3326263
Beschreibung

Karteikarten von Jonathan O'Keeffe, aktualisiert more than 1 year ago
|
|
Erstellt von Jonathan O'Keeffe
vor etwa 9 Jahre
|
|
| Frage | Antworten |
| 1. List the main causes of chronic liver disease | 1. Alcohol 2. Viral hepatitis 3. Autoimmune hepatitis 4. Primary biliary cirrhosis |
| 2. What investigations would you initiate to investigate the underlying cause of chronic liver disease? | Viral and autoimmune hepatitis screen Metabolic screen(ceruloplasmin, ferritin, alpha-1 antitrypsin) AFP (hepaocellular carcinoma) liver US and biopsy. |
| 3. Which three things suggest decompensated liver function? | 1. Jaundice 2. Ascites 3. Encephalopathy (asterixis) |
| 4. Up to how many spider naevi can be considered normal on examination of a patient? | 4 |
| 5 List the main stigmata of chronic liver disease | Spider angioma (naevi) Jaundice Scleral icterus Palmar erythema Gynecomastia Encephalopathy Asterixis (liver flap) |
| 6. What are the main feature of decompensated pulmonary fibrosis? | Cor pulmonale central cyanosis (Hypercapnic flap?) |
| 7. What are the main causes of pulmonary fibrosis? | Idiopathic (70%) Connective tissue disease (RA, SLE) Extrinsic Allergic Aveolitis Industrial lung disease (asbestosis, silicosis) Drugs (methotrexate, amiodarone) |
| 8. What Ix would you initiate for pulmonary fibrosis? | FBC (incl ESR due to CTD) ABG (Type 1 failure) CXR (reduce lung vol, diffuse reticular nodular shadowing + honeycombing in severe disease) High res CT |
| 9. Main points to elicit in the Hx of a Bell's palsy? | Onset sudden or over several hours? Severe pain at Sx onset? (RHS/bad prognosis) Signs of stroke? (arm or leg weakness) Any blisters in mouth/tongue? Tinnitus, hearing loss or vertigo (vestibulocochlear involvement) |
| 10. What would you examine to assess a Bell's palsy? | CN 5, 7 (excluding Glabellar sparing) and 8 nb. The corneal reflex is often absent. The ears and oral cavity looking for herpetic rashes (RHS). |
| 11. What would your Mx plan for a Bell's palsy consist of? | 1. Steroids in the acute phase 2. Slit lamp eye exam (corneal ulcers) 3. Otoscopic ear exam. |
| 12. What are the functions of the facial nerve? | -Blinking and closing the eyes, smiling, frowning, flaring nostrils and raising eyebrows. -Lacrimation and salivation. -Taste in the anterior two-thirds of the tongue, via the chorda tympani nerve. -Innervates the stapedius muscle of the inner ear (via tympanic branch) |
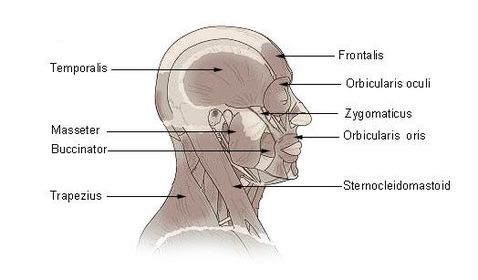
| 13What are the muscles of mastication and what is their innervation? | The masseter, temporals, medial pterygoid, and lateral pterygoid are innervated by the 3rd (mandibular) branch of the trigeminal nerve |
| 14. Which nerve mediates both the efferent and afferent limb of the jaw jerk? | The trigeminal nerve |
| 15. The combination of pes caves, muscle wasting, a high stepping gait and a predominantly motor peripheral neuropathy is characteristic of which condition? | Charcot-Marie-Tooth (aka Hereditary Sensory Motor Neuropathy and Peroneal Muscular Atrophy. Axonal and demyelinating forms can be differentiated by EP. |
| 16. What investigations would you request to investigate episodes of collapse of a presumed cardiac origin? | FBC(?anaemia) U&E(?arrhythmia) TFT ECG + 24 hour tape Echocardiogram Tilt test |
| 17. After valvular replacement surgery how should a patient ideally be followed up? | In the short term, post op, est. that the prosthetic valve is well seated, not sig regurgitant, and no para-prosthetic leak. Once est. long term FU should is usually an annual echo. |
| 18. How do you assess the risk of a prosthetic valve developing thrombus? | Tissue valves carry low risk and usually require only anti-platelets. Both aortic and mitral metallic valves are at thrombus risk, mitral>aortic, due to lower trans-mitral velocities and associated AF and require anti-coagulation with wafarin. |
| 19. What are the indications for urgent aortic valve replacement? | 1. Symptomatology: incl. new onset angina, dyspnoea or syncope. 2. Using reg echos: precipitous change in LV size or function. |
| 20. What are the characteristic features of psoriasis on examination? | Well circumscribed erythematous silvery scaly plaques Nail changes(pitting and onycholysis) Assymetric joint involvement (esp. DIPJs) |
| 21. What are the management options for psoriatic arthropathy? | Physio OT simple analgesia/NSAIDS In severe cases: methotrexate or other systemic Tx (nb.systemic steroids may cause a flare on withdrawal) |
| 22. What is the most usual indication for thoracoplasty? | Old TB |
| 23. What are the causes of bronchiectasis? | Childhood infection (e.g. measles) Obstruction (tumour, nodes, FB) CF Hypogammaglobulinaemia Kartagener's Syndrome |
| 24. What would bronchiectasis show on spirometry? | Obstructive pattern (type IV) red FVC and FEV1 FEV1/FVC <0.7 |
| 25. What is the differential for a ejection cardiac murmur? | Aortic stenosis Aortic sclerosis (?doesn't radiate) HCM (Hokum) Pulmonary valve stenosis VSD Tetralogy of Fallot |
| 26. What is the differential for a regurgitant systolic cardiac murmur? | Mitral regurg Tricuspid regurg VSD (a. Roger's type 1 (with pulm HTN) and 2 (wo pull HTN) b. slitlike) |
| 27. What are indications for thoracoplasty? | Cavitary TB Empyema Bronchopleural fistula Persistent spaces following pulmonary resection |
| 28. What are the three classical signs of Parkinson's disease? | Tremor Rigidity Hypokinesia |
| 29. What are the classical features of cerebellar syndrome? | Dysdiadochokinesia Ataxia Nystagmus Intention tremor Slurring Hypotonia |
| 30. What is the DDx for expyramidal Sx? | Parkinson's PSP MSA Normal pressure hydrocephalus |
| 31. What is the differential for hepatomegaly | HEPATIC Heamatological (CLL, haemochromatosis) Ethanol (ASH and NASH) PSC, PBC, Portal HTN Autoimmune or vial hepatitis Tumour Infiltration (Wilson's, sarcoid, amyloid, ) Cardiac (CCF, pericarditis) |
| 32. What are the causes of Parkinsonian syndrome? | Idiopathic Drugs -(phenothiazides, metoclopramide, haloperidol, reserpine) Postencephalitis Cerebral tumours (involving the BG) |
| 33. What are the complications of Parkinson's disease? | Dysphagia Constipation Recurrent falls Postural hypotension Memory loss Depression |
| 34. What is the most common organism causing exacerbvation of bronchiectasis? | pseudomonas |
| 35. What complications of liver cirrhosis do you know? | Ascites Coagulopathy Portal HTN Encephalopathy |
| 36. What might precipitate encephalopathy? | GI bleed Infection Constipation Increased protein intake Renal failure Electrolyte imbalance Drugs (benzos, opiates) |
| 37. How would you Mx a Pt with encephalopathy? | Tx precipitating cause Give lactulose (to decrease ammonia) Correct hypokalaemia Involve liver team |
| 38. What are the clinical signs of coarctation of the aorta? | HTN Radiofemoral delay Absent femoral pulses Mid-systolic or cont murmur Subscapular bruit Rib notching (figure of 3 on CXR) Post-stenotic dilatation of aorta (CXR) |
| 39. What at the signs of a third nerve palsy? | Eye is deviated downwards and outwards Ptosis Pupil dilatation (Surgical -parasymp damage) No pupil dilatation(medical-no parasymp damage) |
| 40. What are common causes of a medical third nerve palsy? | Mononeuritis multiplex (eg. DMII) MS Midbrain infarction Migraine |
| 41. What are common causes of a surgical third nerve palsy? | Cavernous sinus pathology PCA aneurysm (classically painful) |
| 42. What are the contents of the cavernous sinus? | O TOM CAT Oculomotor nerve Trochlear nerver Ophthalmic div of 5th Maxillary div of 5th Carotid (internal) Abducens nerve Trochlear nerve |
| 43. What are the typical clinical signs in COPD? | Tar stains CO2 flap and bounding pulse Central cyanosis Pursed lips (prolonged expiratory phase) Use of accessory muscles Hyper-expanded chest Crackles if infection present |
| 44. What are the signs of cor pulmonale? | Loud P2 Rt ventricular heave Raised JVP Peripheral oedema |
| 45. What is COPD? | COPD is a spirometric diagnosis characterised by airflow obstruction which is not fully reversible. It comprises chronic bronchitis with emphysema. FEV1/FVC<0.7 |
| 46. How would you investigate a possible new diagnosis of COPD seen in clinic? | Spirometry after bronchodilators CXR (hyperinflation or other causes of SOB) FBC (polycythaemia or anaemia) ABG (type II resp failure) ECG (Rt heart failure) Anti-trypsin deficiency (in a young person) |
| 47. What Tx would you offer a stable COPD Pt seen in clinic? | Smoking cessation clinic 'Reliever' inhaler (e.g. salbutamol) 'Preventor' inhaler (eg. salmeterol or seretide ie. salmeterol + fluticasone) Aminophylline IV/PO |
| 48. What features of a patient's presentation with COPD would suggest LTOT should be considered? | FEV1<0.3 of predicted Peripheral oedema raised JVP cyanosis polycythaemia Sats<92% on RA |
| 49. What are the criteria for LTOT? | 2 ABGs 3 weeks apart where stable & PaO2<7.3 or 7.3<PaO2<8 + 1 or more of 1. Nocturnal hypoxia 2. Pulmonary HTN 3. Peripheral oedema 4. Secondary polycythaemia |
| 50. How long does LTOT need to be used for? | At least 15 hours per day |
| 51. Are there any risks associated with aminophylline? | Aminophylline has a fairly narrow therapeutic window. Toxicity: nausea, vomiting, diarrhoea, agitation, dilated pupils. Severe toxicity: arrhythmias and convulsions. Can also cause hypokalaemia. |
| 52. What dosing regime would you use for aminophylline? | 5mg/kg loading over 30mins. Then: Infusion of 0.5mk/kg/hour. Check levels at 24 hours and daily thereafter. |
| 53. How would you manage an exacerbation of COPD? | Controlled O2 through a venturi mask Salbutamol and ipratropium nebs Oral pred IV aminophylline if poor response to above. If infective give ABx NIV if required. |
| 54. How and why would you initiate NIV? | If after 1 hour of medical Mx the Pt is still acidotic and in type II respiratory failure, then NIV should be considered. (initially IPAP = 10, PEEP=5 and titrate IPAP us as per ABGs) |
| 55. What is alpha-1 antitrypsin deficiency? | Alpha-1 antitrypsin is a protease inhibitor produced by the liver. In the lungs this protects alveolar tissue from damage by neutrophil elastase. Deficiency makes COPD likely in the 3rd or 4th decade in a smoker. Classic pattern: pan lobar emphysema in lower lobes. |
| 56. How do you categorise haematological causes of hepatosplenomegaly? | With anaemia: myeloproliferative or lymphoproliferative disorders With lymph nodes: CLL or lymphoma |
| 57. How would you CONFIRM a diagnosis of liver cirrhosis? | Liver US may be suggestive, but a liver biopsy is required for definitive diagnosis. |
| 58. What is the Child Pughs score used for? | 59. Prognosis in liver cirrhosis (i.e. predicting 1 and 2 year survival) |
| 60. What features contribute to the Child Pughs score? | Bilirubin Serum albumin INR Ascites Hepatic encephalopathy |
| 61. What is the purpose of the Rockall score? | To identify patients at risk of an adverse outcome following an acute GI bleed. |
| 62. What factors contribute to the Rockall score? | Age Shock Co-morbidity Diagnosis Evidence of bleeding on endoscopy (score<3 = good prognosis, but >8 = high risk) |
| 63. What might the examination findings be in a patient with a renal transplant? | |
| 64. What are the causes of hepatosplenomegaly? | 1-Infection: Acute viral hepatitis, Infectious mononucleosis, Cytomegalovirus 2-Haem: Myelo- (CML ,Myelofibrosis) and lympho-(CLL, Hodgkin's Lymphoma) proliferative disease. Anaemia:Pernicious anaemia, Sickle cell anaemia, Thalassaemia 3-Chronic liver disease and portal hypertension: Chronic active hepatitis 4-Amyloidosis 5-Acromegaly 6-Systemic lupus erythematosus |
| 65. What is your differential for splenomegaly? | CHINA Congestion - portal HTN Heam (Haemolytic anaemia, SSD, hereditary spherocytosis) Infection (Malaria, EBV, CMV, HIV) Neoplastic (CLL, Myelofibrosis, lymphoma) Autoimmune (sarcoid, amyloid, RA) |
| 66. What are the causes of a massive spleen? | Three Ms CML Myelofibrosis Malaria |
| 67. What drugs do you know which cause pulmonary fibrosis? | Chemo Tx: Methotrexate, cyclophosphamide, bleomycin Cardiac Tx: amiodarone, propanolol Abx: nitrofurantoin, sulphasalazine |
| 68. What is caplan's syndrome? | Large rheumatoid nodules in coal workers' lungs. |
| 69. What would you expect to happen to the second heart sound in cor pulmonale? | loud HS II |
| 70, What investigations would you do to assess acromegaly? | CXR: cardiomegaly ECG and echo: IHD (DM and HTN) Pituitary function tests (GH, IGF-1, T4, ACTH, PRL and testosterone) Glucose: DM Visual perimetery: bitemporal hemianopia MRI pituitary |
| 71. What are the important points to check for in taking a Hx of acromegaly? | Increased hand, feet and jaw size Change in appearance Coarse oily skin Headaches Peripheral vision loss Joint pain |
| 72. What classes of disease would you consider if asked to examine the hands in PACES? | Neurological (nerve entrapment or muscle disease) Rheum (RA) Endocrine (acromegaly) |
| 73. How long would you expect a bioprosthetic versus a mechanical valve replacement to last? | A bioprosthetic valve would be expected to fail within 10-15 years whereas a mechanical valve would function for 20-30 years. |
| 74. What is the mortality rate of a patient with prosthetic valve endocarditis? | PVE has an overall mortality of around 50%. If the PVE occurs within 60 days of implantation the mortality is much higher, at around 75% |
| 75. What are the causes of mitral regurgitation? | Acute: IHD, endocarditis (BE) Chronic: Degenerative mitral valve disease Rheumatic heart disease LV dilatation mitral valse prolapse papillary muscle dysfunction Connective tissue disease |
| 76. What are the clinical signs of severity in mitral regurgitation? | Soft first heart sound Palpable thrill Heaving apex beat 3rd heart sound |
| 77. What are the consequences for group 1 and 2 driving licence holders after an MI? | Group 1: must stop for 4 weeks but need not inform the DVLA. Group 2: Must stop and can only retrieve licence if can pass stage 3 of and ETT off anti-anginal Tx. |
| 78. What conditions would be expected to give rise to a pure motor syndrome? | Distal myopathy Multifocal motor neuropathy MND Myasthenia gravis |
| 79. What are the complications of coronary angiography? | Heamatoma at access point Reaction to contrast/renal toxicity Embolic stroke (1/500) |
| 80. What clotting disorders might be associated with DVT? | Factor V Leiden Protein C or S deficiency Antithrombin III deficiency |
| 81. What would your DDx be for a unilateral swollen arm? | Lymphoedema (+/- lymphadenopathy, Pancoast's tumour) Subclavian thrombosis Superior VC obstruction |
| 82. What are the main complications of cardiac valve replacement? | Heamorrhage Thomboembolus Infective endocarditis |
| 83. What is your DDx for spastic paraparesis? | Transverse myelitis (eg. MS) Cord compression Vit B12 deficiency MND Trauma Cerebral palsy |
| 84. What are the radiologic features of osteoarthritis? | Narrowing of joint space Subchondral bone sclerosis Osteophytes Bone cysts |
| 85. What are the clinical features of osteoarthritis in the hands? | Heberden's nodes (osteophytes) Squaring of the thumb Reduced ROM |
| 86. What is your Ddx for pain and swelling in the joints of the hands? | RA OA Psoriatic arthritis Crystal arthropathy |
| 87. How would you distinguish between inflammatory and non-inflammatory causes of pain and swelling in the hands? | Duration of morning stiffness Pattern of joint involvement (Prox and symmetric = RA, distal and asymmetric = gout or psoriatic ) Involvement of CMC (carpometacarpal) joint is typical of OA (squaring of thumb). |
| 88. What is your Ddx for the cause of end stage renal failure? | DM HTN Glomerular nephritis PKD Reflux nephropathy Renal vascular disease |
| 89. What autoantibodies are seen in lupus? | ANA: pres in 95% Anti-histone: may suggest a drug cause Anti-dsDNA: v specific but sen = 60% Anti-Sm: v specific bu sen = 20% Anti-Ro and ant-La: ANA -ve subacute cutaneous lupus Antiphospholipid: sens = 40% |
| 90. What Ix would you request to investigate the cause of end stage renal disease? | BP Bloods: glucose, renal function, ESR, Ab-screen for vasculitis. Renal US +/- renal angiography |
| 91. What are the stages of kidney failure based on the eGFR levels? | 1: eGFR>90 + evidence of damage 2: eGFR 60-90 + evidence of damage 3: eGFR 30-60 4: eGFR 15-30 5: eGFR<15 |
| 92. What is the frequency of testing and FU required for each of the 5 stages of renal failure? | 1 & 2: Annually 3: 6 months 4: 3 months 5: 6 weeks |
| 93. What are the principal side effects of haemodialysis? | Fatigue Hypotension Staph infections Muscle cramps Itchy skin Insomnia Bone and joint pain Loss of libido Dry mouth Anxiety |
| 94. What pharmacological agent might you use to treat neuropathic pain in diabetic neuropathy? | Tricyclics (eg Amitriptyline) or anticonvulsants (e.g. gabapentin) IV lidocaine or topical capsaicin in intractable cases |
| 95. What are the indications for lobectomy? | Old TB Non-small cell carcinoma Bronchectasis with recurrent haemoptysis Solitary pulmonary nodule |
| 96. What are some of the complications of lung cancer? | SVC obstruction Recurrent laryngeal nerve palsy Horner's + wasted small muscles of hand T1 Endocrine: gynaecomastic (ectopic \[\beta\]HCG) Neuro: LEM, periph neuropathy, proximal myopathy, paraneoplastic cerebellar degeneration. Derm: acanthosis nigricans, dermatomyositis |
| 97. What are the possible treatments for NSCLC? | Surgery: lobectomy or pneumonectomy Rx Chemo: EGFR +ve - erlotinib |
| 98. What are the possble treatments for SCLC? | Chemo: benefit with 6 courses. |
| 99. What form might palliative medical care take in lung malignancy? | MDT Dexamethasone and Rx for mets Stent and dex for SVCO Rx for haemoptysis, bone pain, cough Chemical pleurodesis - talc Opiates for cough and pain |
| 100. What is the Abx Tx for pulmonary TB? | PIRE Pyrazinamide (6M): se=hepatitis Isoniazid (2M): se = periph neuropathy Rifampicin(2M): se = Hepatitis + rogers the OCP Ethambutol(6M): retrobulbar neuritis and hepatitis |
| 101. What is the Tx for extra pulmonary TB? | Abx (PIRE) up to 12 months Corticosteroids (e.g. pred) if cerebral disease |
| 102. When should latent TB be Tx? | 1. People aged <36 2. People with HIV 3. Healthcare workers 4. People with evidence of scarring caused by TB, as shown on a chest X-ray, but who never received treatment |
| 103. What is the Ddx for a new proximal myopathy? | Endocrine disorders (Cushing's) Polymyositis |
| 104. How would you distinguish polymyositis from PMR? | CK, AST, ALT +/- muscle biopsy |
| 105. Which of the following drugs is contraindicated in severe aortic stenosis?... Beta-blockers, furosemide, spironolactone, ACE inhibitors, amiodarone. | ACE inhibitors |
| 106. What are the indications for aortic valve replacement? | Secondary dyspnoea, angina, syncope or pre-syncope. Pressure gradient >60mmHg Serial evidence of left ventricular dysfunction |
| 107. What are the complications of prothetic cardiac valves? | All valves Valvular dysfunction Infective endocarditis Metallic only Microagiopathic haemolytic anaemia Thromboembolism |
| 108. What are the causes of aortic stenosis? | Degenerative calcific change Bicuspid valve Rheumatic heart disease |
| 109. What is the difference between an essential tremor and an intention tremor? | An intention tremor is only present as the target is approached, whereas an essential tremor may be present throughout all phases of movement. |
| 110. What is the difference between a stroke and a TIA? | They are both focal neurological deficits secondary to a vascular lesions, however a TIA resolves within 24 hours and a stroke does not. |
| 111. What is a consent form 4? | A form documenting a decision to perform a procedure on a patient where… 1. The patient lacks capacity to consent to or refuse the treatment. AND 2. The treatment is in the best interest of the patient. |
| 112. What is the differential diagnosis for erythema nodosum? | Sarcoidosis Streptococcal infection Drugs (sulphonamides) TB IBD |
| 113. What skin lesions are seen in sarcoid? | Lupus pernio Erythema nodosum Nodules Scar infiltration Plaques |
| 114. What are the most common organs affected in sarcoidosis? | The lungs (90%), eyes (25%), skin (25%) lymph nodes. |
| 115. What investigations would you request in a suspected new presentation of sarcoid? | FBC, U&E, LFTs, ACE level, CXR ECG Pulmonary function tests Urinalysis Eye clinic Specialist referral (eg resp in pulmonary involvement) |
| 116. What symptoms should you ask about in sarcoid? | Fever, fatigue, SOB, weight loss, vision changes, palpitations, abdominal symptoms, LOC. |
| 117. What treatment approaches exist for sarcoid? | Inhaled steroids (for minor cough) Topical steroids (for skin) NSAIDs for joint involvement Oral steroids (prednisolone) |
| 118. Which joints are commonly affected by RA? | PIPJs, MCPJ, MTPJ, wrists, knees. |
| 119. What are the causes of anaemia in RA? | Chronic disease Felty's syndrome Irod deficiency NSAIDS Folate deficiency Coexisting pernicious anaemia B12 deficiency |
| 120. What is Felty Syndrome? | RS, splenomegaly and neutropenia. |
| 121. What are the grades of diabetic retinopathy? | Background: micro-aneurysms, retinal haemorrhages, +/- exudates Pre-proliferative: cotton wool spots. Proliferative: new vessel formation. +/- maculopathy (hard exudates near macula) |
| 122. What is the Tx for background, pre-proliferative and proliferative retinopathy? | Diabetic control, HTN control etc. + Background: annual screening Pre-proliferative: every 4 months Active proliferative requires pan-retinal photocoagulation. |
| 123. What are the clinical features of cor pulmonale? | Parasternal heave Raised JVP Ankle/sacral oedema. |
| 124. What are the consequences for a group 1 driving licence holder who has a seizure? | Stop driving for 1 year, with 3 exceptions 1. First fit: no driving for 6 months 2. All seizures in past 3 years were nocturnal-you can drive. 3. Seizure was provoked (e.g. head injury) |
| 125. What are the consequences for a group 2 driving licence holder who has a seizure? | Needs to stop driving for 10 years, and can only regain it if fit free for 10 years and off anticonvulsants when reassessed. i.e. end of career. |
| 126. What are the implications for a group 1 driving licence holder who is diabetic? | Okay as long as you do not have poor vision, frequent hypos, severe hypos (requiring hospitalisation), or loss of hypo awareness. |
| 127. What are the implications for a group 2 driving licence holder who is diabetic? | You can drive even on insulin provided: 1. You have stable glycaemic control over 3 months. 2. You can evidence this using a monitor with a memory function. 3. You are checking your BM at least twice a day. |
| 128. What is the target HbA1c for a type II diabetic? | <6.5% |
| 129. At what HbA1c would you consider beginning insulin Tx on top of oral Tx for diabetes? | >7.5% |
| 130. What are the second line oral Txs available if diet and metformin fail to achieve glycaemic control? | 1. Sulphonylureas (weight gain + hypo risk) 2. Gliptins 3. GLP-1 mimetic 4. Glitazone 5. SLGT-inhibitor (2-5 have low hypo risk and are weight neutral or induce weight loss) |
| 131. What is your Ddx for binocular diplopia? | Nerve palsies Thyroid eye disease Myasthenia Ocular myopathies (e.g. Oculopharyngeal muscular dystrophy) |
| 132. What is an Adies pupil? Who gets it typically? What other sign is commonly present? | A tonically dilated pupil. More common in women. Absent ankle reflexes often accompany it. |
| 133. What does an RAPD generally denote? | Optic nerve disease |
| 134. What is your differential for painful loss of vision? | Retrobulbar neuritis Giant cell arteritis |
| 135. What are the possible components of treatment for hypopituitarism? | Hydrocortisone Thyroxine Sex hormones (HRT or testosterone) Desmopressin (ADH anologue) |
| 136. What are the clinical features of hyperthyroidism? | Eyes: lid retraction & lid lag Peripheral: agitation, sweating, tremor, palmar erythema, tachy/AF, brisk reflexes |
| 137. What are the clinical features of Grave's which distinguish it from simple hyperthyroidism? | Eyes: Proptosis, chemosis, ophthalmoplegia Peripheral: Thyroid acropachy, Pretibial myxoedema |
| 138. What are the potential complications of thyroid eye disease? | Exposure keratitis Optic nerve compression Papilloedema |
| 139. What Ix would you undertake for suspected case of Grave's disease? | TFTs: TSH and T3/T4 Thyroid autoantibodies Radioisotope scanning: increased I-131 uptake in Graves, reduced in thyroiditis. |
| 140. What treatments exist for Grave's disease? | B-block (e.g. propanolol) & Thionamide (e.g. Carbimazole) Stop at 18 months and assess. 1/3 remain euthyroid. For other 2/3 repeat thionamide Radioiodine I-131 Subtotal thyroidectomy. |
| 141. What are the salient complications of carbimazole? | Bone marrow suppression causing neutropenia and agranulocytosis. |
| 142. What are the clinical features of hypothyroidism? | FAT, TIRED and COLD Fatigue and low energy levels Cold intolerance Weight gain |
| 143. What drugs are known to cause hypothyroidism? | Amiodarone, lithium, thionamides (e.g. carbimazole) |
| 144. What are the causes of a Goitre? | Idiopathic Iodine deficiency Hashimoto's thyroiditis Grave's Goitrogens (e.g. lithium) Multinodular goitre Adenoma Carcinoma. |
| 145. What is your differential for a mixed sensorimotor peripheral neuropathy? | Diabetes Hypothyroidism Charcot-Marie-Tooth CIDP CTD (SLE and RA) POEMS Paraneoplastic (esp haem) Drugs (phenytoin) |
| 146. What tool would you use to assess risk in a new presentation of angina or hypertension? | QRISK2 (USES: age, BP, smoking, ratio of total serum cholesterol to high-density lipoprotein cholesterol) body mass index, ethnicity, deprivation, family history, CKD, RA, AF, DM, and antihypertensive treatment.) |
| 147. What is your differential for haemoptysis? | LRTI (pneumonia, abscess, TB, fungus) Malignancy PE Vasculitis Osler-Weber-Rendu Parenchymal disease (sarcoid, fibrosis) Cardiac (pulm oedema, mitral stenosis) Bleeding diathesis |
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.