6620765
Beschreibung
Karteikarten von Ashutosh Kumar, aktualisiert more than 1 year ago
|
|
Erstellt von Ashutosh Kumar
vor etwa 8 Jahre
|
|
| Frage | Antworten |
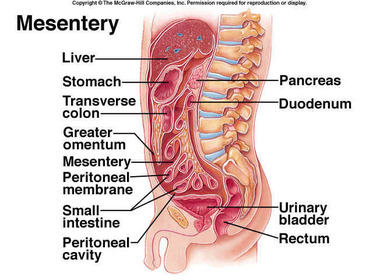
| List and briefly describe the abdominal structures derived from the peritoneum: | 1. Mesentery: A double layer of peritoneum (containing blood vessels, nerves and lymphatics) which anchor the viscera to the posterior abdominal wall. 2. Omenta: Extension of the peritoneum, 'aprons' from the stomach and superior duodenum. 3. Peritoneal ligaments: Membranous folds of peritoneum which support and maintain the position of an organ. 4. Peritoneal recesses: Potential spaces in the peritoneal cavity. 5. Peritoneal fossae: Depressions in the anterior abdominal wall. |
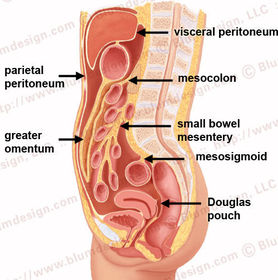
| Describe the Small intestine mesentery: Mesoappendix: Transverse mesocolon: Sigmoid mesocolon: | The mesentery is a double layer of peritoneum which contains nerves, lymphatics and blood vessels supplying the viscera. The mesentery functions to anchor the viscera to the posterior abdominal wall. Small intestine mesentery: attaches the jejunum and ileum to the posterior abdominal wall. Runs diagonally, from the right lower quadrant to left upper quadrant. Mesoappendix: An extension of the terminal ileal mesentery. Transverse mesocolon: Anchors the transverse colon to the posterior abdominal wall. Continuous with the posterior layer of the greater omentum. Sigmoid mesocolon: Anchors the sigmoid colon to the posterior abdominal wall. |
| Describe the functions of the mesentery: | The mesentery contains the blood vessels, nerves and lymphatics of the supported viscera. The mesentery anchors the viscera to the posterior abdominal wall. The mesentery has a lot of fat. which serves two functions: 1. Stored energy. 2. Fat associated lymphatic tissue (FALT); keeps the colonic bacteria in check. |
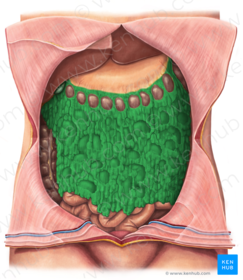
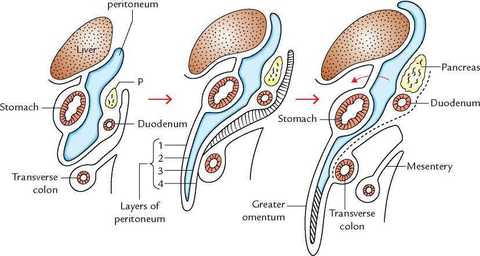
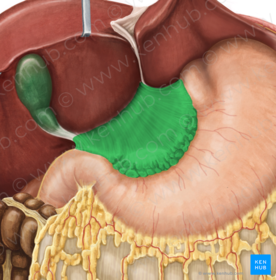
| Describe the anatomy of this structure: Describe the functions: | The greater omentum extends inferiorly from the greater curvature of the stomach and the superior duodenum to hang in front of the coils of small intestine. It then wraps under itself (2 layers upon 2= 4 layers) and ascends to attach to the transverse colon. Functions: The greater omentum is considered mobile. This is because it can become adherent to inflamed areas and therefore seal off and prevent spread of infection. Hence, the greater omentum is often called the 'policeman of the abdomen'. |
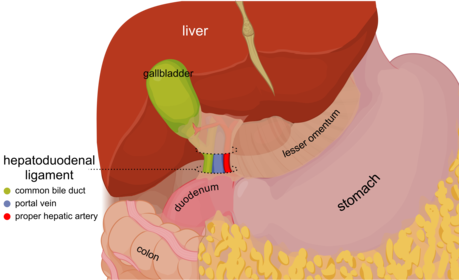
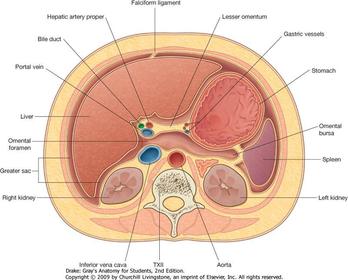
| Describe the anatomy of this structure: | The lesser omentum extends from the lesser curvature of the stomach and superior aspect of the superior duodenum to the porta hepatis of the liver (where structures enter and exit the liver). The lesser omentum is thickened as two ligaments: 1. Hepatogastric; extends between the lesser curvature and porta hepatis. 2. Hepatoduodenal; extends between superior duodenum and porta hepatis; contains the portal triad; common bile duct on right, hepatic artery proper on left and portal vein posterior. |
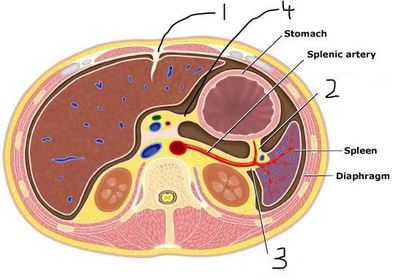
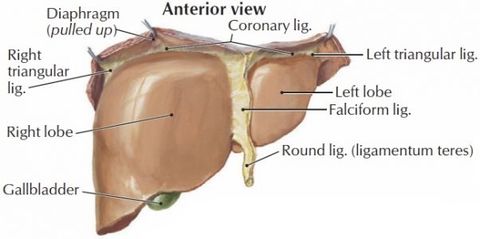
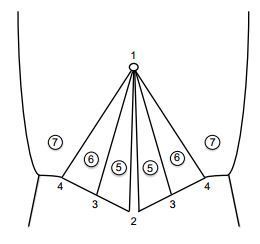
| Name and describe 1: Describe what runs in the inferior margin of 1: | 1: Falciform ligament; a sagittally oriented ligament that extends between the anterior surface of the liver and the inner anterior abdominal wall, extending as far inferior as the umbilicus. Running in the free inferior margin is the ligamentum teres/round ligament; the obliterated umbilical vein which carries oxygenated blood from the placenta. |
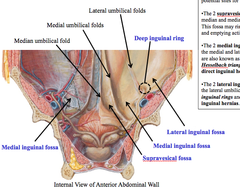
| Describe 2, 3 and 4: | 2: Median umbilical fold/ligament; remnant of the urachus. 3: Medial umbilical fold/ligament; remnant of the umbilical artery. 4: Lateral umbilical fold/ligament; peritoneal fold over the inferior epigastric vessels. |
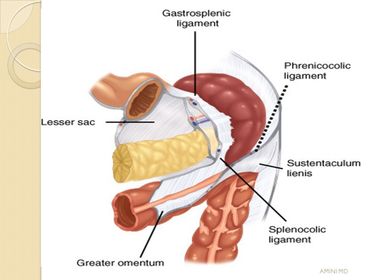
| Describe the ligaments extending from the spleen: | 1. Gastrosplenic: From the fundus of the stomach to the hilum of the spleen. 2. Splenorenal: From the anterior surface of the left kidney to the hilum of the spleen. 3. Splenocolic: Inferior spleen to left colic flexure. 4. Splenophrenic: Superior spleen to diaphragm. |
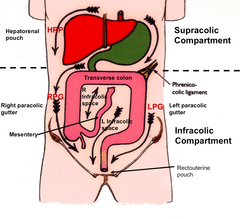
| Describe how the abdominal viscera can be subdivided with respect to the transverse colon: | The abdominal viscera can be grouped with respect to where they lie in relation to the transverse colon; above (supracolic), below (infracolic). Supracolic organs include: esophagus, stomach, liver, gallbladder and biliary system, spleen and pancreas. |
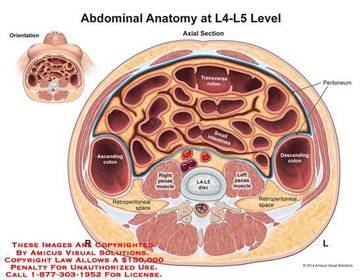
| Describe how the infracolic compartment can be further subdivided: | The infracolic compartment can be further subdivided into right and left compartments by the mesentery of the small intestine; this runs diagonally along the posterior abdominal wall from the right lower quadrant to left upper quadrant. |
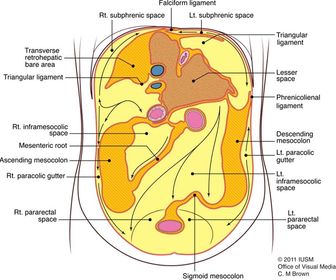
| Describe the location of the ascending and descending colon: | They are retroperitoneal i.e not suspended in the peritoneal cavity but relatively fixed on the posterior abdominal wall. They once had mesentery but this has since fused with the posterior abdominal wall. Hence they are secondary retroperitoneal rather than primary (always retro). |
| Describe the paracolic gutters and their clinical significance: | Lieing between the lateral aspects of the ascending and descending colon and posterolateral abdominal wall are the right and left paracolic gutters, respectively. They enable the spread of infection between the supracolic and infracolic compartments. The right paracolic gutter communicates with the right subphrenic space, hepatorenal/subhepatic/Morrison's pouch and pouch of douglas (rectouterine in female, rectovesical in male). The left paracolic gutter cannot communicate with the splenorenal space because of the intervening phrenicocolic ligament (from splenic flexure to diaphragm). |
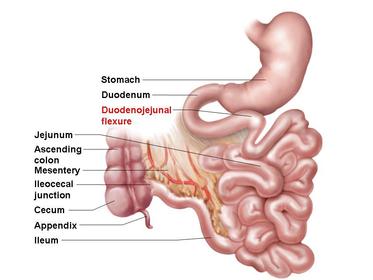
| Describe how the divisions of the small intestine are recognized: | The small intestine consists of 3 parts: 1. Duodenum. 2. Jejunum. 3. Ileum. The duodenojejunal flexure (DJ flexure) marks the junction between the duodenum and jejunum. There is no distinct morphological demarcation between the jejunum and ileum. Instead, the proximal two-fifths from the DJ flexure is arbitrarily considered the jejunum and the distal three-fifths the ileum. |
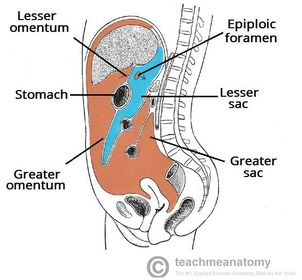
| Describe the divisions of the peritoneal cavity: | The peritoneal cavity can be divided into two spaces: 1. Greater sac; consists of 4 layers and contains no organs, extends from the diaphragm to the pelvis. 2. Lesser sac: Lies behind the greater sac and stomach but is anterior to the posterior abdominal wall and retroperitoneal organs such as the pancreas. The greater and lesser sac communicate via the epiploic foramen. |
| Name the boundaries of the epiploic foramen/omental window: Superior: Inferior: Anterior: Posterior: Name the ligaments which can be felt through the window in the lesser sac: | Superior: Caudate lobe of the liver Inferior: Superior aspect of superior duodenum Anterior: Hepatoduodenal ligament containing portal triad Posterior: IVC and right crus of the diaphragm Gastrosplenic and splenorenal ligaments can be palpated inside the lesser sac. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.