6635871
Description
Flashcards by Liam Musselbrook, updated more than 1 year ago
|
|
Created by Liam Musselbrook
about 8 years ago
|
|
| Question | Answer |
| Viruses causing bronchiolitis | RSV (75-80%) Adenovirus Influenza Parainfluenza Metapneumovirus |
| Symptoms of bronchiolits | Cough (dry and persistant) Coryza Apnoea Poor feeding Increased work of breathing |
| Signs of bronchiolits | Low oxygen saturations Fine end-inspiratory crackles Wheeze |
| Investigations and management for bronchiolitis | Inv: Pulse oximetry, NPA, Fluid balance Management: SUPPORTIVE - Oxygen & Feeding |
| Paluvizumab | Monoclonal antibody Passive immunity Given to those at risk Monthly for 5 months over winter period Expensive! |
| Presentation of viral wheeze | Coryza Cough Fever Decreased oral intake Increased work of breathing Wheeze |
| Management of viral wheeze | Oxygen Inhalers/ nebulisers Salbutamol Atrovent CXR Prednisolone Antibiotics Montelukast |
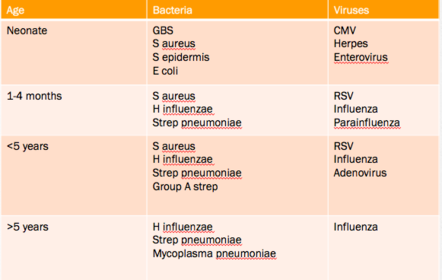
| Pneumonia-causing organisms in children | |
| Symptoms and signs of pneumonia | Fever Cough, Grunting Increased respiratory effort/ distress Poor feeding Lethargy Reduced air entry Crackles Dullness to percussion |
| Investigations for pneumonia | NPA CXR Bloods Blood culture Sputum culture |
| Management of pneumonia | Oxygen Hydration Antibiotics (Oral or IV?) Chest drain |
| Causes/RF for recurrent pneumonia | Cystic fibrosis Immune deficiencies HIV / AIDs Kartagener’s syndrome Reccurent aspiration, Reflux Foreign body Tracheoesophageal fistula CLD |
| Common cause and common age range for croup? | 75% cases parainfluenza 6months - 6years Peak incidence is in the second year of life |
| Presentation of croup | Barking cough Coryza Hoarse voice Stridor |
| Differential diagnoses for croup | Epiglottitis Bacterial tracheitis Inhaled foreign body Angioedema |
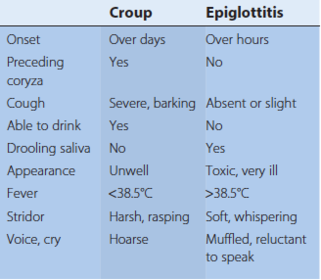
| Clinical features of croup vs epiglottitis | |
| Management of croup | CALMING ENVIRONMENT Airway management- do you need an anaesthetist? Oxygen Oral dexamethasone and prednisalone Nebulised budesonide Nebulised adrenaline Watch for rebound |
| Whooping cough: age, organism and immunisation | <5 years Bordetella pertussis Immunised antenally Immunised 2, 3, 4 months |
| Presentation of whooping cough | Coryza Paroxysms/ spasms of cough Followed by an inspiratory whoop (often absent in small children) 49 Apnoea Cyanotic episodes Can last up to 10-12 weeks |
| Management of whooping cough | Perinasal swab Supportive Erythromycin (doesn't alter course of illness in active infection, use to reduce spread) |
| Mild/moderate acute asthma | Able to talk in full sentences Sats: ≥92% PEF: ≥50% best or predicted HR: ≤140 age 2-5, ≤125 >5 yrs RR: ≤40 2-5 yrs, ≤30 >5 yrs |
| Moderate/sever acute asthma | Can't complete full sentence Sats: <92% PEF: 33-50% of best or predicted HR: >140 2-5yrs, >120 >5yrs RR: >40 2-5yrs, >30 >5yrs |
| Life-threatening | Cyanosis Sats: <92% in air Silent chest Poor respiratory effort Fatigue or exhaustion Agitation or reduced level of consciousness |
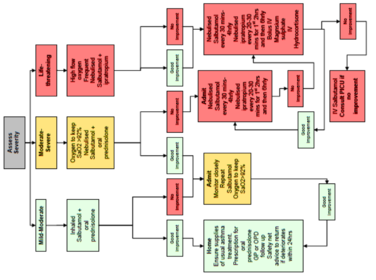
| Draw the treatment flowchart for acute asthma | |
| Management of asthma in < 5yrs | SABA when required Step 1) Very low dose inhaled corticosteroid Step 2) Add a leukotriene receptor antagonist Step 3) Refer to a paediatric specialist, possibly inhaled steroids to low-dose Step 4) Consider trials of either: - increasing the ICS to medium-dose, or - addition of a fourth drug - SR theophylline Step 5) Consideration of regular oral steroids |
| Algorithm of management of chronic asthma 5-12yrs | SABA when required 1) Very low dose inhaled corticosteroid 2) LABA 3) No response to LABA - stop LABA and increase dose of ICS to low-dose Response to LABA - continue LABA and increase ICS to low-dose/consider leukotriene receptor antagonist 4) Consider trials of either: - increasing the ICS to medium-dose, or - addition of a fourth drug - SR theophylline Refer to paediatric specialist 5) Consider oral steroids |
| Newborn and infant clinical features of Cystic Fibrosis | Newborn: Diagnosed through newborn screening Infancy: • Meconium ileus in newborn period • Prolonged neonatal jaundice • Failure to thrive • Recurrent chest infections • Malabsorption, steatorrhoea |
| Diagnosis of Cystic Fibrosis | Cl >60 mmol/L in sweat test Confirmation of diagnosis can be made with testing for gene abnormalities in the CFTR protein. |
| Respiratory management of CF | Regular spirometry Physiotherapy Prophylactic antibiotics Nebulised DNAse or hypertonic saline |
| Nutritional management of CF | Oral enteric-coated pancreatic replacement therapy (Creon) High-calorie diet Fat-soluble vitamin supplements |
| Problems teenagers with CF face | Diabetes Liver disease Distal intestinal obstruction syndrome Male infertility Psychological issues |
| Screening for CF | Immunoreactive trypsinogen (ITP) with heel-prick blood test (Guthrie test) |
| Pharyngitis (*in older children, what is a common pathogen? | Sore throat Pharynx and soft palate are inflamed and local lymph nodes are enlarged and tender Mostly adenoviruses, enteroviruses and rhinoviruses Oder child, group A β-haemolytic strep = common pathogen |
| Centor criteria for tonisillitis | Tonsillar exudate Tender anterior cervical adenopathy Fever over 38°C by history Absence of cough 3 or 4 of Centor criteria are met, the positive predictive value is 40% to 60% Absence of 3 or 4 has negative predictive value of 80% |
| Common pathogens for tonsillitis | Group A β-haemolytic strept Ebstein-Barr (infectious mononucleosis) |
| Antibiotic therapy for tonsillitis | Often given despite only 1/3 tonsiliitis caused by bacteria Penicillin (erythromycin if penicillin allergy) Amoxicillin best avoided -> widespread rash if Ebstein-Barr is cause |
| How long is treatment required for in order to ensure prevention of rheumatic fever? | 10 days Not indicated in the UK where rheumatic fever is now exceedingly rare. |
| What is the criteria for tonsillectomy? | Sore throats are due to acute tonsillitis. The episodes of sore throat are disabling and prevent normal functioning. Seven or more well-documented, clinically significant, adequately treated sore throats in 1 year; or five or more in 2 years; or three or more in 3 years A peritonsillar abscess (quinsy) Obstructive sleep apnoea (the adenoids will also normally be removed) |
| At what age is otitis media most common? | 6-12 months |
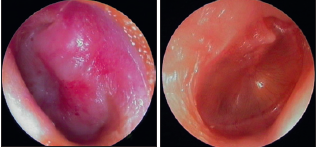
| Clinical features of acute otitis media | Otalgia Fever Tympanic membrane is seen to be bright red and bulging with loss of the normal light reflection Occasionally, there is acute perforation of the eardrum with pus visible in the external canal. |
| Image of (left) acute otitis media and (right) AOM with effusion | |
| Common pathogens of acute otitis media | Viral -RSV and rhinovirus, Bacterial - pneumococcus, nontypeable H. influenzae and Moraxella catarrhalis. |
| Treatment of acute otitis media | Most spontaneously resolve Pain should be treated with regular paracetamol or ibuprofen Antibiotics - marginally shorten duration of pain but don't affect hearing loss, often useful to give the parents a prescription, but ask them to use it only if the child remains unwell after 2–3 days. Amoxicillin usually |
| Otitis media with effusion (OME) | Caused by recurrent ear infections Eardrum is seen to be dull and retracted, often with a fluid level visible Conductive hearing loss Very common between the ages of 2 and 7 years, peak incidence 2.5-5 years Can interfere with normal speech development and result in learning difficulties in school |
| Management of OME | Usually conservative If it doesn't resolve then insertion of grommets is indicated If problems recur after grommet extrusion, reinsertion of grommets with adjuvant adenoidectomy is usually advocated |
| Sinusitis | Infection of the paranasal sinuses may occur with viral URTIs. Secondary bacterial infection - pain, swelling and tenderness over the cheek from infection of the maxillary sinus Antibiotics + analgesia + topical decongestants |
| Indications for adenoidectomy + tonsillectomy | Recurrent otitis media with effusion with hearing loss, where it gives a significant long-term additional benefit, especially if reinsertion of grommets is considered Obstructive sleep apnoea (an absolute indication) |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.