8513233
Beschreibung

Karteikarten von RadTech Fairy, aktualisiert more than 1 year ago
|
|
Erstellt von RadTech Fairy
vor fast 8 Jahre
|
|
| Frage | Antworten |
|
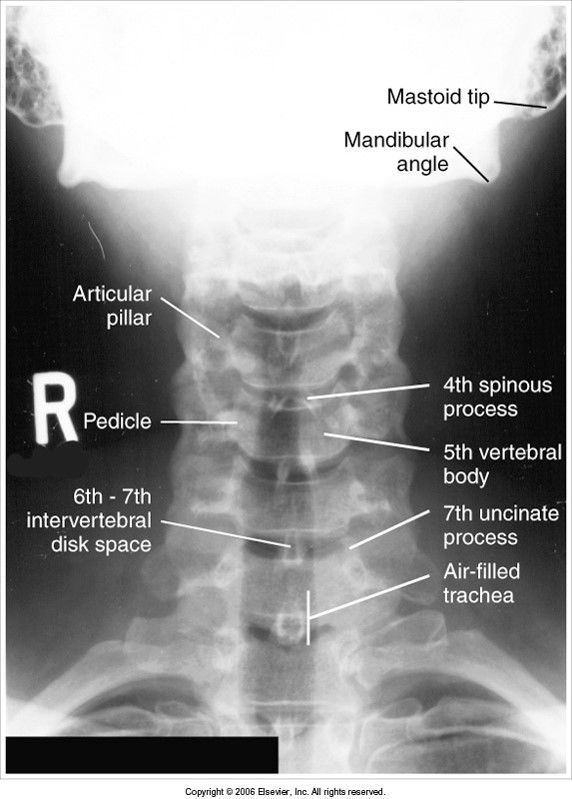
AP axial cervical spine
evaluation criteria
Image:
Ap Cspine (image/jpeg)
|
C3-C7 visible no rotation spinous processes lined up to midsagittal plane (MSP) SC joints are symmetric and equidistant from spine mastoid tips are equidistant from spine |
| chin depressed over C3 | |
| rotation to the left | |
|
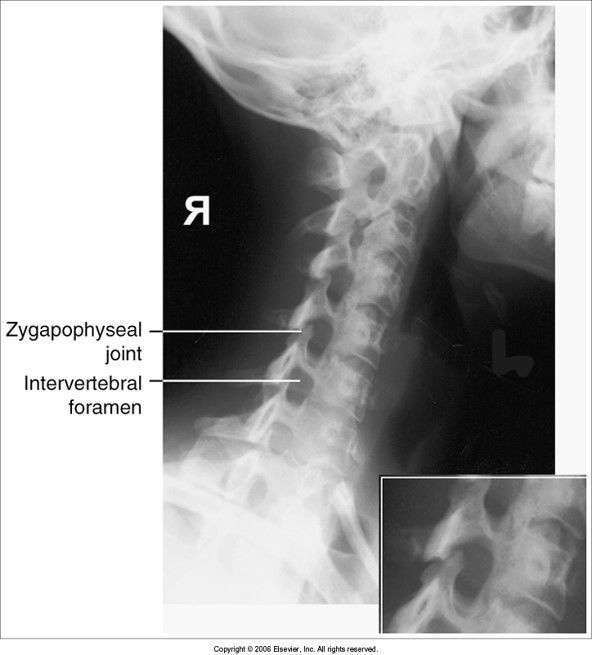
Oblique C-Spine
evaluation criteria
Image:
Oblique Cspine (image/jpeg)
|
RAO and LAO show IVF closest to IR RPO and LPO show IVF farther from IR open IVF pedicles in profile |
| no cephalic angle | |
| underrotation | |
| overrotation | |
|
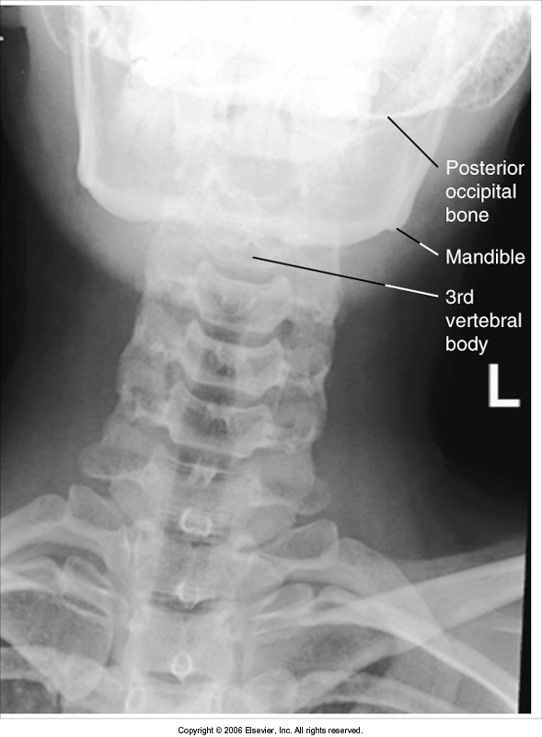
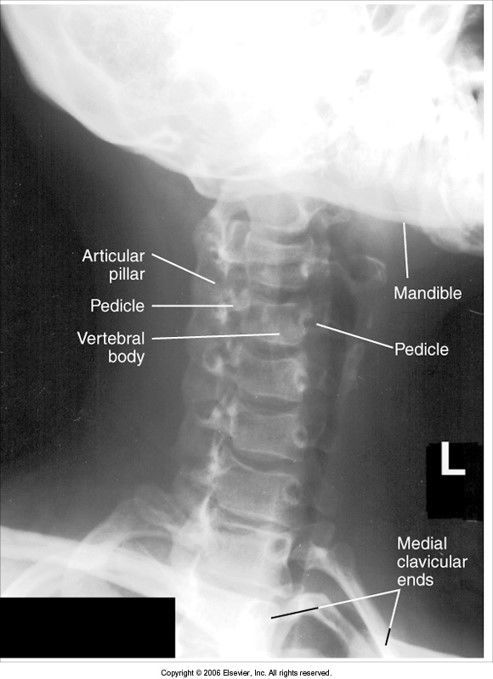
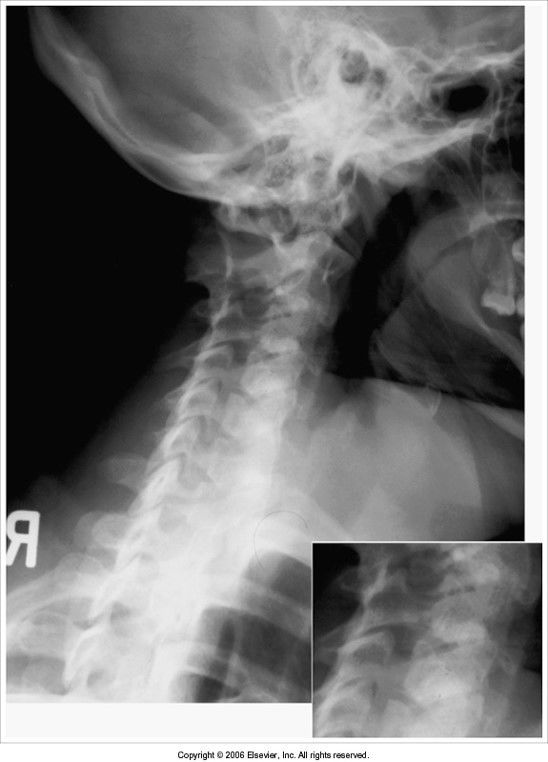
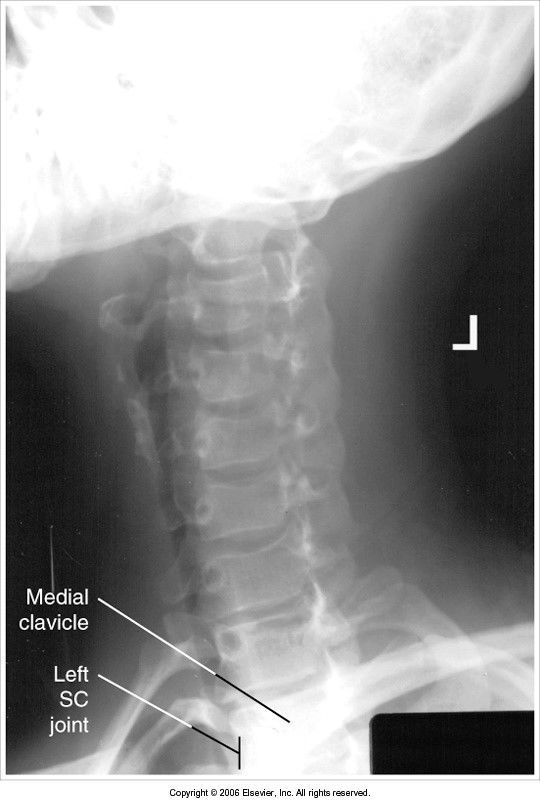
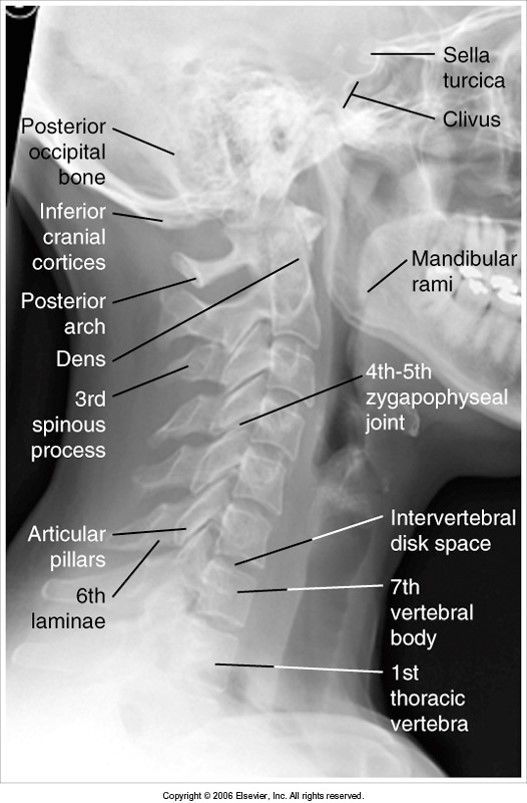
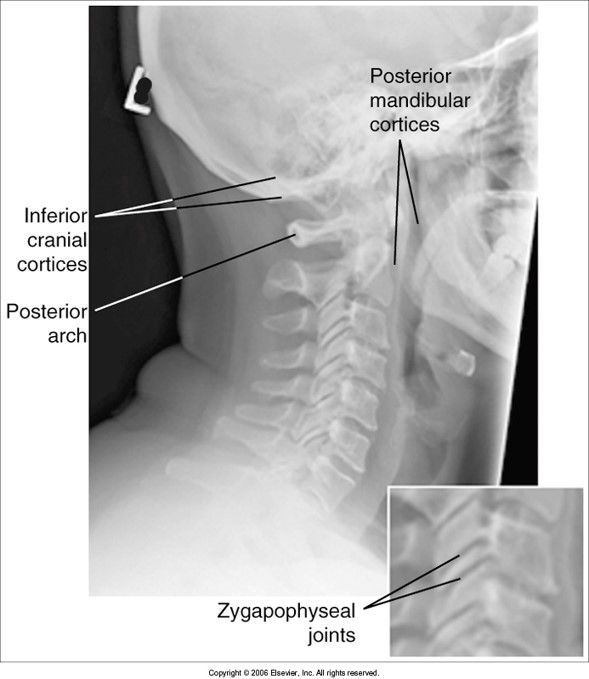
Lateral C-Spine
evaluation criteria
Image:
Lateral C Spine (image/jpeg)
|
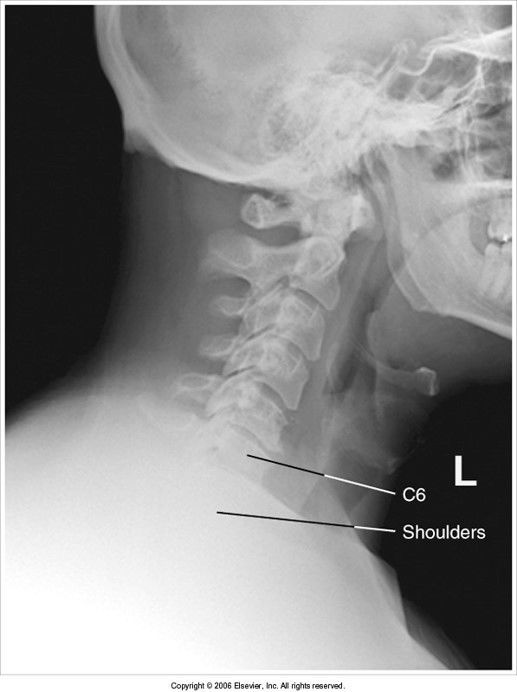
all 7 vertebrae are visible spinous processes in profile right and left zygapophyseal joints (z. jt.) and articular pillars are superimposed posterior arch and spinous process of C2 are in profile intervertebral disk spaces open |
| mandibular rami are not superimposed: pt. rotated articular pillars and z. jt.s are separated: pt. head tilted away from IR | |
| base of skull and sella turcica coned off z. jt.s closed: rotation | |
| mandible not superimposed: head is tilted z. jt.s are separated | |
| C7 is invisible behind the shadow of the shoulders - give pt weights to relax shoulders down | |
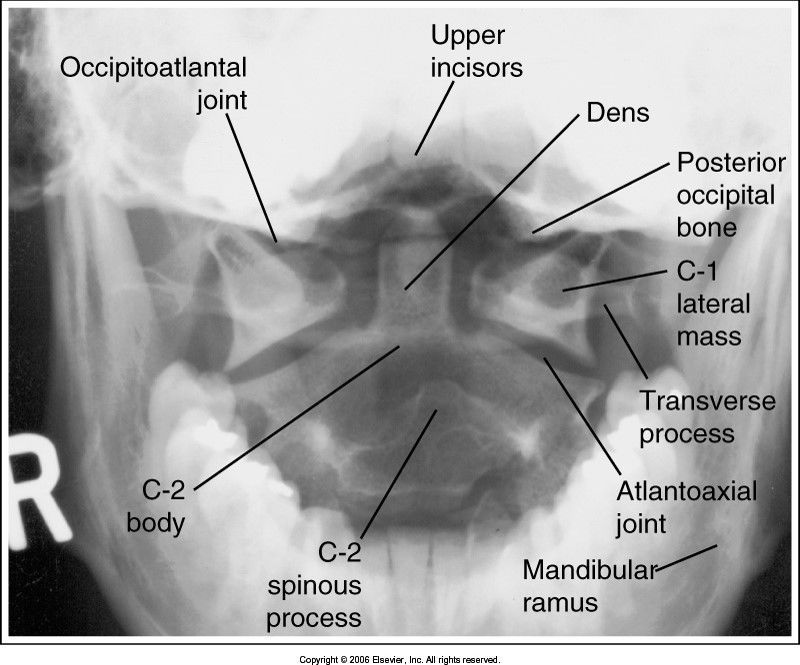
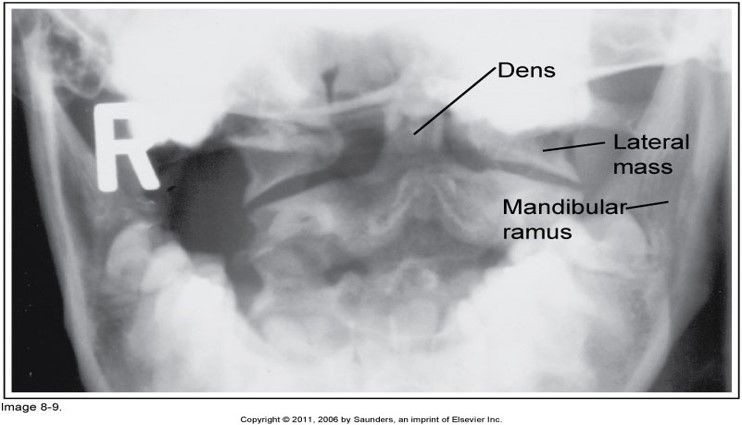
| AP Open Mouth evaluation criteria | atlas and axis, ondontoid, lateral masses of C1, and z. jt.s of C1-C2 are well visualized without superimposition |
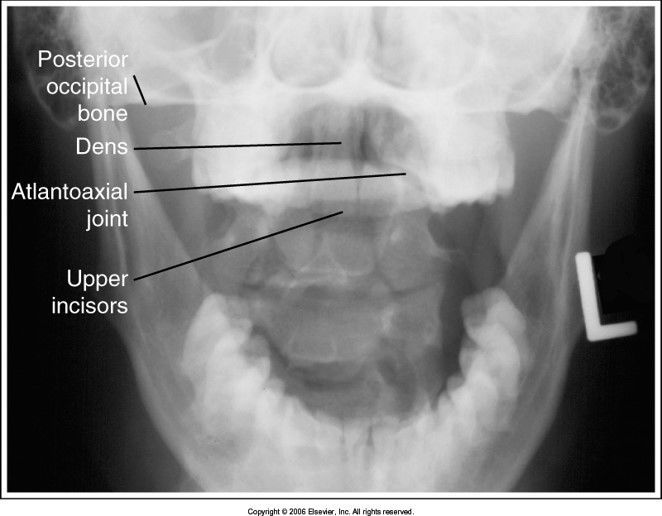
| teeth are superimposed over the dens: head is tilted forward | |
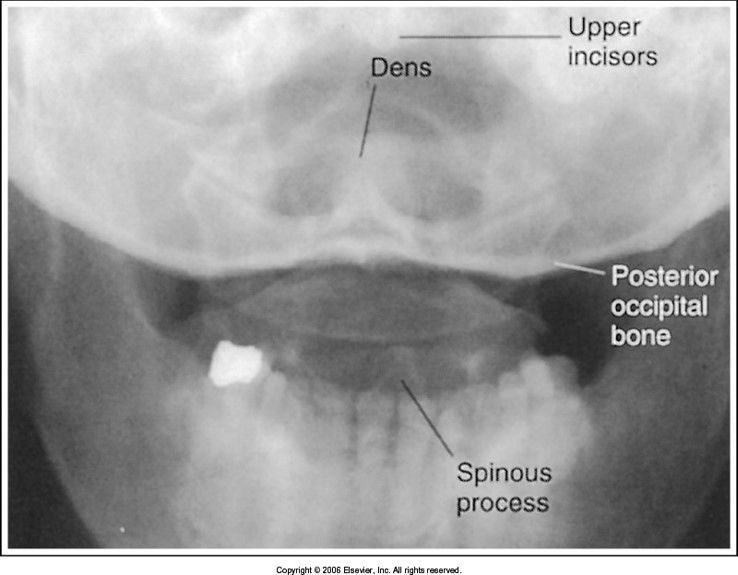
| base of the skull superimposes the dens: head is extended too far | |
| dens is situated to the left of the MSP: pt's head is rotated towards the right | |
|
AP Thoracic Spine
evaluation criteria
Image:
Ap Tspine (image/jpeg)
|
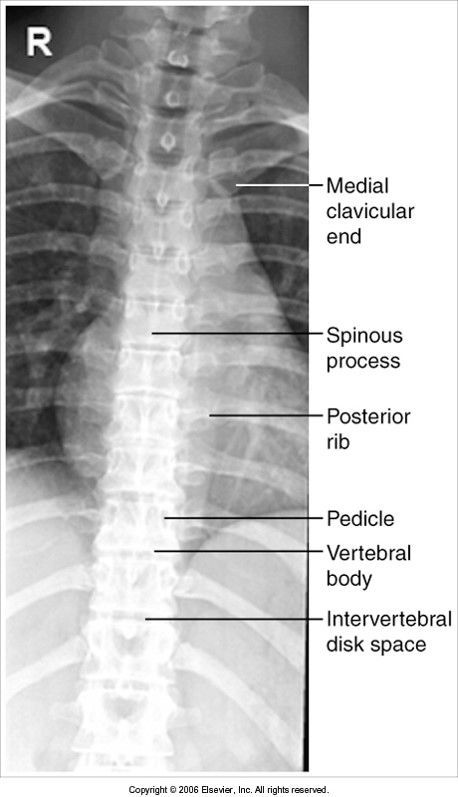
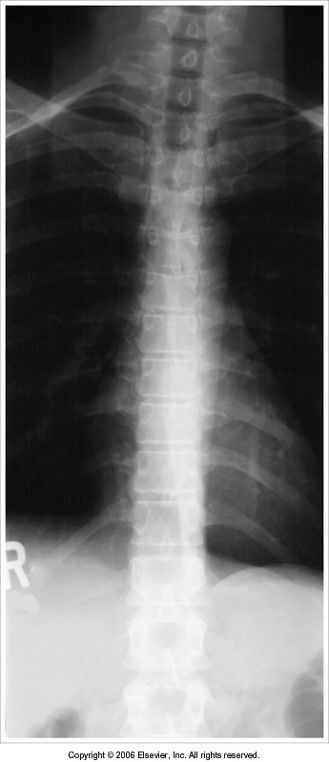
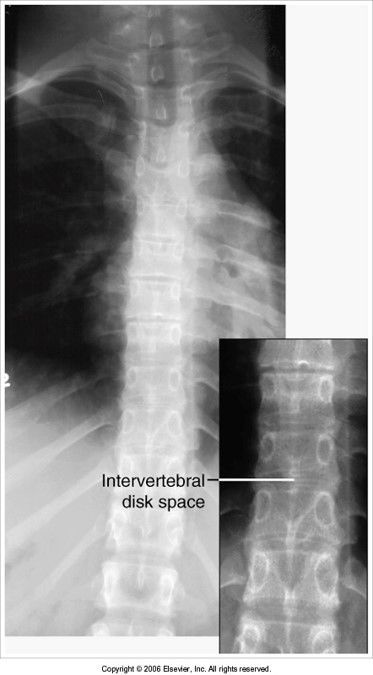
all 12 thoracic vertebrae are visible with no rotation, flexion, extension, or tilt collimation is evident exposure is taken after expiration to reduce lung volume and create more uniform density patient positioned so the thorax is under the cathode side of the beam (annode-heel effect)* |
| exposure was taken on full inspiration: lung fields are overexposed and density is not well distributed | |
| intervertebral joint spaces are obscured: pt's legs/knees were extended when they should've been flexed | |
|
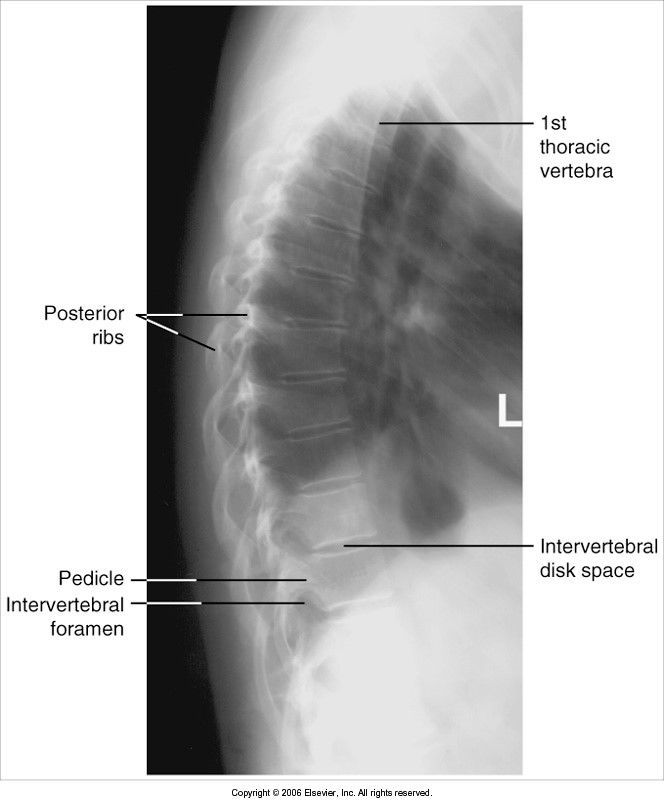
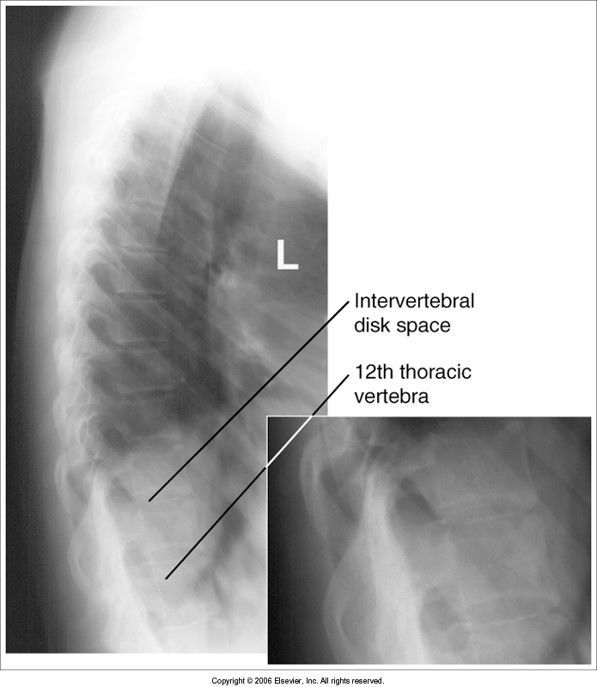
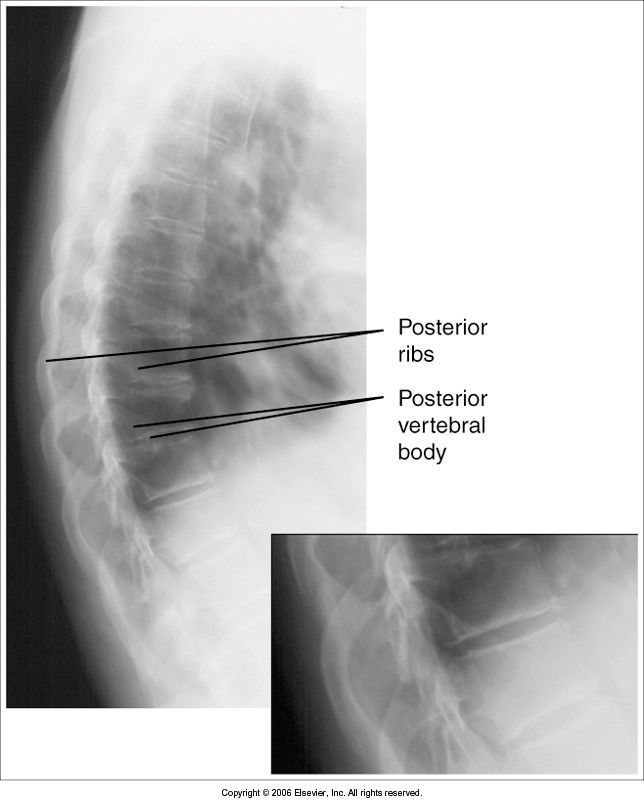
Lateral T-Spine
Evaluation Criteria
Image:
Lateral Tspine (image/jpeg)
|
thoracic bodies of T4-T12 are seen with open IVF and no rotation *exposure taken using a breathing technique to blur out the ribs and lung markings |
| ribs are not blurred out: inadequate breathing technique lower thoracic vertebral bodies are obscured: pt's hips were not supported so spine is curved laterally | |
| posterior ribs and vertebral bodies aren't superimposed: pt rotated | |
|
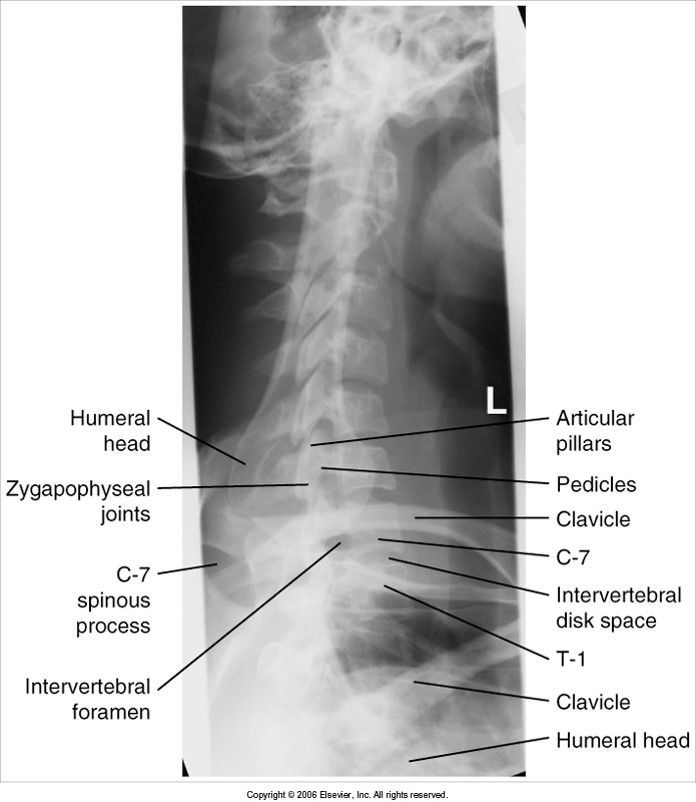
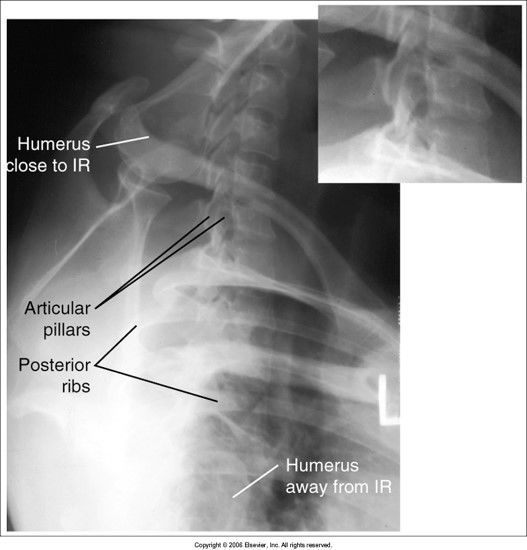
Swimmer's Lateral T-Spine
Evaluation Criteria
Image:
Swimmers Tspine (image/jpeg)
|
C5-T3 included humerus should be above head and aligned with vertebral column humerus away from IR should be anterior to spine intervertebral disk spaces should be open |
| acceptable (bontrager's demonstration picture) | |
| posterior ribs and vertebral bodies aren't superimposed: patient is rotated | |
|
Image:
Swimmers Tilt (image/jpeg)
|
intervertebral disk spaces closed: c-spine is not parallel to IR |
|
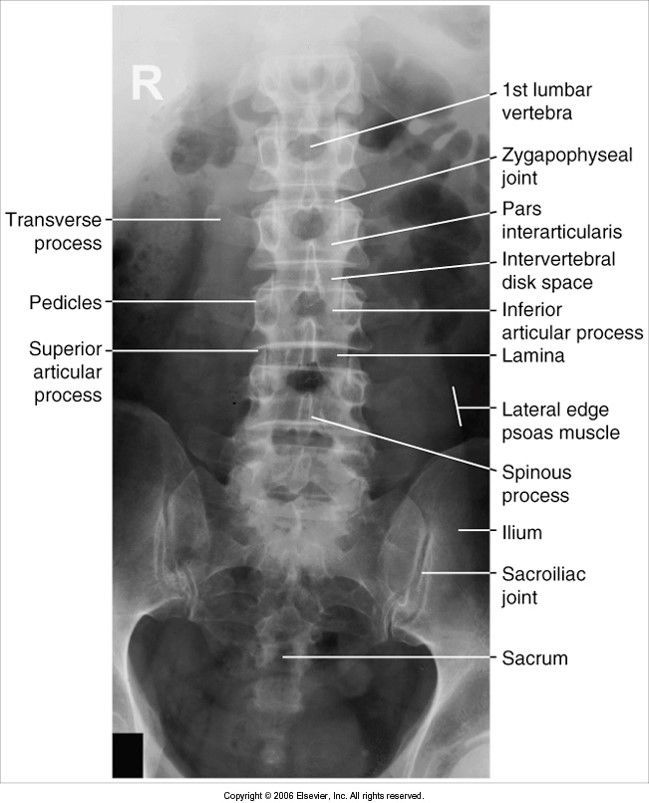
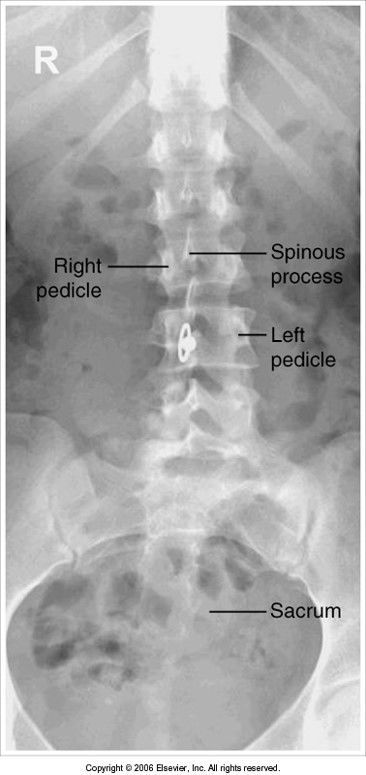
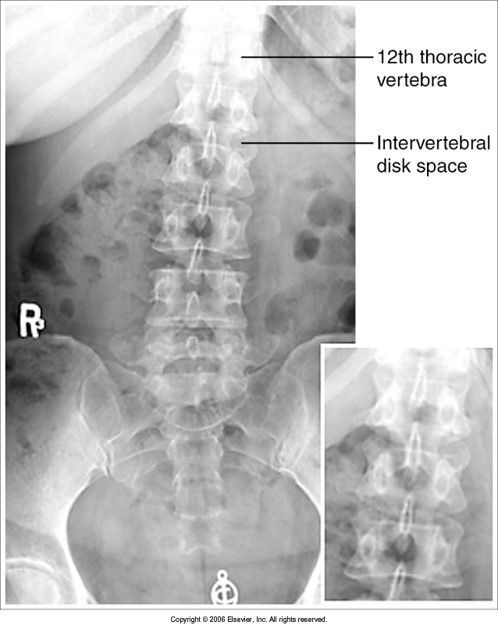
AP Lumbar
evaluation criteria
Image:
Ap Lumbar (image/jpeg)
|
T12-sacrum are included intervertebral disk spaces are opened patient positioned with knees and hips flexed sacrum/coccyx centered to MSP and pelvic inlet |
| spinous processes are shifted to the right of the midline and the sacrum/coccyx shifted to the right of MSP: patient's hips rotated towards the left | |
| extreme scoliosis | slight scoliosis |
| intervertebral disk spaces are closed: the knees and hips need to be flexed | |
|
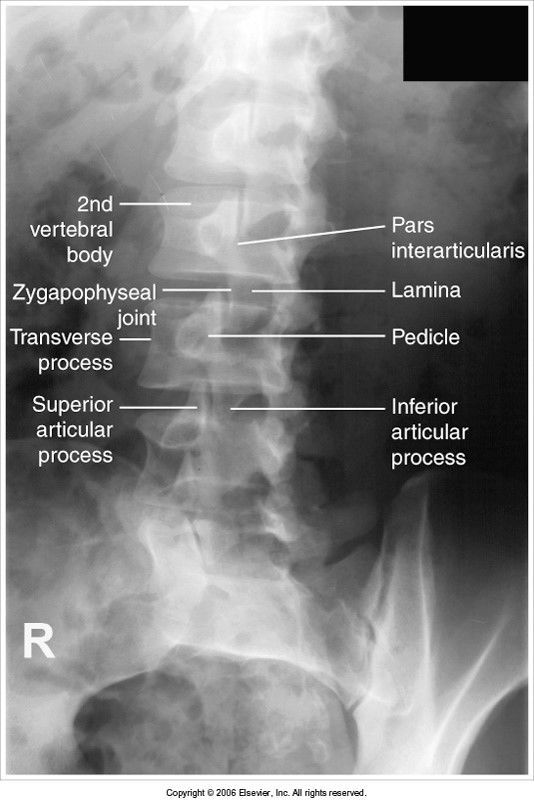
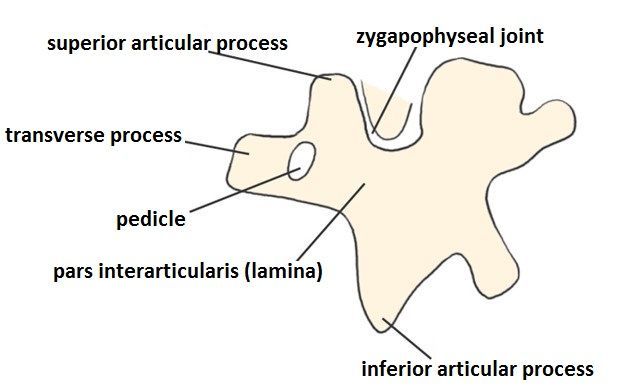
Oblique Lumbar
evaluation criteria
Image:
Oblique Lumbar (image/jpeg)
|
scotty dogs should be visible open z. jts LPO and RPO show the z jt closest to IR LAO and RAO show the z jt farther from IR |
|
Image:
Scottie Dog 2 (image/jpeg)
|
Scottie Dog |
| underrotation | |
| overrotation | |
|
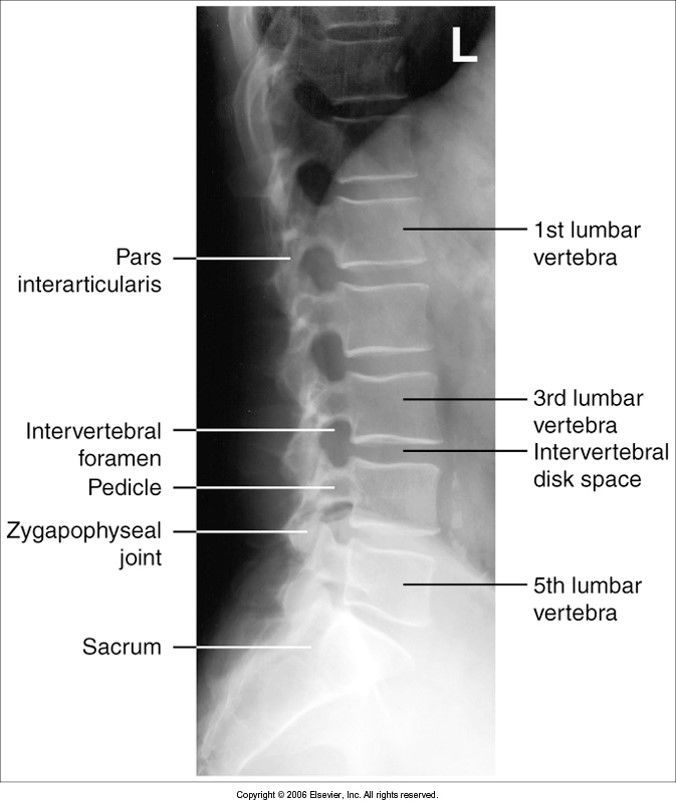
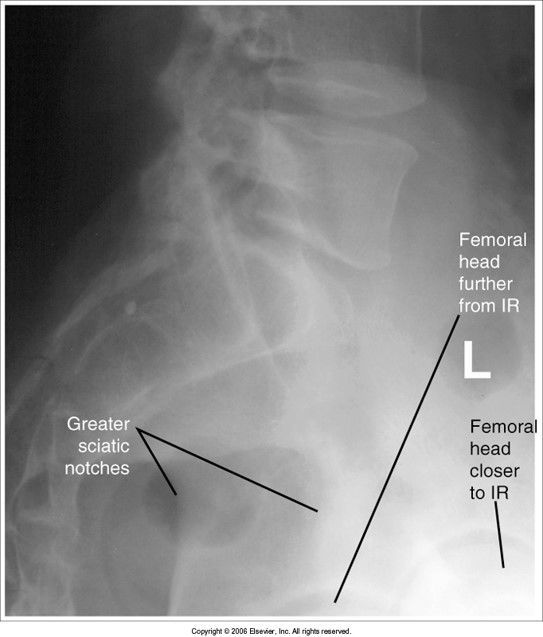
Lateral Lumbar
evaluation criteria
Image:
Lateral Lumbar (image/jpeg)
|
open intervertebral foramina (IVF) open intervertebral disk spaces |
| intervertebral disk spaces closed - hips/waist was not supported | |
|
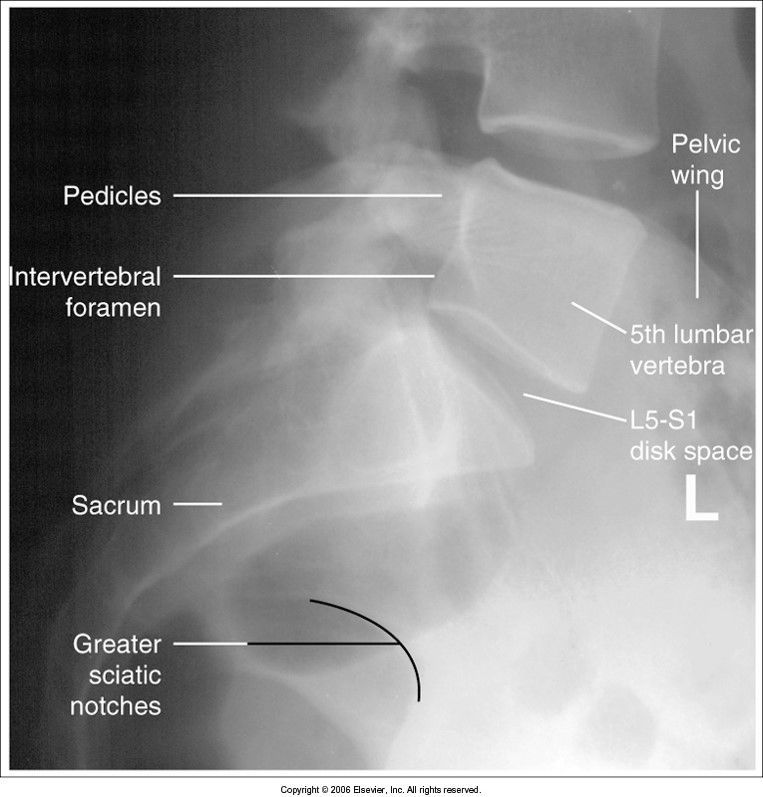
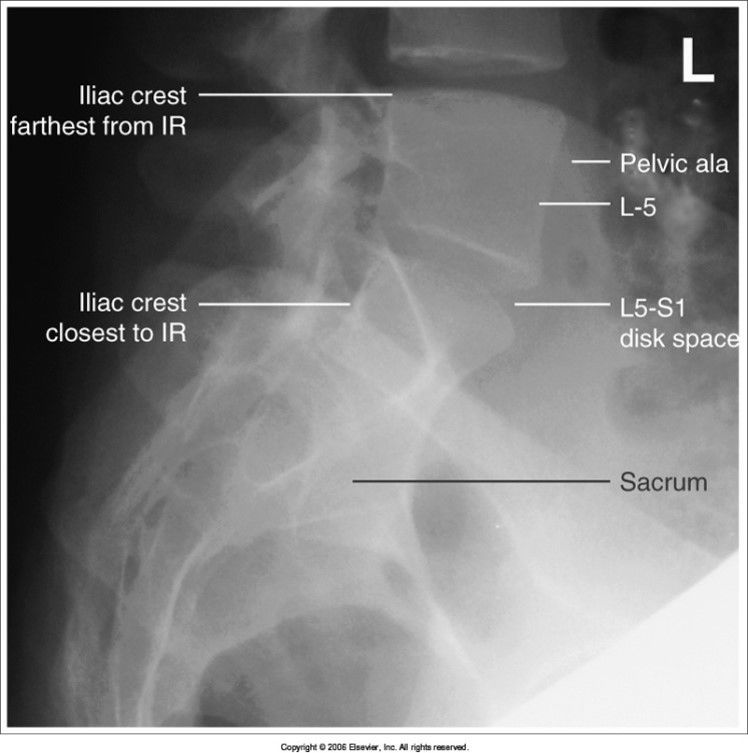
L5-S1 spot
evaluation criteria
Image:
L5 S1 Spot (image/jpeg)
|
lumbosacral joint open IVF clearly demonstrated right/left pedicles superimposed |
| iliac wings are not superimposed - pelvis is tilted from being unsupported | |
| femoral heads aren't superimposed: pelvis is rotated | |
|
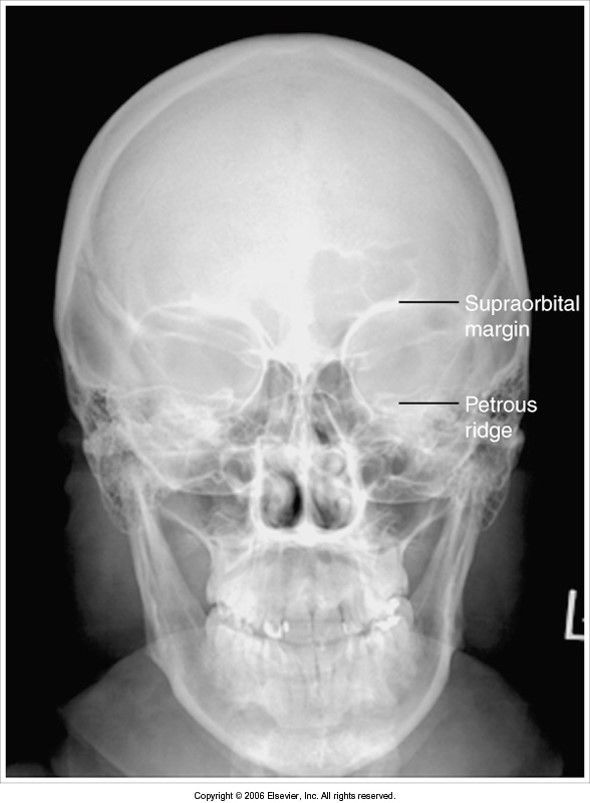
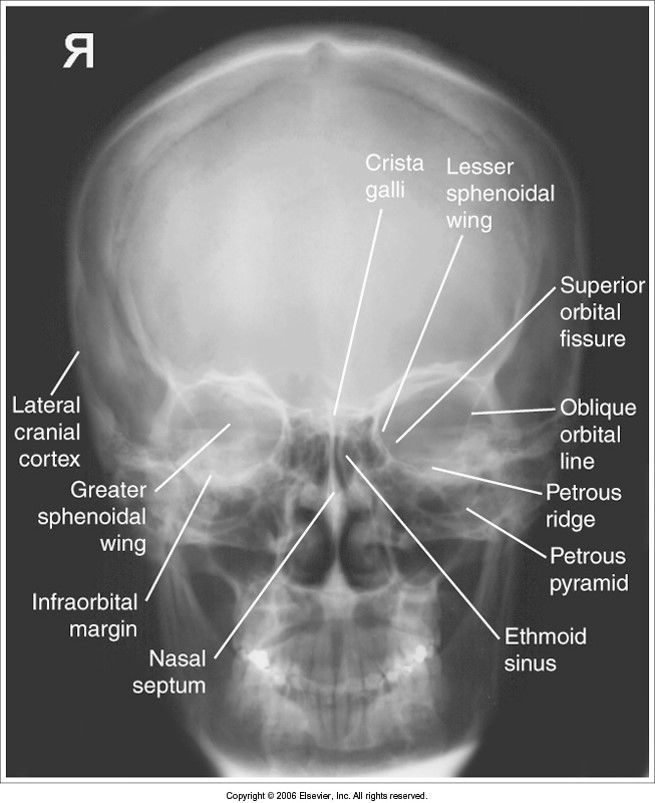
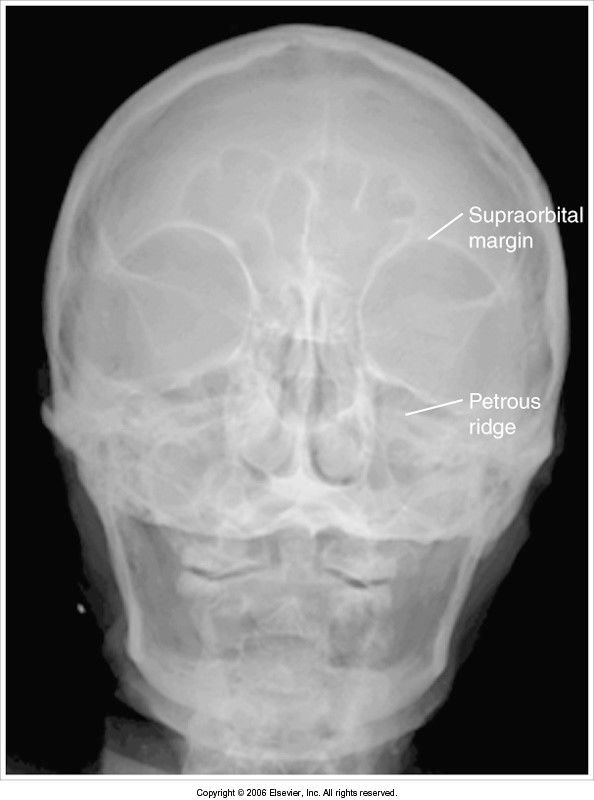
PA Skull 0 degrees
evaluation criteria
Image:
Pa Skull (image/jpeg)
|
petrous ridges fill the orbits orbits are symmetric and equidistant from MSP |
| petrous ridges aren't filling the orbits chin isn't tucked enough to get OML perpendicular to IR | |
| petrous ridges are seen above the orbital rims chin is tucked too much - OML isn't perpendicular | |
|
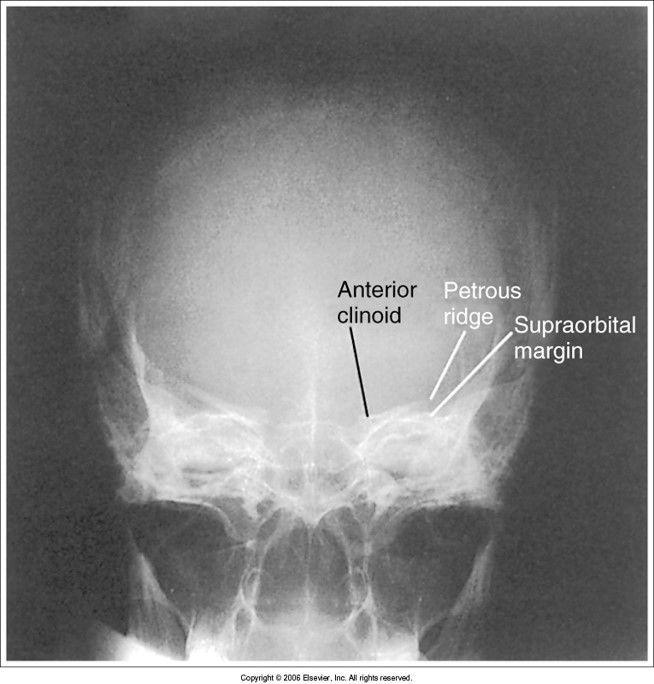
PA Caldwell 15
evaluation criteria
Image:
Pa Caldwell (image/jpeg)
|
petrous ridges are seen within lower 1/3 of orbits OML is perpendicular to IR |
| CR angle was 15 cephalic: orbits are magnified, skull is foreshortened *in trauma cases this is acceptable* | |
| head is tilted petrous ridges are below orbital floors: CR was angled too caudal | |
|
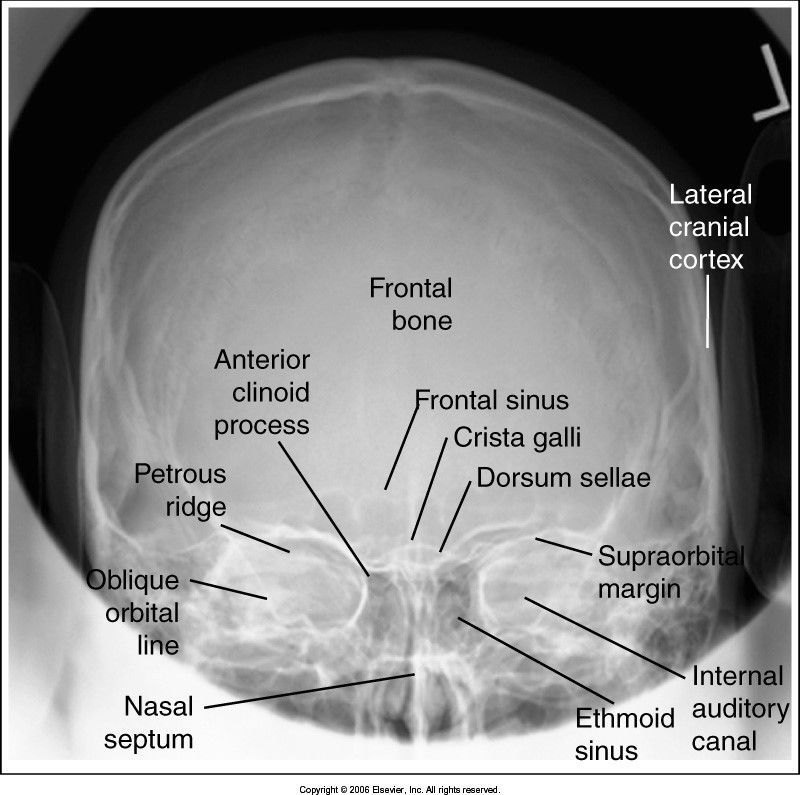
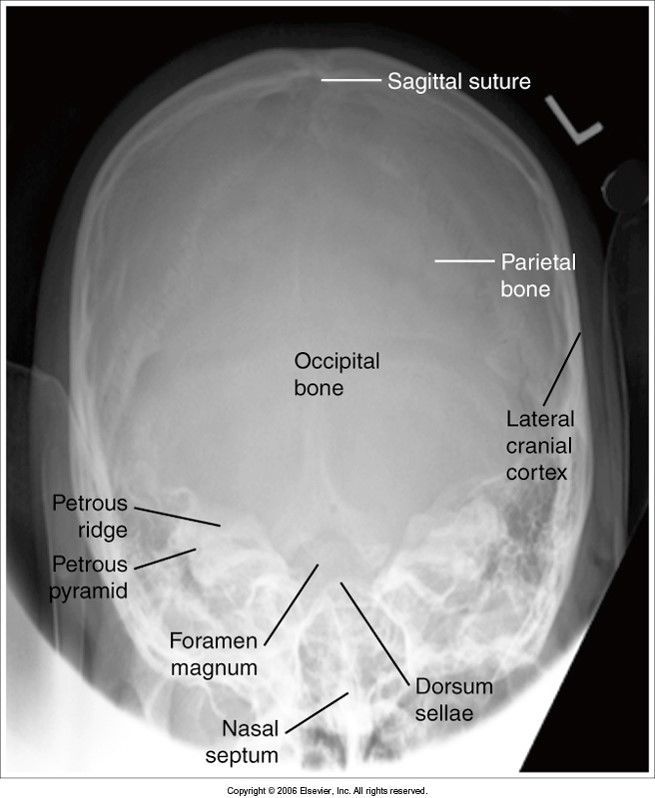
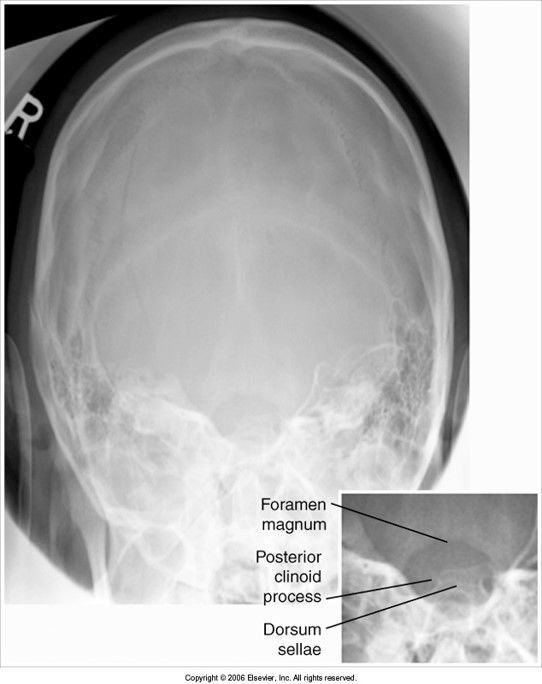
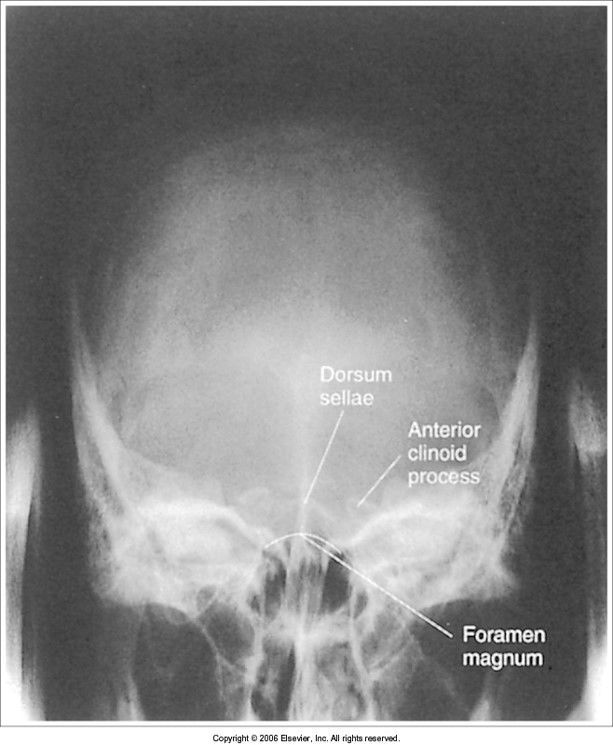
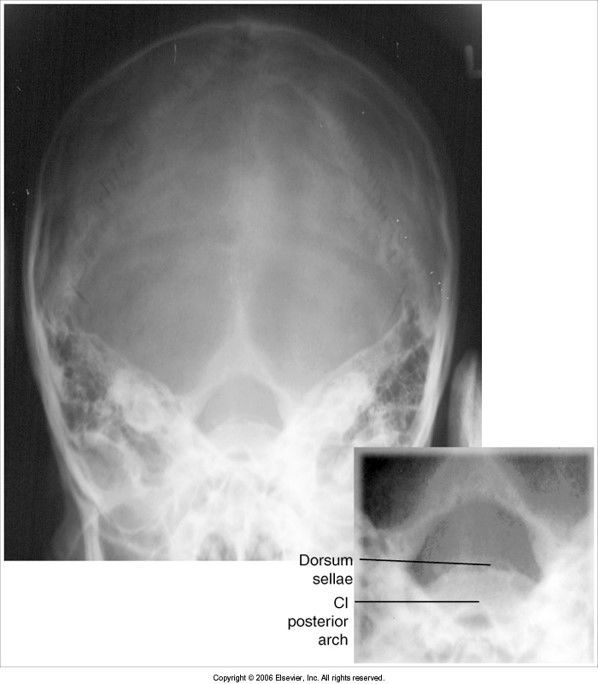
AP Axial Towne Method
evaluation criteria
Image:
Ap Townes (image/jpeg)
|
dorsum sellae is seen within the foramen magnum petrous pyramids are symmetric |
| dorsum sellae is off center to the right: patient's face is turned to the left | |
| dorsum sellae is not within foramen magnum head is not flexed enough OR we need more tube angle | |
| posterior arch of C1 is seen within foramen magnum: head is over flexed, OR the tube angle is too caudal | |
|
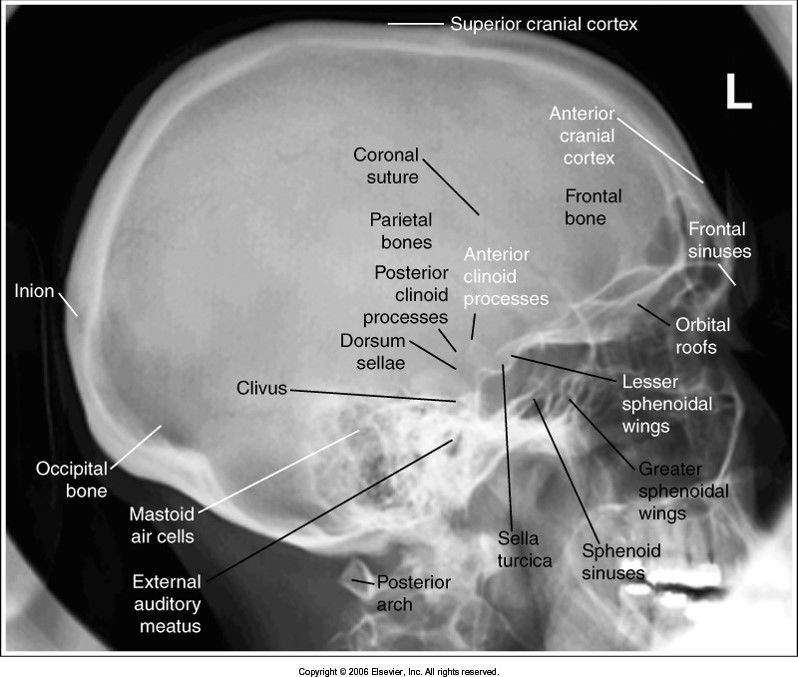
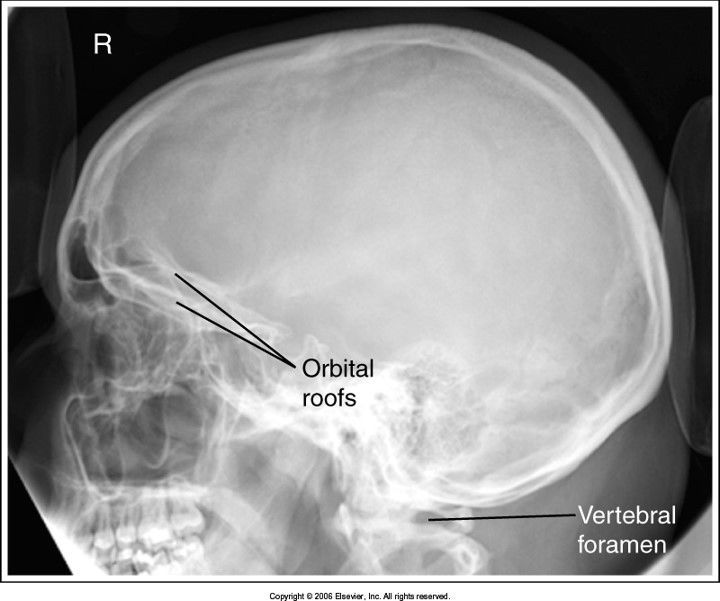
Lateral Skull
evaluation criteria
Image:
Lateral Skull (image/jpeg)
|
superimposed facial bones sella turcica and clivus are in profile |
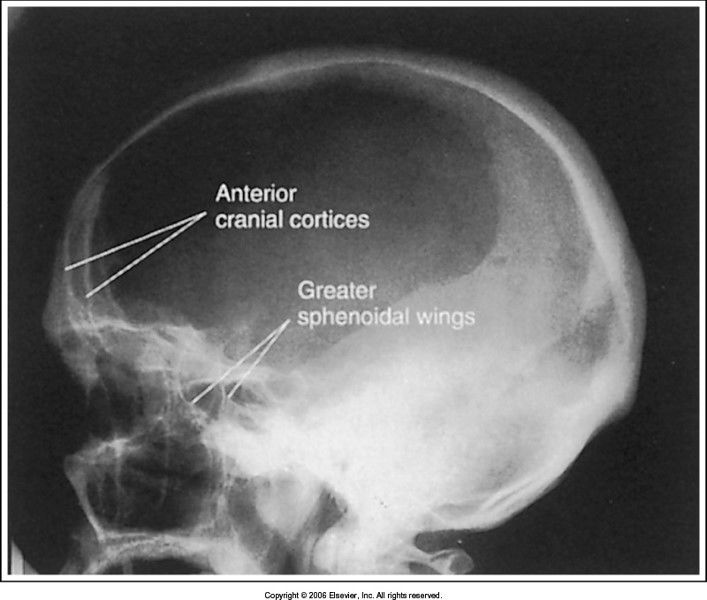
|
Image:
Lat Skull Tilt (image/jpeg)
|
structures aren't superimposed vertically TILT |
| facial features aren't superimposed horizontally ROTATION | |
|
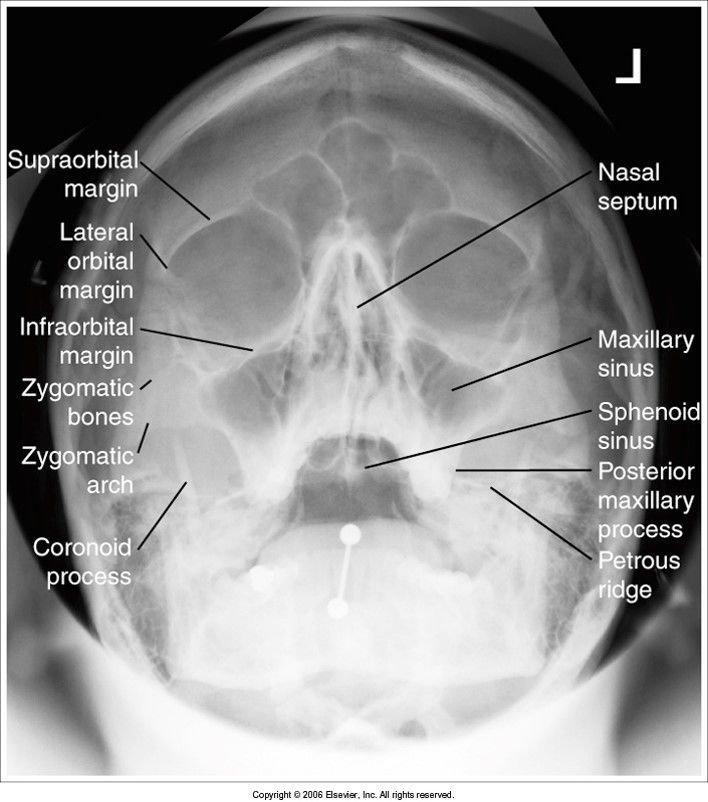
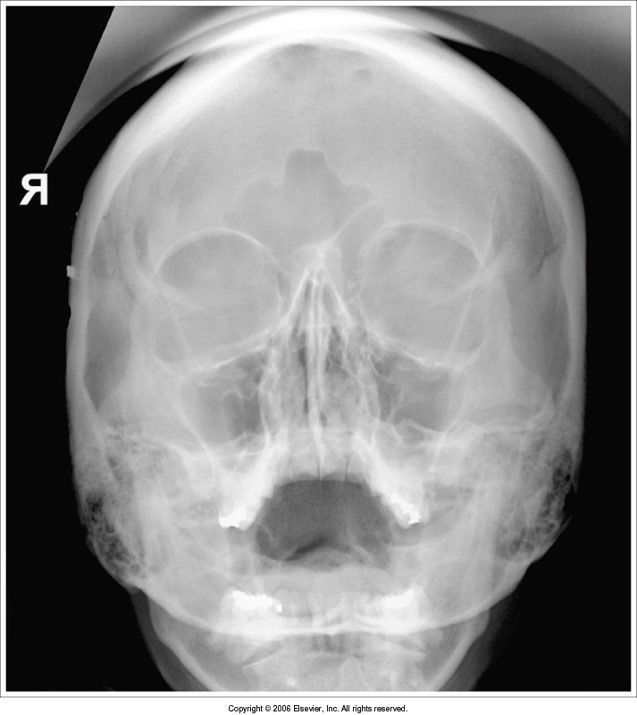
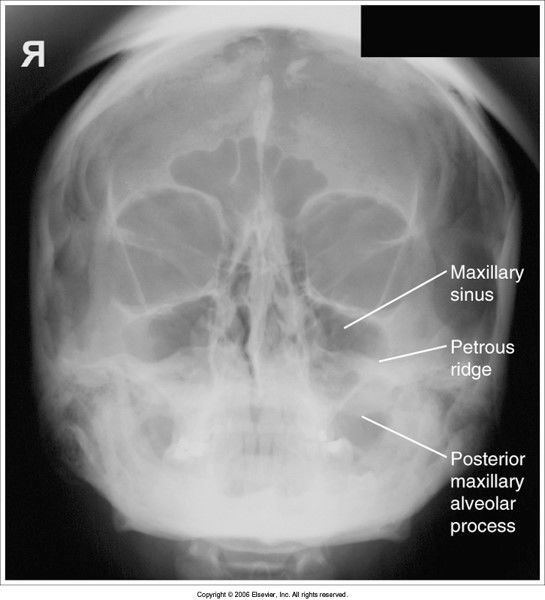
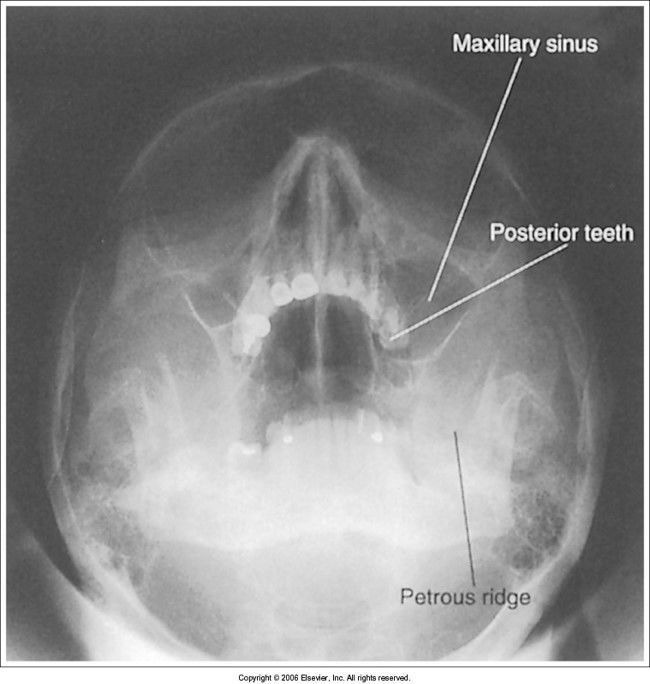
Parietoacanthial Waters
Modified and Transoral
evaluation criteria
Image:
Pa Waters (image/jpeg)
|
PETROUS RIDGES ARE BELOW THE MAXILLARY SINUSES facial features and sinuses are symmetric no rotation SPHENOID sinus is best viewed on the transoral projection MML or LML perpendicular to IR |
| since this is a modified waters view, it's okay that the petrous ridges are within the maxillary sinuses *acceptable image* | |
| standard PA waters: -petrous ridges are within the maxillary sinuses: MML is not perpendicular to IR -head must be extended backward | |
| transoral waters: petrous ridges are low, and upper teeth are in maxillary sinuses head is overextended - flex head forward to bring MML perpendicular to IR | |
| if a patient is rotated with the right side more anterior on the AP C-spine, which SC joint will be lying more over the spine? | Right SC joint *side closest to IR will be open* |
| Which positioning line is used to position the head for the AP c-spine? | AML |
| On this oblique of the c-spine you will see the IVF closest to the IR | RAO/LAO |
| On this oblique of the l-spine, you will see the zygapophyseal joints of the side closest to the IR | RPO/LPO |
| On this view of the t-spine you will see the zygapophyseal joints | Lateral |
| On this oblique of the l-spine, you will see the zygapophyseal joints on the side farthest from the IR | RAO/LAO |
| On this oblique of the c-spine you will see the IVF farthest from the IR | RPO/LPO |
| Which direction will you angle the CR for an AP oblique c-spine? | 15-20 cephalic |
| Which direction will you angle the CR for a PA oblique c-spine? | 15-20 caudal |
| For an oblique c-spine, the _________ obliques provide less absorbed dose to the thyroid gland | anterior |
| how can you determine if there was a tube angle on an oblique c-spine projection? | the disc spaces will be open but the IVF will be closed |
| On a lateral c-spine, if the head is tilted towards the IR we will see the .... | vertebral foramen of C1 |
| On a lateral c-spine, if the head is tilted away from the IR, we will see ..... | posterior arch of C1 still in profile, but the rami of the mandible are not superimposed and the base of the skull |
| On the AP open mouth projection of the c-spine, the teeth are superimposing the dens. How do we correct this problem on the repeat image? | extend head back |
| On the AP open mouth projection of the c-spine, the base of the skull is superimposing the dens. What will we do on the repeat? | flex head forward |
| how can you determine which side was rotated more anteriorly on a lateral lumbar/lateral L5-S1? | the femoral heads should be superimposed. The side that is farther from the IR will be more magnified if the magnified femoral head is more anterior, the patient is rotated |
| There's trauma and you need to do a PA Caldwell skull projection. You can't get the OML perpendicular to the IR because of the C-collar. What will you do? | angle your CR perpendicular to the OML, (caudal if PA, cephalic if AP) then add an additional 7 degrees to the tube angle |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.