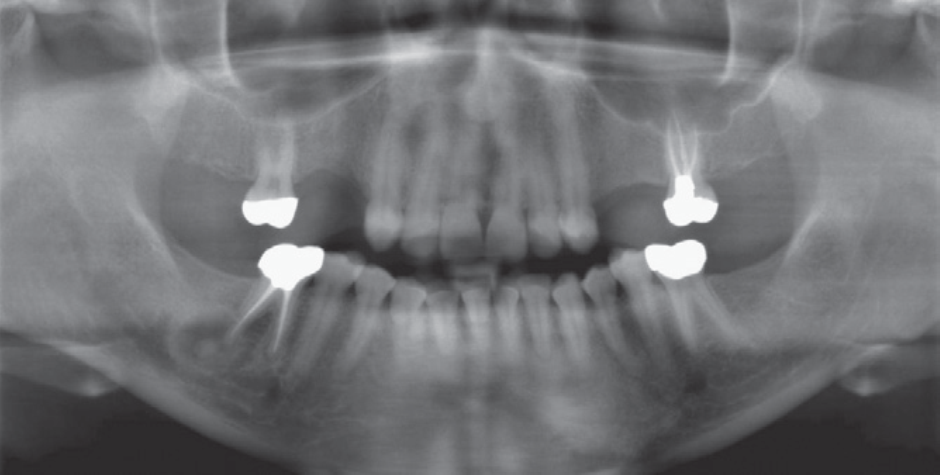
| Focal COD |
COD also known to present unifocally in posterior jaws
Image:
Image (binary/octet-stream)
|
| Multifocal COD |
involving more than one site
Image:
Image (binary/octet-stream)
|
| Florid COD |
Image:
Image (binary/octet-stream)
|
| Management of COD | -Can be diagnosed confidently on panoramic or periapical films (Biopsy not needed; Should be avoided because hypovascular bone prone to infection (osteomyetlitis)) -Do not do a root canal if the teeth are vital!! -Patient can be followed with serial imaging -Osteomyelitis may rarely develop |
| Osteoma | -benign, slow-growing, bone-forming tumor -Limited almost exclusively to craniofacial bones (gnathic bones less commonly) -Most commonly diagnosed in 4th-5th decades -Asymptomatic -Firm, painless expansion |
| Osteoma Diagnosis | -radiographic imaging or biopsy -radiographic appearance of gnathic osteomas resembles that of parosteal osteosarcoma and typically requires biopsy |
| Bones/areas affected by Osteoma | -Paranasal sinuses, cranial vault, nasal cavity, orbit -Inferior or lingual border of mandible -Condylar or coronoid regions |
| Osteoid osteoma & osteoblastoma | -Microscopically identical neoplasms with predilection for 1st-3rd decades -May appear radiolucent, radiopaque, or mixed depending on amount of osteoid is produced |
| Osteoid Osteoma | -Less than 1.5-2 cm in diameter -50% of cases involve femur or tibia -Presents with tenderness, severe nocturnal pain relieved by aspirin -10-12% of all bone tumors (Uncommon in gnathic bones) -Treated by surgical resection -Recurrences uncommon |
| Osteoblastoma | -Larger than 1.5-2 cm in diameter -Frequently involves vertebral column -Pain not distinctly nocturnal and unresponsive to aspirin -Less than 1% of bone tumors -Common in craniofacial bones -Treated by surgical resection -25% recurrence rate |
| Osteosarcoma | -malignant neoplasm of bone -most common primary bone malignancy -second most common malignancy to metastases -75% occur in 1st-2nd decades of life -Usually arises in long bones of extremities (50% in area of knee; 6-10% occur in craniofacial bones) -Typically presents as painful, progressively enlarging masses; pathologic fracture may be first symptom |
| Osteosarcoma survival | -Historically 85-90% of patients developed metastases and died of disease -Most patients have subclinical metastatic disease at time of surgery -Introduction of neoadjuvant chemotherapy has markedly improved & predicted survival >>Responders (>90% tumor necrosis)= long-term survival in 90% of cases >>Non-responders= 5yr survival rate of <15% |
| Osteosarcoma of Gnathic bones | -tends to affect skeletally mature patients (3rd-5th decades most common) -local pain/paresthesia & swelling most consistent complaints -Local recurrence most important reason for therapeutic failure -metastases occur in 30% of patients (average survival rate <1yr) |
| What percent of mandibular and maxillary osteosarcomas recur | -50% of mandibular osteosarcomas -80% of maxillary osteosarcomas |
| Radiographic appearance of Gnathic Osteosarcoma |
-radiolucent, radiopaque, or mixed depending on ratio of bone destruction/formation
-widening of PDL, loosening of teeth, and supracrestal bone formation may all be seen
Image:
Image (binary/octet-stream)
|
| Osteosarcoma, Codman triangle, & 'sunburst' appearance |
-when breaking through the cortex, lifts off normal periosteum, inducing reactive bone formation
Image:
Image (binary/octet-stream)
|
| Surface osteosarcomas | -most osteosarcomas arise within medullary cavity of bone; some originate in periosteal or cortical region w/ little to no medullary involvement |
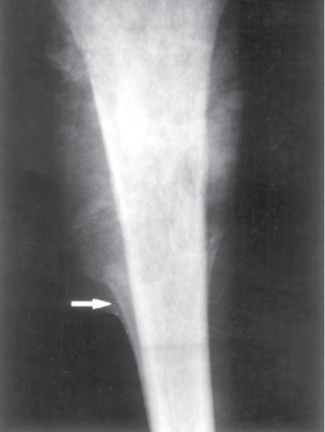
| Periosteal osteosarcoma |
-better prognosis than conventional osteosarcoma
Image:
Image (binary/octet-stream)
|
| Parosteal osteosarcoma |
-excellent prognosis
Image:
Image (binary/octet-stream)
|
| Chondrosarcoma | -Malignant neoplasm of cartilage -Peak incidence after 5th decade of life -<10% occur in craniofacial bones -local pain/paresthesia & swelling most consistent complaints |
| Chondrosarcoma statistics | -3rd most common primary bone malignancy following osteosarcoma & multiple myeloma -Approx. 1/2 as common as osteosarcoma -90% are low/intermediate grade tumors (grade I & II) -10% are high-grade (grade III, other rare variants) |
| Chondrosarcoma Precursor lesions | -Osteochondroma, enchondroma (<1%) -Ollier disease, Mafucci syndrome |
| Low/intermediate grade Chondrosarcoma | -Slow growing w/ low metastatic potential -Relatively refractory to chemotherapy, radiation -Treated by surgical resection |
| High-grade chondrosarcoma | -high metastatic potential -surgical resection remains best chance for cure but some indications for chemotherapy, radiation |
| Mesenchymal chondrosarcoma | -<5% of all chondrosarcomas -gnathic bones most common site of involvement -significant minority occur extraskeletally -Most common in 2nd-3rd decades -Aggressive= 10yr overall survival ranges from 10-54% |
| Metastases to gnathic bones | -comprise 1% of all oral/maxillofacial malignancies -gnathic bones & mouth uncommon sites -Gnathic bones 2x as commonly involved as oral soft tissues -Typically evidence of widespread disease -Average survival rate 7months -First evidence of disease in up to 25% of patients -Local pain/paresthesia & swelling most consistent complaints -Bon preferred site of metastasis of several neoplasms (breast, prostate, thyroid, kidney, lungs) |
| Radiographic appearance of metastatic disease | -poorly circumscribed radiolucency most common appearance -breast and prostate cancer may appear radiopaque |
| Synovial Chondromatosis | -benign disorder (likely neoplastic) or synovium -Nodules of cartilage produced from synovial membrane >>become detached from synovial membrane, float in the joint; may ossify -Self-limiting or indolent course -Rarely may transform to synovial chondrosarcoma |
| Synoviuim | specialized connective tissue which maintains synovial fluid within synovial cavity of synovial joints |
| Treatment of Synovial chondromatosis | -surgical removal of loose bodies & synovial membrane as needed |
| Synovial Chondromatosis characteristics | -typically monoarticular -affects majority weight-bearing joints -TMJ uncommonly affected -Pain, swelling, or limitation of function -Male predilection -TMJ involvement present with non-specific signs and symptoms (pain, swelling, restricted movement, clicking/popping, crepitus, malocclusion) |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.